PEDIATRIC SURGERY2018 4 No Attendance Obligatory Type of

PEDIATRIC SURGERY-2018 4 No. : Attendance: Obligatory Type of lecture: theory Place : Hall no. 4 college of medicine –Mustansiriyah University. Date : Monday 5 th of March 2018. Time : 8: 00 – 9: 00 AM. Students: 4 th year / college of medicine / Mustansiriyah University By : Dr. Ali E. Joda M. B. Ch. B. - F. I. C. M. S. - pediatric surgeon. E. mail : ali. egab. joda@uomustansiriyah. edu. iq

• Objectives: What is the field of pediatric surgery & how it differs from general surgery? By the end of this lecture, you have to be able to recognize the main features of neonatal intestinal obstruction & how you can approach to infant with this problem. What is atresia & where it could be occur in gastrointestinal tract? How can you differentiate it from other causes of intestinal obstruction like malrotation of midgut & meconium ileus. What are the main lines of treatment?

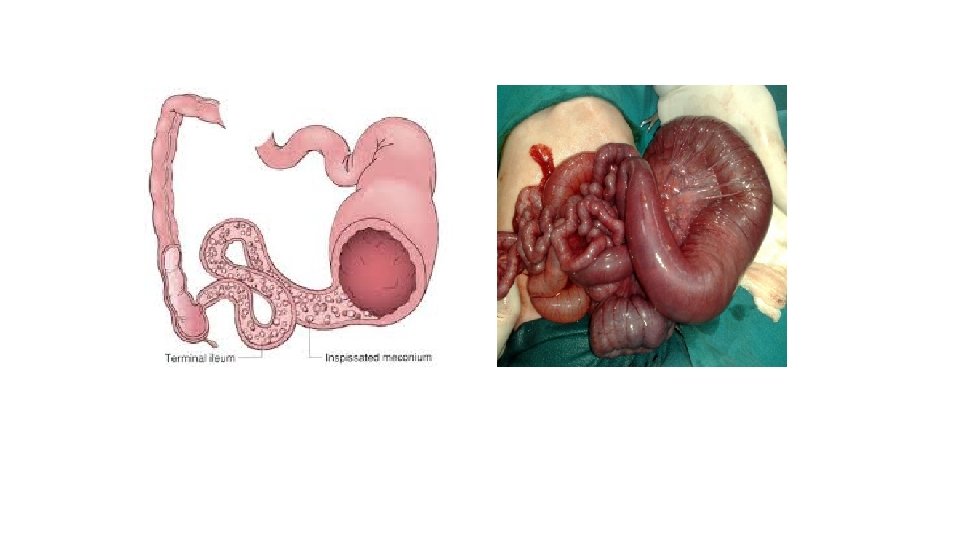
Meconium ileus is really a wrong name because it is intestinal obstrucrtion due to mechanical obstruction (inspissated meconium) in the terminal ileum due to abnormal composition of fetal meconium due to cystic fibrosis. Pathophysiology : - Cystic fibrosis is autosomal recessive disease result from mutation (F 508 del mutation) in the gene termed cystic fibrosis transmemebrane regulater (CFTR gene) responsible for coding cell membrane protein 3 -, 5 - c. AMP, which regulate the flow of ions across the epithelial surfaces , so its defect will lead to abnormal electrolyte composition on the epithelial membranes. it affect the respiratory tract , pancreas , & the gastrointestinal tract. The fetal meconium will have less water content, less pancreatic enzyme, sucrase , lipase, but more protein & albumin so it will be extremely viscid , thick & dehydrated. This meconium will obstructs the terminal ileum.

Presentation : Simple meconium ileus : like any neonatal I. O , failure to pass meconium , progressive abdominal distension , bilious vomiting. Dilated bowel loops which become visible on examination & have doughy character & indents on palpation. Complicated meconium ileus : volvulus , intestinal atresia , intestinal necrosis , perforation , & meconium peritonitis.

