Pediatric case conference Scrotal pain in children Personal

 n Sex:")




 n Abdomen: soft, mild distended, general tenderness, no muscle guarding n")














- Slides: 22
Pediatric case conference Scrotal pain in children
Personal Data n Name: 蔡XX n Age: 9 y/o 8 m/o (1998/5/10) n Sex: male n Chart No. : 9877343
2008 -1 -11 15: 04 n Vital signs: n BT: 35. 6, HR: 99, RR: 20 n BW: 33 kg n 檢傷 3級: n 病患主訴因睪丸腫脹, 中度疼痛
Chief complaints n Scrotum pain since last night
Present Illness No fever n Left scrotum pain n No dysuria n Activity: decreased n Appetite: good n Past history: denied n Vaccination: as schedule n Allergy history: denied n Travel history: denied n
Physical Examination n PAT: n Appearance: ill-looking n Breathing: smooth, no retration n Circulation: oximeter: 99%, stable n E 4 V 5 M 6 n HEENT: throat no injection, ear-drum: ok n Chest: bil. Clear, RHB without murmur
Physical Examination (continue) n Abdomen: soft, mild distended, general tenderness, no muscle guarding n Extremity: free, no skin rash, CRT < 1 sec n Left scrotum erythema, swelling and severe tenderness, no relieved by lifting Prehn’s sign: (-)
n Impression ? ?
The most common causes of acute scrotal pain in children n torsion of the appendix testis (46%) n Epididymitis (35%) n Testicular torsion (16%) • Lewis, AG, Bukowski, TP, Jarvis, PD, et al. Evaluation of acute scrotum in the emergency department. J Pediatr Surg 1995; 30: 277.
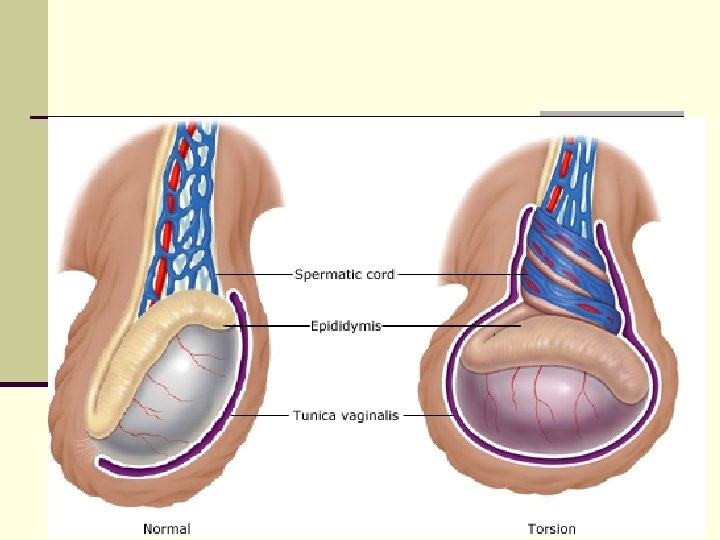
Normal testis anatomy
Distinguishing features of conditions associated with scrotal pain Acute epididymitis Testicular torsion Torsion of appendage Peak incidence Perinatal and puberty Prepubertal <2 years and postpubertal Onset of pain Usually sudden Usually gradual Duration of pain Usually < 12 hours Usually >24 hours Previous episodes Typical Unusual If previous episode Nausea and vomiting Common Uncommon Fever Unusual Common History of trauma Occasional Unusual Dysuria or discharge Rare Common Historical features
Testicular torsion Torsion of appendage Suggestive fingings Bell-clapper Palpable nodule "Blue dot" None Cremasteric relfex Usually absent Usually present Tenderness Testicular initially, then diffuse Appendage initially, Epididymis initially, then testis then diffuse Scrotal erythema or edema Common >12 hours Acute epididymtis Physical findings
Blue dot sign n Infarction and necrosis of the appendix testis can be seen as a "blue dot" sign (arrow) in 21 percent of cases. Reproduced with permission from Charise Johns, MD.
Testicular torsion Torsion of appendage Unusual Common Positive smear or culture No No Often Leukocytosis Uncommon Common Acute epididymtis Laboratory tests Pyuria Common
Testicular torsion Torsion of appendage Acute epididymtis Perfusion studies Color Doppler Decreased Normal or increased Radionuclide Decreased Normal or increased
Urine analysis Color Amber Turbidity Clear SP. gravity 1. 028 PH 7. 0 Leukocyte Trace Nitrite Negative Protein Negative Glucose Negative Ketone Negative Urobilinogen 1. 0 Bilirubin Negative Blood 3+ RBC 141 WBC 1 Epith-Cell 0
Summary of patient n Pre-puberty n Acute onset scrotum pain with swelling and tenderness(persistent or intemittent ? ) n Pain duartion: 12 -24 hs n Prehn’s sign: (-) n U/A no pyuria n Q 1: Testis torsion/intermittent torsion ? Or appendage torsion ? n Favor testis torsion (more information will be better) n Q 2: what’s next ? n Consult Urologist
Urologist Consultation n PE: n soft abdomen n Testis: L’t > R’t n Left scrotum swelling with erythema n Tenderness n Prehn’s sign: negative n Testis echo: left testis flow (+) n Impression: r/o testis torsion
OP note n Scrotal approach left testis torsion about 270 degree was noted, after detorsion testis color recovered, testis appendix congestion, excision of appendix was done. n Right orchiopexy was done
Discussion n What role is color Doppler playing in diagnosis of acute scrotum? n testicular and epididymal size n scrotal fluid n scrotal wall thickening n enlarged appendix testis n arterial flow in the testis and epididymis n decreased testicular perfusion § § § n testicular torsion large hydrocele Abscess Hematoma scrotal hernia Negative scans § spontaneous detorsion § partial or intermittent torsion n How many percentages of diagnosis of testis torsion are done by clinically without color Doppler ?
n Thank you for attention