Pediatric imaging Learning objectives 1 Systemic approach interpretation

Pediatric imaging

Learning objectives 1. Systemic approach interpretation 2. Recognize the normal anatomical structures and the range of normal appearance 3. Describe the criteria for diagnosis of pulmonary opacity , pleural effusion , pneumothorax, pulmonary collapse and cardiomegaly on CXR. 4. Recognizing free intra abdominal air and what imaging position is favorable

differentiate between normal distribution of abdominal gas pattern , dilated small bowl and Large bowl on plain abdomen x-ray. 6. construct the appropriate imaging algorithm for common diagnostic scenarios. 5.

Plain chest film Is usually taken in the supine AP projection , and PA according to patients age and cooperation. indication respiratory distress…. Ex, pneumonia Lung collapse Pneumothorax Emphysema Pleural effusion

Prolonged or chronic cough Persistent cough , if more than 3 wks. Even in the absence of chest signs. X ray may show , lobar collapse, emphysema, dens hilar shadow or pulmonary infiltrate

Prolonged fever More than 10 – 14 days is a definite indication with absence of localization May revile lung abscess , hilar shadow or pulmonary infiltrate
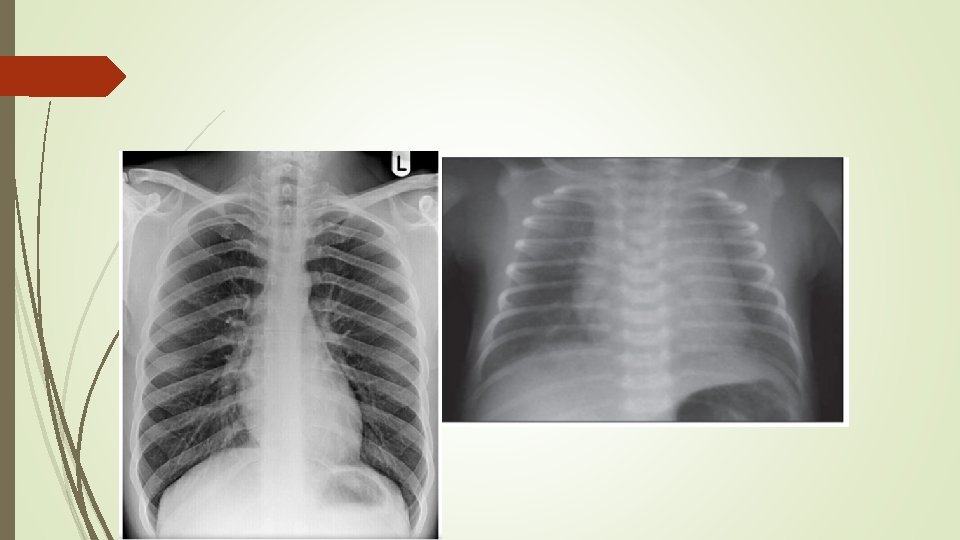

The normal chest in the young 1. well specialized normal heart size , which looks objectively enlarged , among a relatively small lung. Normal anterior superior mediastinum (thymic shadow ) Transverse rib orientation. With equal intercostal spaces , on both sides Clear both lung fields with faint vascularity gas under the LT hemidiaphragm Liver under the Rt hemidiaphragm Central trachea and both sternal end of the clavicles, to avoid error misinterpretation Clear lung fields

Normal chest pa view

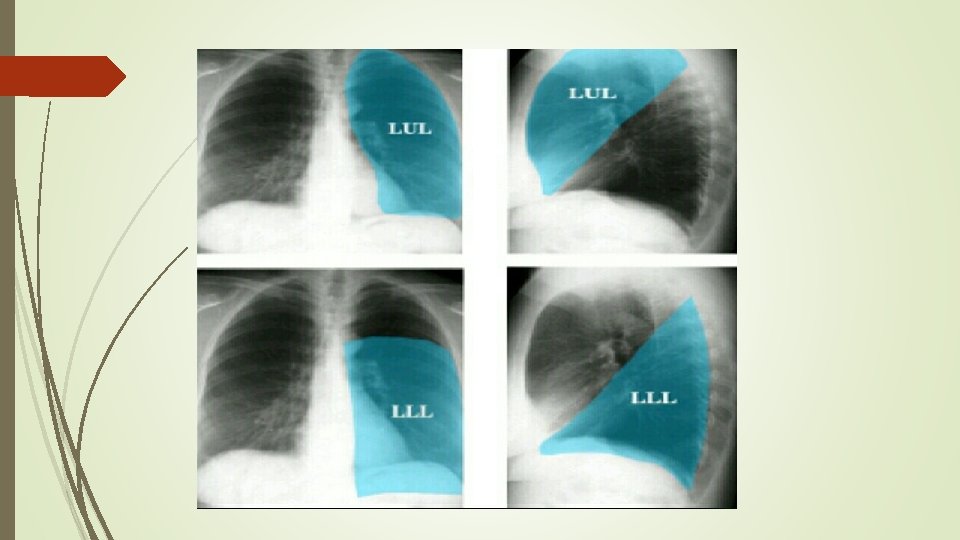
Lung zone

Congenital heart disease

Congenital heart disease , increase pulmonary vascularity

increase lung vascularity Upper lobe blood diversion, vascular redistribution Prominent vessels Reaching the lung apex and periphery

Tetralogy of Falot Cyanotic Congenital heart disease Difficult breathing , finger clubbing , heart murmur.


