Pediatric Stone Disease Overview Epidemiology 4 Reasons Stones





")
")



 Polinsky 1993; Robertson, 1978, Basaklar,")


 – Mildly radioopaque (cystine) – Radio-opaque (calcium)")












 Inhibitors Tamm-Horsfall")


 – Mg/m")










")








 Other Colonic Pathways Absorption Ox")













 Urease-splitting organisms Collecting system anomalies Stones intrinsically filled with")











- Slides: 82
Pediatric Stone Disease
Overview Epidemiology 4 Reasons Stones Form Diagnostic Tests The Menu of Stones
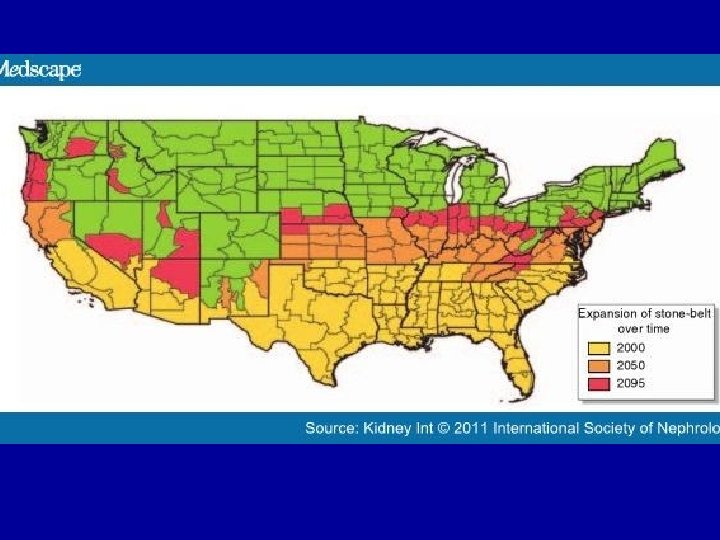
Pediatric Urolithiasis How is it compare to adult stone disease? LESS COMMON th 1/50 the rate No “Stone Belt” Increasing Incidence
GENDER EQUALITY No male predominance
SIMILAR PASSAGE RATES Similar spontaneous passage (8 -50 %)
SIMILAR RECURRENCE Similar Recurrence (~ 50 %)
MORE VARIED CAUSES More secondary etiologies
The Bigger the Stone, The Less Likely it Passes % mm
Presenting Features of Pediatric Stone Disease by Age (Sums exceed 100% due to multiple presenting features) Milliner, Murphy, Mayo Clin Proc, 1993
Primary Etiology of Pediatric Stones (20% have multiple causes) Polinsky 1993; Robertson, 1978, Basaklar, 1991
Types of Pediatric Stones
Acute Management Imaging Decide if Urology needs to be called Pain Control Fluids
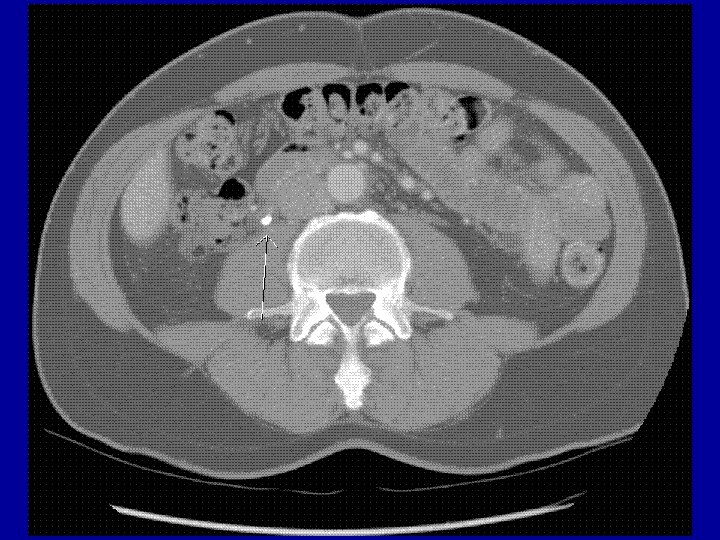
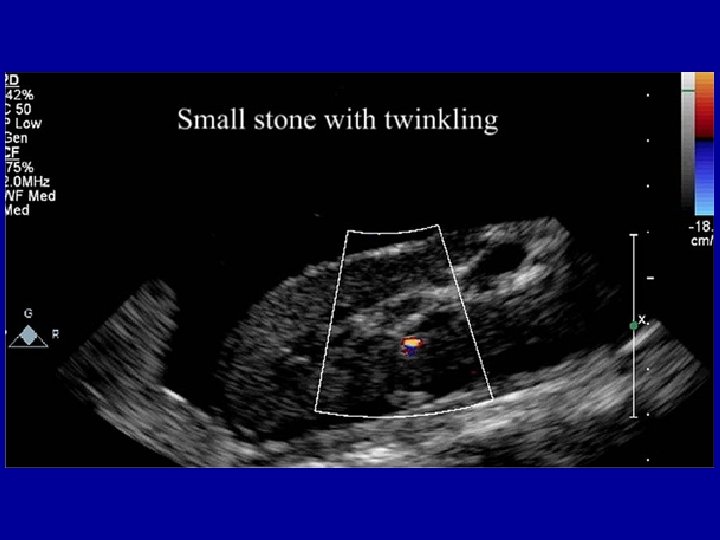
Imaging • X-Ray – Non-radioopaque (uric acid) – Mildly radioopaque (cystine) – Radio-opaque (calcium) • IVP • US • CT Scan – imaging of choice
Non-Medical Treatment • Indications –> 5 mm –Staghorn –Struvite stones –Infection –Obstruction
Acute Management of Stones • Hydration Oral better than IV • Pain Control NSAIDS better than opioids
Use of Alpha Blockers and Stone Passage Rates %
ESWL vs Laser Lithotripsy • ESWL – Pros • Great for Ca. Ox and Urate stones • Non-invasive – Cons • • GETA for kids < 8 y Can’t break up Cystine stones Poor success rate with BIG stones (> 1 cm) Hemorrhage and edema post-ESWL
Overview Epidemiology 4 Reasons Stones Form Diagnostic Tests The Menu Of Stones
The 4 Quadrants of Stone Formation Too Much Solute Too Little Solvent Too Many Promoters Too Few Inhibitors