Diagnosis : o Plain abdominal X-ray : dilated bowel loops , air-fluid levels , soapbubble appearance (air mixed with tenacious meconium) , peritoneal calcification , peumoperitonium. o Contrast enema (water soluble - gastrografin) : (it is diagnostic) microcolon of disuse , containing small rabbit pellets of inspissated mucus. Abdominal ultrasound : ascites , intra-abdominal mass (meconium pseudocyst) , calcification.

Treatment : Resuscitation : IVF , NG decompression , antibiotic coverage , vitamin K to correct any coagulopathy. Non-operative management: - (only for uncomplicated meconium ileus) Using hyperosmolar water soluble enema (gastrografin) under fluoroscopic control through catheter inserted into the rectum , the hyperosmolar gastografin will hydrates & softens the meconium mass result in passage of semiliquid meconium. Sometimes we use 10% N-acetylcysteine solution through NG tube to liquefy upper gastrointestinal secretion. The success rate of non-operative treatment range from 63 -83 % but it has potential risk of : (1) rectal perforation. (2) dehydration & hypovolaemic shock. (3) necrotizing enterocolitis.

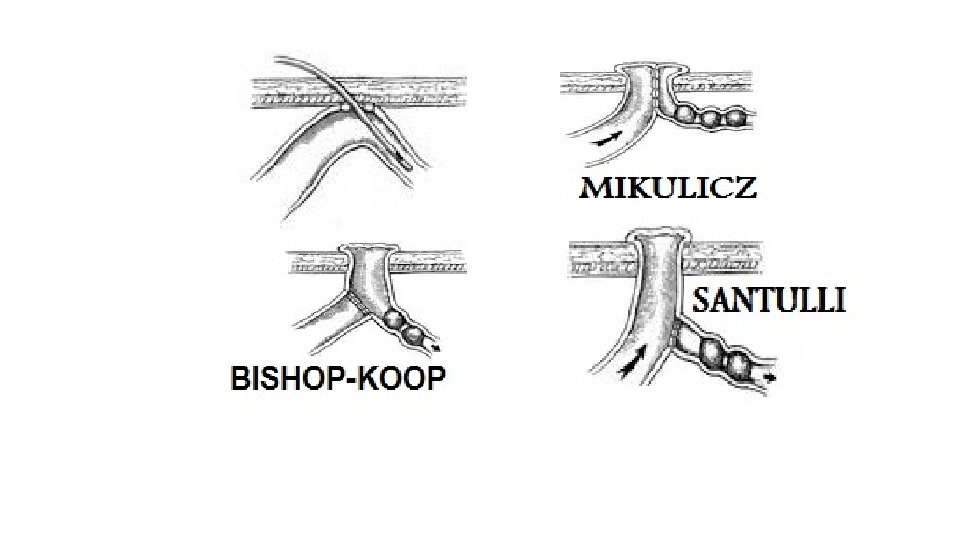
Operative management : Indications : In simple meconium ileus : inadequate evacuation of meconium. In simple meconium ileus : complication of gastrografin enema. In complicated meconium ileus. Surgical options : 1. Tube enterostomies (T-tube). 2. Resection & anastomosis. 3. resection & enterostomy : A. Double parrelled enterostomy (Mikulicz ). B. Distal chimney enterostomy (Bishop – koop). C. Proximal enterostomy (santulli).

Postoperative period : Nutritional management after relief of obstruction & resumption of bowel function, infant with uncomplicated MI & CF can start breast milk or routine infant formula with supplemental pancreatic enzyme 2000 – 4000 IU lipase per 120 ml formula. (((((((((((((((((((((((End))))))))))))))))))))))))) References: 1. Baily & love's short practice of surgery 26 th edition (2013). 2. Ashcraft's pediatric surgery 6 th edition (2014). 3. Arnold G. Coran pediatric surgery 7 th edition (2014). 4. Newborn surgery 4 th edition (2018). 5. Quick guide to Pediatric surgery (2018).
- Slides: 10