Pediatric Lumbar OMT Module l l American College

Pediatric Lumbar OMT Module l l American College of Osteopathic Pediatricians Robert Hostoffer, DO, FACOP, FAAP edited by Eric Hegybeli, DO, FACOP

Background: Andrew Taylor Still, was born in Virginia in 1828, the son of a Methodist minister and physician. At an early age, Still decided to follow in his father's footsteps as a physician. After studying medicine and serving an apprenticeship under his father, Still became a licensed M. D. in the state of Missouri. Later, in the early 1860's, he completed additional coursework at the College of Physicians and Surgeons in Kansas City, Missouri. He went on to serve as a surgeon in the Union Army during the Civil War.

Background: l After the Civil War and following the death of three of his children from spinal meningitis in 1864, Still concluded that the orthodox medical practices of his day were frequently ineffective, and sometimes harmful. He devoted the next ten years of his life to studying the human body and finding better ways to treat disease.

Background: His research and clinical observations led him to believe that the musculoskeletal system played a vital role in health and disease and that the body contained all of the elements needed to maintain health, if properly stimulated. Still believed that by correcting problems in the body's structure, through the use of manual techniques now known as osteopathic manipulative treatment, the body's ability to function and to heal itself could be greatly improved. He also promoted the idea of preventive medicine and endorsed the philosophy that physicians should focus on treating the whole patient, rather than just the disease. l http: //www. aacom. org/OM/history. html

Toddler and Children OMT

Muscles of the back
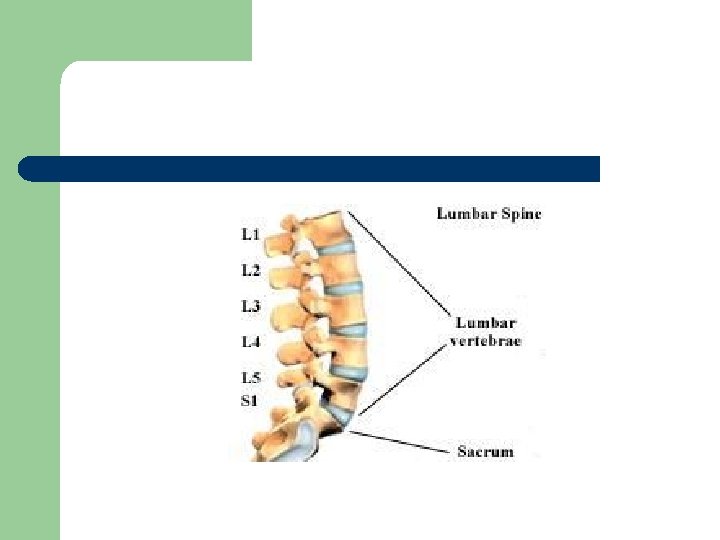

Lumbar Spine Vertebrae

Contributions to Lumbar Somatic Dysfunction l l l Sacral base unleveling Psoas spasm Short leg Scoliosis Spondylolisthesis Spondylolysis

Pediatric Lumbar Considerations l l Toddlers naturally have an increased lumbar lordosis because of inadequately developed abdominal musculature Children with lumbar somatic dysfunction will have a positive hip drop test on the affected side

Myofascial Stretching l Patient is prone. Place thumb onto paraspinal muscles adjacent to the vertebral spinous process. In a bowing like motion stretch the muscles away from you and release. Perform slowly.
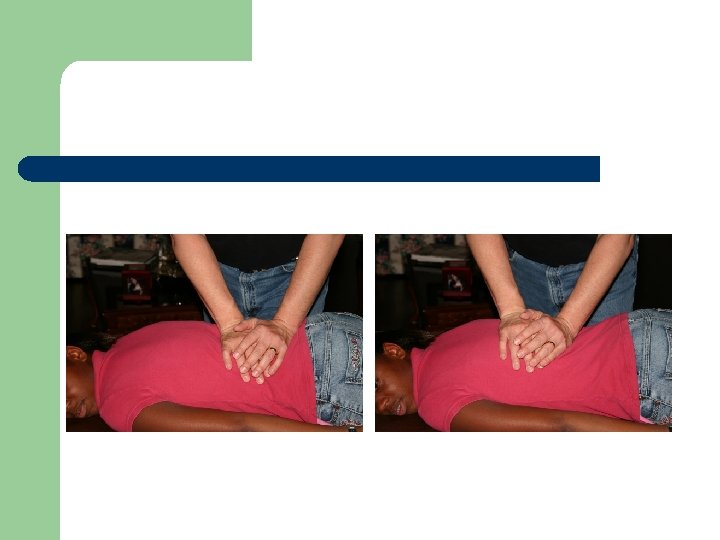

Demonstrate the procedure on patient in front of director

Lumbar rotation technique l Patient is supine. Have the patient lace fingers behind head. Standing to the side of the patient grab the patient’s contra lateral upper arm and pull toward you and caudally.