Too Much Solute Low sodium diet Enhance reabsorption Low dietary intake of solute
Too Little Solvent Most stones prevented 2 with > 2 L/m /day
Too Many Promoters p. H Uric Acid
p. H and Stone Risk High p. H Ca. PO 4 Struvite Low p. H Ca. Ox Uric Acid Cysteine
Most important inhibitors Too Few Inhibitors Citrate Magnesium Natural (but clinically insignificant) Inhibitors Tamm-Horsfall Protein Osteopontin Prothrombin fragment 1
Lemonade Therapy • 4 oz of lemon juice in 2 Liters of water • Can restore normal citrate levels Urology, 2007
Overview Epidemiology 4 Reasons Stones Form Diagnostic Tests The Menu Of Stones
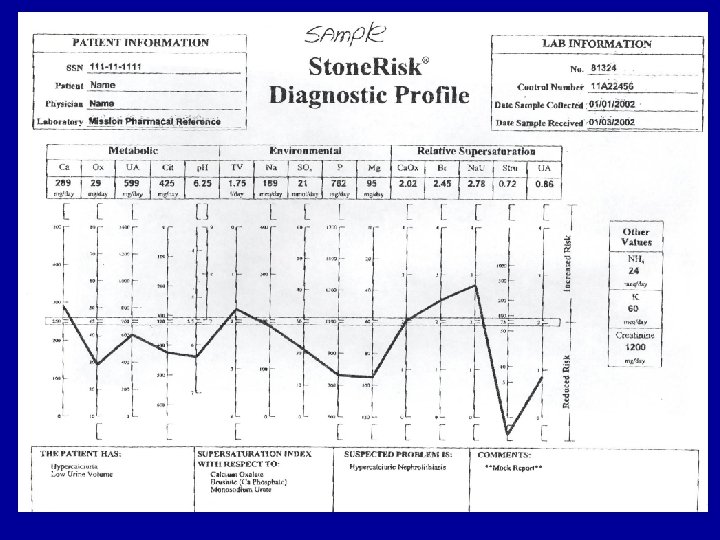
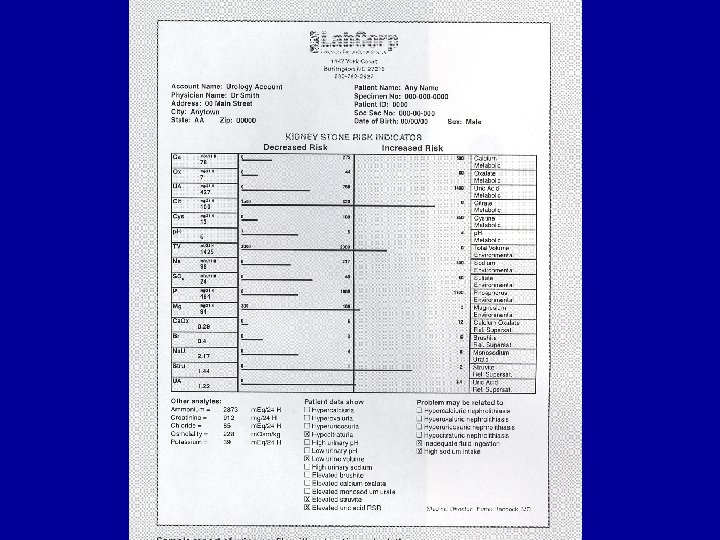
Timed Urine Collection • A variety of units – Mg/kg/day (calcium, magnesium) – Mg/m 2/day (oxalate) – Mg/1. 73 m 2/day (uric acid) – Mg/g creatinine (cystine, citrate) • Other measures – saturation indices – Mg/Ca and Citrate/Ca ratios
What’s So Special About the Orange Jug? • Thymol – prevents change in p. H, citrate, uric acid, sulfate, sodium, potassium, and c. AMP • HCl or Boric Acid – prevents change in Ca, Mg, PO 4, Ox, ammonium, creatinine
Spot Urine Solutes • Solute : Creatinine – Ca / Cr < 0. 22
Urinalyses: Crystals
Diamonds
Uric Acid Crystals Pink Junk
Coffin Lids
Hexagons
Spectroscopy of Stone
Overview Epidemiology 4 Reasons Stones Form Diagnostic Tests The Menu Of Stones
A MENU OF STONE DISEASES Look what I passed!
Hypercalciuria Facts • 50% of identified metabolic abnormalities – 50% are inheritied (Autosomal Dominant) • 10 -16% of untreated kids get stones in 1 -4 y – 72% within 15 yrs (retrospective Hungarian) • Idiopathic #1 cause – Renal or GI subtypes (clinically unimportant) • 70% of kids have + Family Hx • Can be associated with low bone density
Secondary Causes of Hypercalciuria • Ketogenic Diet • Vitamin D intoxication • Medication (steroids, loop diuretics) • • • Immobilization Acidosis Hypercalcemia Thyroid disorders Dent’s Disease d. RTA Ca. SR Mutations Familial hypomagnesemia-hypercalciuria Bartter’s syndrome • Medullary Sponge Kidney
Medullary Sponge Kidney
Upper Limit of Normal for Spot Ca: Cr Ratios
