Pediatric ED Case Conference Presented by R 1

Pediatric ED Case Conference Presented by R 1 謝岳哲

General Data �Name: 溫XX �Gender: Male �Age: 4 y 3 m/o �BW: 16 kg �Chart No: 4380467

2006 -02 -19 20: 53 �Keelung ER �Triage: 3級 �檢傷記錄:病患主訴因腹痛 �Vital signs: --BT: 35. 4 --HR: 129 --RR: 20 --BP: 160/109

Chief Complaint �Post-prandial abd pain was noted after 稀飯 today

Present Illness �No diarrhea �No fever �Activity: good �Last meal: decreased �Watery drinking: OK �Decreased urine output �Vomiting and diarrhea 5 days ago with improved

Past History: �Denied systemic disease �Allergy: Nil �Vaccination: as scheduled

Physical Examination �Cons clear, E 4 V 5 M 6 �HEENT : No active lesion �HEART : tachycardia without murmur �CHEST : clear BS �ABDOMEN : normoactive BS tenderness over epigastrium and periumbilicus �EXT: free movable �小朋友抱在媽媽懷裡,不肯下來走

�What else more do you want to know? �What’s your impression?

More about the patient…… �History: Ø Location? Onset? Pattern? Radiation? Alleviating or aggravating factors? Associated symptoms? Ø Nausea/vomiting? Diarrhea? Bloody? Mucus? Ø Fever? Cough? Sore throat? Headache? Dysuria? Hematuria? Ø Trauma? Previous surgery? Congenital disorder?

More about the patient…… �PE Ø Appearance: dehydration? Toxic? Ø Abdomen: Percussion? Peritoneal signs? Mass? Ø Pharyngeal erythema? exudate? Ø Breath sound? Heart sound? Knocking pain? Ø Jaundice? Skin rash? Petechiae?

Pediatric Assessment Triangle B: work of breathing Abnormal airway sounds Abnormal positioning Retractions Flaring A: appearance – “TICLS” T– Tone I– Interactiveness C– Consolability L – Look/Gaze S – Speech/Cry C: circultion Pallor, Mottling, Cyanosis
 Common Ø AGE Ø UTI Ø Trauma")
Differential diagnosis of abdominal pain (2~5 Y/O) Common Ø AGE Ø UTI Ø Trauma Ø Appendicitis Ø Pneumonia, asthma Ø Viral syndromes Ø Constipation Less Common Ø Meckel’s diverticulum Ø HSP Ø Toxin Ø Intussusceptions Ø Nephrotic syndrome Ø Cystic fibrosis Rare Ø Incarcerated hernis Ø HUS Ø Neoplasm Ø Hepatitis Ø Myocarditis, pericarditis Ø Inflammatory bowel disease Ø Choledochal cyst Ø DM Ø porphyria Textbook of Pediatric Emergency Medicine 5 th ED, Table 50. 1
 Abdominal Ø Trauma Ø Intussusception Ø")
Life-threatening causes of acute abdominal pain (2~5 Y/O) Abdominal Ø Trauma Ø Intussusception Ø Appendicitis Ø Incarcerated hernia Ø Meckel’s diverticulum Ø Obstruction secondary to previous OP Ø Peritonitis Extra-abdominal Ø Toxic overdose Ø HUS Ø DKA Ø Sepsis Ø Myocarditis, pericarditis Textbook of Pediatric Emergency Medicine 5 th ED, Table 50. 2

