Pediatric Chain of survival PBLS Prevention Early CPR

Pediatric Chain of survival PBLS Prevention Early CPR Prompt access to EMS Rapid PALS Integrated post-CA care 대한심폐소생협회
 Asphyxial CA ≫ VF CA ( in")
ABC or CAB? in PBLS v Incidence) Asphyxial CA ≫ VF CA ( in infants and children) v Ventilations are extremely important in ped resuscitation. ABC makes a difference? CAB 대한심폐소생협회
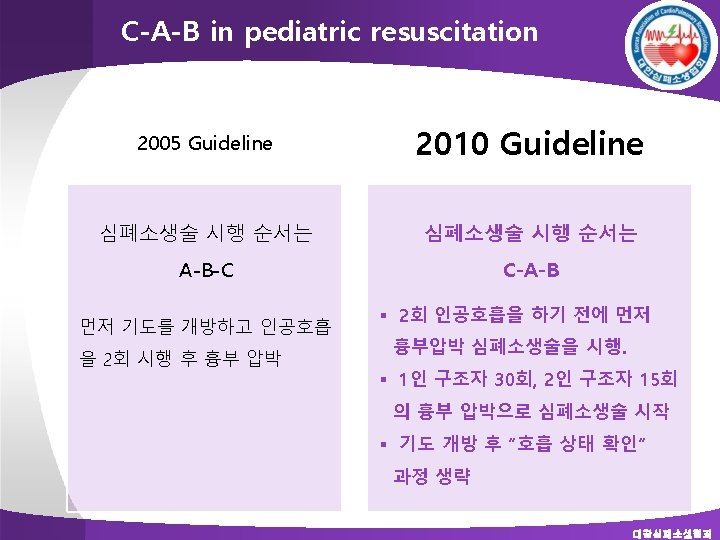

PBLS Sequence for Lay Rescuers Safety of Rescuer and Victim Assess Need for CPR Check for Response Check for Breathing Start Chest Compressions Open the Airway and Give Ventilations Coordinate Chest Compressions and Breathing Activate Emergency Response System 대한심폐소생협회

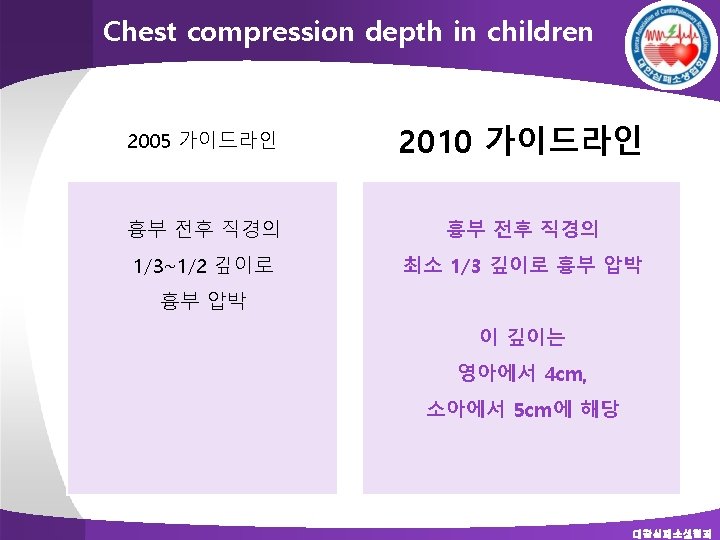
High quality CPR in PBLS v Push fast : at least 100 compressions / min v Push hard : at least 1/3 depth of AP diameter of the chest n 1. 5 inches (4 cm) in infants n 2 inches (5 cm) in children v Allow complete chest recoil v Minimize interruptions of chest compressions v Avoid excessive ventilation 대한심폐소생협회

Chest compression depth in children Pediatrics. 2009; 124: e 69 -74 : 280 consecutive CT reconstruction, < 8 yrs 대한심폐소생협회

Chest compression depth in children Pediatrics. 2009; 124: e 69 -74 # Residual internal depth < 10 mm ; potential to injure the intrathoracic structures and may actually not be achievable 대한심폐소생협회