Nephrocalcinosis in Preemies 16 -64 % of infants < 1500 g / < 32 wks GA 50% resolve Etiologies - diuretics - immature tubular function - TPN - differences in urinary solute handling
Hypercalciuria Treatments Too Much Solute Low Sodium Diet Thiazide Diuretics Amiloride Low Oxalate Diet High Fiber Diet Low Protein Diet* Too Little Solvent Increase water intake (2 L / m 2 / day) Too Little Inhibitors Potassium Citrate Lemonade Neutral orthophosphate Too Many Promoters Neutral or Alkaline p. H
Cystinuria • Tubular defect of dibasic amino acid uptake – COLA amino acids • Presents with stones • Only homozygous patients affected • No generalized aminoaciduria and hexagonal crystals in urine
Cystine Stones
Cystinuria Treatments Too Much Solute Too Little Solvent Too Little Inhibitors Too Many Promoters Penicillamine, tiopronin, MPG or captopril Low methionine diet* Increase water intake (4 L / m 2 / day) Get U-Cys < 250 mg/L Potassium Citrate Lemonade Alkalinization (Potassium Citrate)
Oxalate Metabolism Vitamin C Glycine AGT (B 6 cofactor) Other Colonic Pathways Absorption Ox Glomerular Filtration Diet
Dietary Oxalate • 10 -20% of urinary oxalate is dietary in origin • Mostly in plants • Only 2 -14% is absorbed – Based on concurrent calcium intake – Based on Oxalobacter activity • Absorbed everywhere in GI tract • Colon can excrete oxalate in ESRD (angiotensin mediated; blocked by ARBs)
Enteric Hyperoxaluria • Colonic hyperabsorption with small bowel disease – Crohn’s Disease – Cystic Fibrosis • Depletion of Oxalobacter with chronic antibiotics
Oxalobacter formigenes 70% reduction in Ca-Ox stones based on colonization status JASN, 2008
Primary Hyperoxaluria Type 1 – AGT Deficiency Type II – Alternate oxalate pathway (milder form) Usually present with Urolithiasis in childhood can present with nephrocalcinosis or ESRD Progressive chronic kidney disease Elevated urine oxalate and glycolate Flecked retina May respond to Pyridoxine
These are all high oxalate produce. Which has the most oxalate? (HINT: It’s oxalate load is its only renal claim to fame. )
High Oxalate Foods • • • Plums Cocoa • Parsley Tea • Asparagus • Currants Rhubarb • Cranberries • Oranges • Grapefruit Spinach • • Pepper Peanuts Beets Starfruit S. T. A. R.