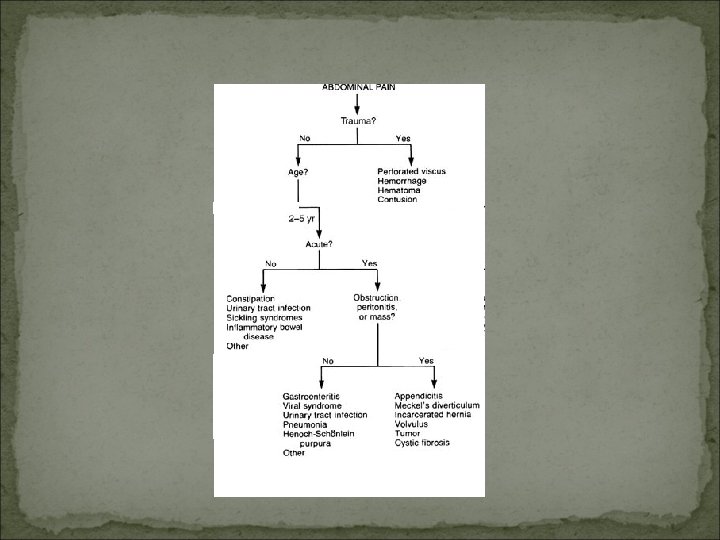
Evaluation of abdominal pain

ED initial impression �Abdominal pain, r/o gastroenteritis

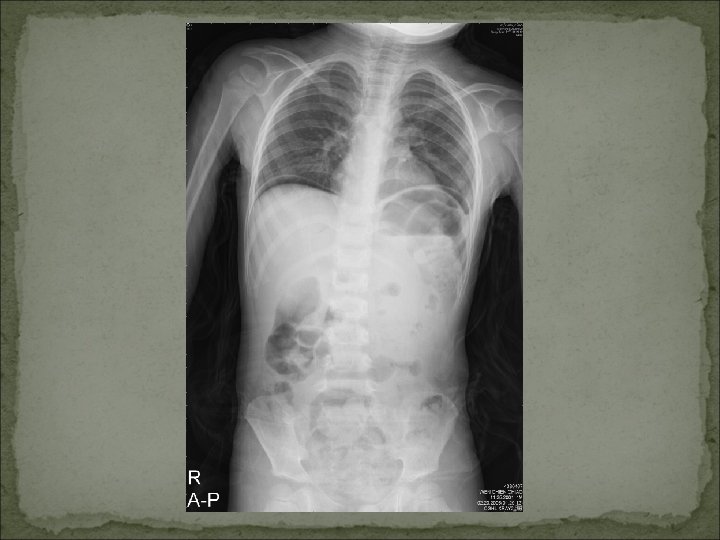
Initial Order �CBC/DC, BUN, CRP, Sugar �KUB �IV with D 5 W run 60 cc/hr

�Any comment about the order?


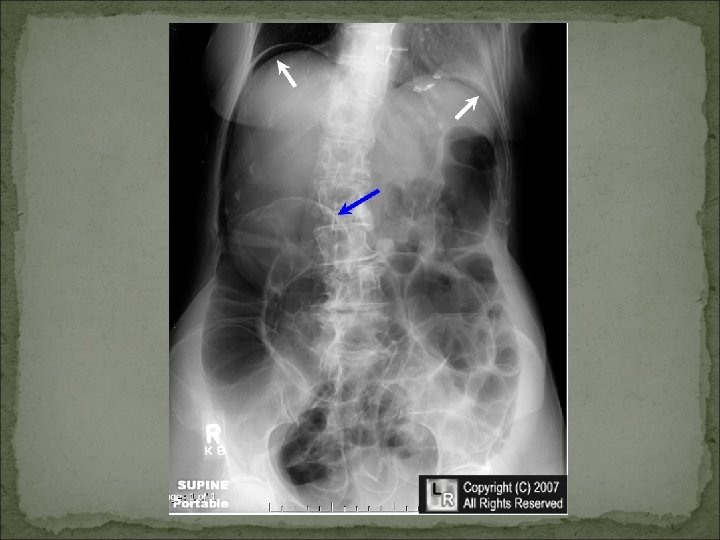
�Bilateral subphrenic free air, C/W bowel perforation


Pneumoperitoneum �Football sign �Double wall sign �Triangle sign �Hepatic-lucency sign �Visible falciform ligament

Extraluminal air “triangle sign” 腸子看起來很立體 “double wall sign” Falciform ligament


Impression �Hallow organ perforation, cause? �Pan-peritonitis

Clinical course �Consult GS �Empirical Abx use �Transfer to Linko for operation

Lab results Item WBC RBC Hb Hct MCV PLT Segment Lymphocyte Monocyte Eosinophil Value (2/19) 18. 1 K/u. L 5. 48 M/u. L 11. 7 g/d. L 37. 6% 68. 6 f. L 290 K/u. L 76% 20% 1% 3% Item Value (2/19) Sugar 91 Na 138 K 3. 9 Cl 105

OP Note �Date: 2006/02/20 �OP procedure: laparoscopic repair of perforated duodenal ulcer 1. 2. 3. 4. Ascites: 100 cc turbid ascites Duodenal ulcer: perforation at 1 st portion, near lesser curvature, size 0. 3*0. 3 cm; omental wrapping around the perfoation hole (+) no other lesion was found in the peritoneal cavity fibrin coating over the duodenum

Clinical Course �Check gastrin level on 2/23: �Ascites culture: negative �Discharge on 2006 -02 -24 30. 8 (28 -185)

Final diagnosis �Duodenal ulcer with perforation at 1 st portion complicated with peritonitis s/p primary repair
- Slides: 33