Chest compression depth in children Pediatrics. 2009; 124: e 69 -74 - 1/2 compression : residual space < 10 mm: 94%, 너무 깊다 - 1/3: compression: 0. 5% 대한심폐소생협회

Pediatric BLS Algorithm 대한심폐소생협회


Chest compression for infants 1 rescuer : Two finger tech 2 rescuers : Two thumb-encircling tech 대한심폐소생협회

Two thumb-encircling technique No data show benefit from a circumferential squeeze v Higher CPP than the 2 -finger technique v If you cannot physically encircle the victim’s chest, compress the chest with 2 fingers. 대한심폐소생협회

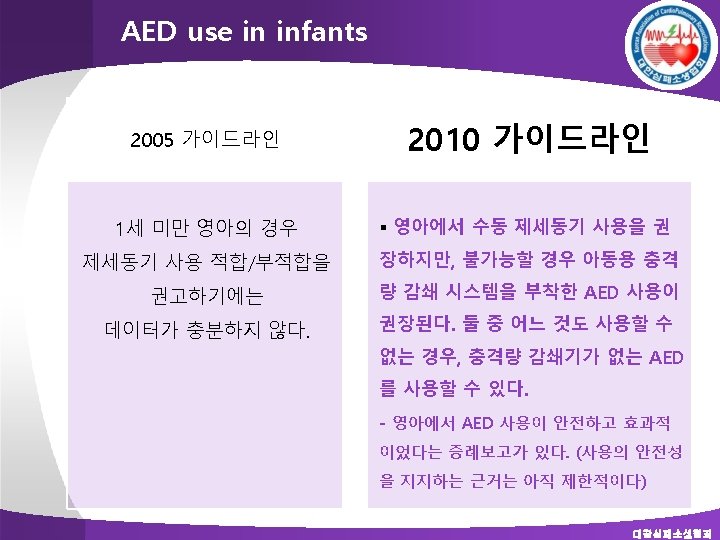
Defibrillation in pediatric BLS v For infants a manual defibrillator is preferred when a shockable rhythm is identified by a trained healthcare provider (Class IIb, LOE C). v If a manual defibrillator is not available, an AED equipped with a pediatric attenuator is preferred for infants. v If neither is available, an AED without a dose attenuator may be used (Class IIb, LOE C). v AEDs that deliver relatively high energy doses have been successfully used in infants with minimal myocardial damage and good neurological outcomes. 대한심폐소생협회

Hands-Only CPR in PBLS v Optimal CPR in infants and children includes both compressions and ventilations, but compressions alone are preferable to no CPR (Class 1 LOE B). 대한심폐소생협회

Hands-Only CPR in PBLS Lancet. 2010; 17: 1347 -54 - 5, 170 children, < 17 yrs - 3, 675 (71%) non-cardiac causes, 1, 551 (30%) cardiac arrests 대한심폐소생협회

Lancet. 2010; 17: 1347 -54 대한심폐소생협회

Avoid excessive ventilation v Excessive ventilation is harmful because it § Increases intrathoracic pressure and impedes venous return and therefore decreases cardiac output, cerebral blood flow, and coronary perfusion. § Causes air trapping and barotrauma in patients with small airway obstruction. § Increases the risk of regurgitation and aspiration in patients without an advanced airway. 대한심폐소생협회

Other CPR Techniques and Adjuncts v Insufficient data in infants and children to recommend for or against the use of the following: n Mechanical devices to compress the chest n Active compression-decompression CPR n Interposed abdominal compression CPR (IAC-CPR) n The impedance threshold device n pressure sensor accelerometer (feedback) devices. 대한심폐소생협회

Foreign-Body Airway Obstruction v No change v 5 back blows + 5 chest compressions for infants v Abdominal thrusts for children 대한심폐소생협회

Special Resuscitation Situations 대한심폐소생협회
 (O) Neutral Position 대한심폐소생협회")
BLS for injured child (X) (O) Neutral Position 대한심폐소생협회

Thank you.
- Slides: 26