Primary Hyperoxaluria Treatments Too Much Solute Pyridoxine Chlorathiazide Increase water intake (3 L / m 2 / day) Too Little Solvent Too Little Inhibitors Magnesium Hydroxide or Gluconate Neutral Orthophosphate -- Too Many Promoters
Enteric Hyperoxaluria Treatments Too Much Solute Cholestyramine Low Oxalate Diet Calcium Citrate Oxalobacter formigenes Too Little Solvent Increase fluid intake ( 2 L / m 2 / day) Too Little Inhibitors Calcium or Potassium Citrate Lemonade Mg Hydroxide -- Too Many Promoters
Uric Acid Stones 5 -8% of pediatric stones Non-radioopaque Causes of hyperuricosuria - Idiopathic Ketogenic Diet Pancreatic Enzymes heme malignancies Lesch-Nyan Tumor Lysis Syndrome Diarrheal states ASA or probenicid therapy
Hyperuricosuria Treatments Too Much Solute Too Little Solvent Too Little Inhibitors Too Many Promoters Allopurinol Low protein intake* Increase water intake (2 L / m 2 / day) Potassium Citrate Lemonade Alkalinization
Medicine Stones Triamterene Ephedrine Phenytoin Indinavir Nelfinavir Sulfadiazine Amorphous silica Ceftriaxone Ampicillin Amoxicillin Robitussin
Bizarre & Unusual Stones & Crystals Ethylene Glycol Tyrosine Massive tissue breakdown Ammonium Urate Poisoning Leucine Massive tissue breakdown Porto-systemic shunts or Dalmation or English Bulldog ancestry
Melamine Stones in China • Added to infant formula in 2008 • 300, 000 affected – > 50, 000 infant hospitalizations – 6 infant deaths
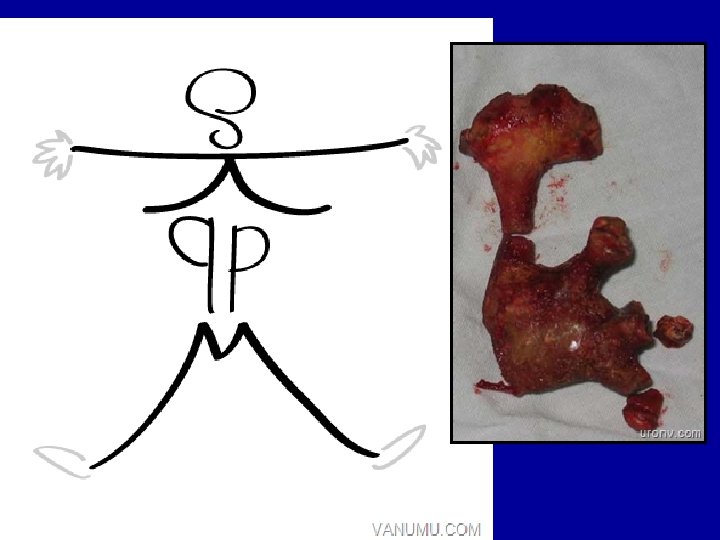
Struvite Stones (Mg Ammonium Phosphate) Urease-splitting organisms Collecting system anomalies Stones intrinsically filled with bacteria #1 cause of staghorn calculi Treatment requires removal of stones
Struvite Stone Treatments Too Much Solute Removal of any stones Too Little Solvent Increase water intake (2 L / m 2 / day) Too Little Inhibitors Too Many Promoters Acetohydroxamic acid (urease inhibitor; many AEs)
Question # 1 All of the following predispose to stone formation except: A. Low urine volume B. Hypocitraturia C. Hypermagnesuria D. Medullary Sponge Kidney