Demonstrate the procedure on patient in front of director

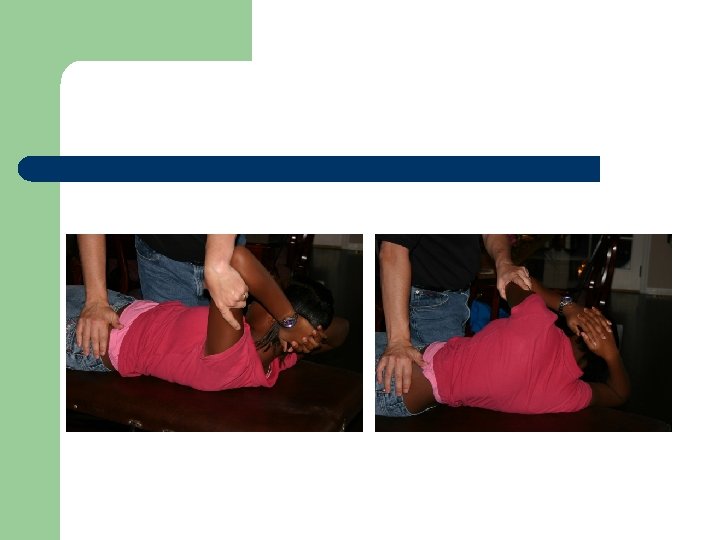
Lumbar Mobilization l The patient is in the lateral recumbent position. The side that the dysfunctional vertebra is rotated towards is up (eg, for a left rotated lumbar, the patient is lying on their RIGHT side). The patients upper most leg is dropped over the side of the table. The patients upper elbow is flexed. The lower elbow is also flexed and the arm is tucked under the head. Stand to the side of the patient with his/her face to you. Your one arm should be placed onto the upper elbow and the other arm placed on the upper hip. A twisting motion is performed by moving the patients elbow backward and the patient’s upper hip forwards, carrying the dysfunctional vertebra into correct position


Demonstrate the procedure on patient in front of director

Innervation Table Organ/System EENT Parasympathetic Sympathetic Ant. Chapman's Post. Chapman's T 1 -T 4 T 1 -4, 2 nd ICS Suboccipital Heart Cr Nerves (III, VII, IX, X) Vagus (CN X) T 1 -T 4 T 3 sp process Respiratory Vagus (CN X) T 2 -T 7 T 1 -4 on L, T 23 rd 3 & 4 th ICS Esophagus Vagus (CN X) T 2 -T 8 --- T 3 -5 sp process --- Foregut Vagus (CN X) T 5 -T 9 (Greater Splanchnic) --- Stomach Vagus (CN X) T 5 -T 9 (Greater Splanchnic) Liver Vagus (CN X) Gallbladder T 6 -7 on L T 5 -T 9 (Greater Splanchnic) 5 th-6 th ICS on L Rib 5 on R Vagus (CN X) T 5 -T 9 (Greater Splanchnic) Rib 6 on R T 6 Spleen Vagus (CN X) T 5 -T 9 (Greater Splanchnic) Rib 7 on L T 7 Pancreas Vagus (CN X) Rib 7 on R T 7 Midgut Vagus (CN X) T 5 -T 9 (Greater Splanchnic), T 9 T 12 (Lesser Splanchnic) Thoracic Splanchnics (Lesser) Small Intestine Vagus (CN X) T 9 -T 11 (Lesser Splanchnic) Ribs 9 -11 T 8 -10 Tip of 12 th Rib T 11 -12 on R Appendix Hindgut Ascending Colon Transverse Colon T 12 Pelvic Splanchnics (S 24) Vagus (CN X) Lumbar (Least) Splanchnics T 9 -T 11 (Lesser Splanchnic) T 5 -6 --- --- --T 10 -11 T 9 -T 11 (Lesser Splanchnic) R Femur @ hip Near Knees L Femur @ hip T 12 -L 2 Descending Colon Pelvic Splanchnic (S 2 -4) Least Splanchnic Colon & Rectum Pelvic Splanchnics (S 24) T 8 -L 2 --- ---

Print out the answer sheet to use with the following questions.

Circle the correct answer and review with director: l l l Question 1: A, B, C, D, E. Question 2: A, B, C, D, E. Question 3: A, B, C, D, E.

l 1. The motion through the lumbar vertebrae is described as: a. b. c. d. e. Rotation Cataring Opposition Flexion and extension Juxtapositioning

l 2. The number of lumbar vertebrae: a. b. c. d. e. 7 5 6 10 4

l 3. Scoliosis is a contraindication to lumbar mobilization. a. b. True False

Certificate of Completion I, _____________, successfully completed the Pediatric OMT Module on __ __ 20__ Signatures: l Pediatric Resident __________ l Pediatric Residency Director______ l l ( Please print and give to program director. )

Congratulations
- Slides: 27