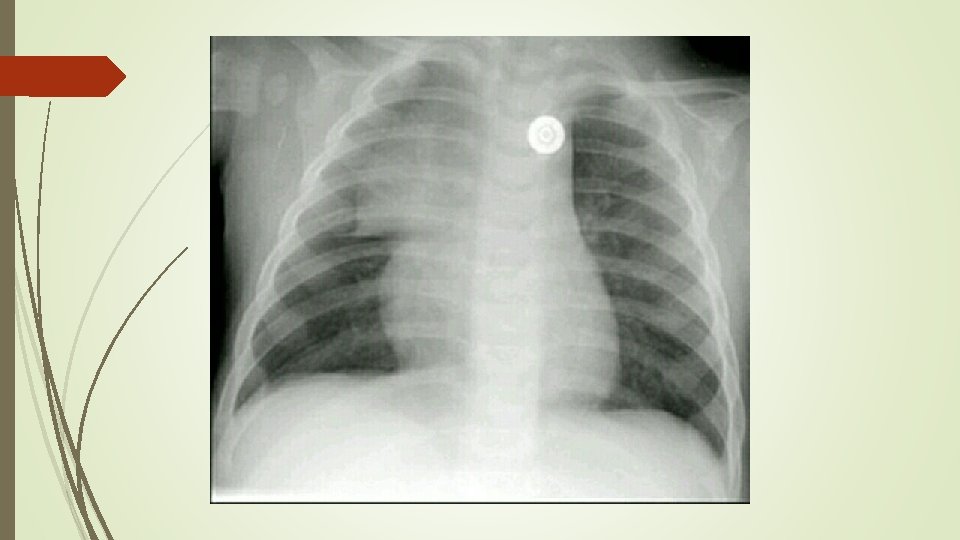
right lung collapse with compensatory inflated left lung Shift of mediastinum to the Rt side Hyper inflated Lt lung with herniation the rt side Clear both costo- phrenic angels


Bilateral pulmonary infitrate DDX bilateral broncho pneumonia pulmonary odema Showing bilateral ill-defined , defuse pulmonary infiltrate, with relative clear both cost phrenic angles


Right side pneumothorax Collapsed Rt lung. Moderate shift of the mediastinum to the LT side


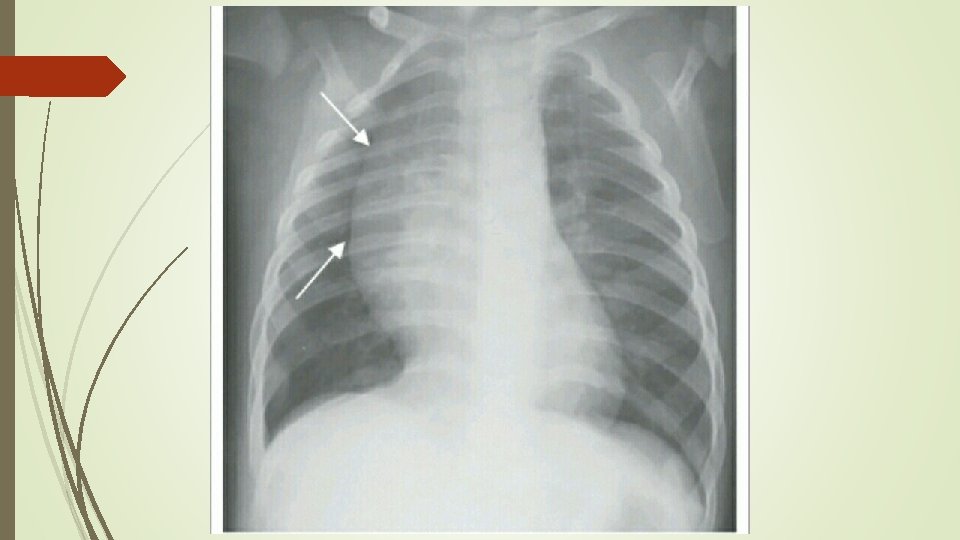
Lt sided mid lobe pulmonary infiltrate lt sided pulmonary opacity with fading lateral borders silhouetting the LT heart border, with mild pleural effusion ( blunting of the LT costophrenic angles)

Middle lobe consolidation


Bilateral moderate –severe pleural effusion Loss of both heart borders, diaphragm and costo phrenic angle with upper border meniscus sign presentation


Pulmonary Mets. Bilateral variable size, non symmetric distribution of pulmonary nodularity's DXX Multiple pulmonary hydatid Metastatic neuroblastoma , Wilms tumor
- Slides: 30