Question # 2 An 8 y/o male with Lesch-Nyan syndrome was recently evaluated for abdominal pain. Plain abdominal X-ray was reported as normal. An US revealed a 6 mm stone in the left renal pelvis and no hydronephrosis. What is the appropriate management? A. Increased fluid intake & alkalinization B. Therapy with allopurinol C. Removal of the stone D. Follow up radiograph
Question # 3 Which of the following bacteria is associated with stone formation? A. E. coli B. Proteus C. Pseudomonas D. Enterobacter
Question # 4 A 10 y/o girl is seen in the ED With acute left renal colic. U/a shows 120 rbc/hpf, Trace protein and numerous hexagonal crystals. Which is true of this clinical condition? A. It is transmitted by autosomal dominant inheritance B. Urinary ornithine is elevated C. Stones are radiolucent D. White cell cystine is elevated
Question # 5 All are true of idiopathic hyper. Calciuria except: A. 24 hr urine collection is not necessary for diagnosis B. It may be absorptive or renal type C. May be a result of immobilization D. It is exacerbated by dietary protein
Question # 6 A 4 y/o boy is evaluated for persistent microscopic hematuria. Labs are normal except for a random urine Ca/Cr ratio of 0. 5 and a 24 hr urine Ca excretion of 6 mg/kg/day. Treatment may include all of the following except: A. Dietary Calcium restriction B. Hydrochlorathiazide C. Salt restriction D. Neutral orthophosphate
Question # 7 All of the following are true of Primary Hyperoxaluria except A. Elevated urine glycolate in Type I B. Urinary oxalate is usually higher is Type I than Type II C. ESRD in common in Type I D. Vitamin C therapy is helpful
Question # 8 Routine U/A in a 17 y/o male with Crohn’s Disease reveals microscopic hematuria. U/S shows bilateral renal stones. Which of the following is likely true in this patient? A. The stones are most probably Ca. PO 4 B. Urinary oxalate excretion is low C. Treatment includes calcium supplements D. Pyridoxine therapy is helpful
Question # 9 All are true of ESWL except: A. The bigger the stone, the more successful the procedure B. It may cause renal hemorrhage and edema C. It is contraindicated if the urinary tract is obstructed D. GETA is required in smaller children