Pediatric case Conference R 1 Pediatric case Conference




")


 n n n n n Ao (mm): 15 LA")
 3 D CT of chest performed on 6/25 n There")





























- Slides: 47
Pediatric case Conference 報告人:R 1 李怡農
Pediatric case Conference 吳小弟 n 病歷號: 7169971 n 生日: 94/11/02 n 就診日期: 96/6/19 (1 y 7 m/o) n TPR: 36. 6/130/21 n CC:Fever for 2 days n
Present Illness Fever 38. 9 C for 2 days n Acetaminophen 4 ml q 4 h by family -> not subsided n cough(+) with sputum(+), rhinorrhea(+) n no diarrhea n vomit for 2 days, many times after drinking or eating n Activity: good n
Present Illness 過去病史: Ever admission due to Enterovirus and Pneumonia n 過敏史: denied n 旅遊史: denied n Vaccination: as schedule n
PE n n n n n PAT:Appearance/Breathing/circulation:all good Conscious: alert, Conjunctiva: not pale, injected(-) Throat: injected(+), Tonsils: enlarge(+), exudate(-) Eardrum: not injected Neck: supple, No LN enlarge Chest: Coarse BS, especial over right side Heart: Regular heart beat, No murmur Abdomen: Soft and flat; Normoactive bowel sound Tenderness(-), Rebound pain(-) Mc. Burney's point tender(-) Extremities: Freely movable, Skin rash(-)
Ped. 2 -D echo (2007/3/12) n n n n n Ao (mm): 15 LA (mm): 15 LVEDD (mm): 32 LVESD (mm): 18 EF: 78 % Dextroposition of heart. (Whole heart shift to right side of spine, apex pointed to left side) Normal intracardiac structural relationship. No pericardial effusion. Good ventricular performance. Vmax 0. 9 m/s for main pulmonary artery. No significant mitral and tricuspid regurgitation. No VSD, no PDA. 2. 9 mm atrial septal defect, secundum type. Normal left-sided aortic arch. Vmax 1. 0 m/s for ascending aorta Vmax 1. 3 m/s for descending aorta. Descending aorta at left anterior aspect of spine. Right-sided superior vena cava. Inferior vena cava at right anterior aspect of spine.
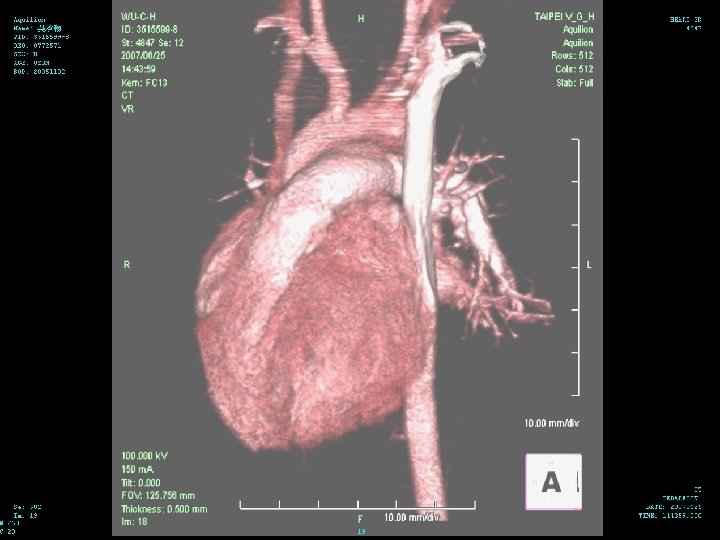
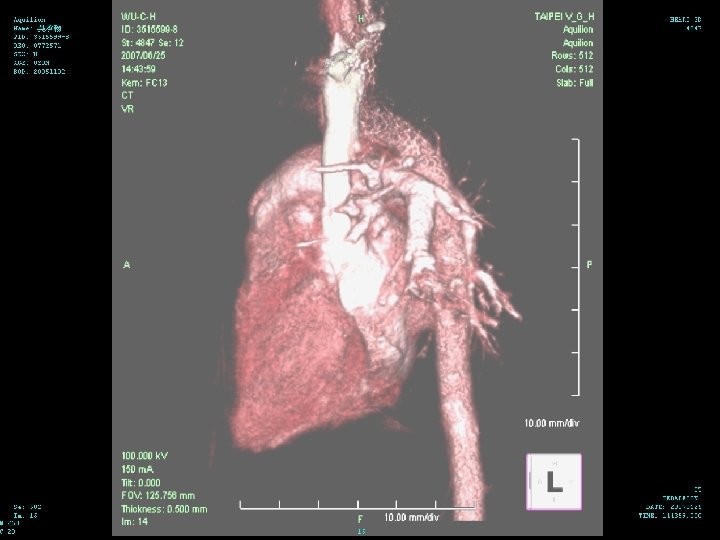
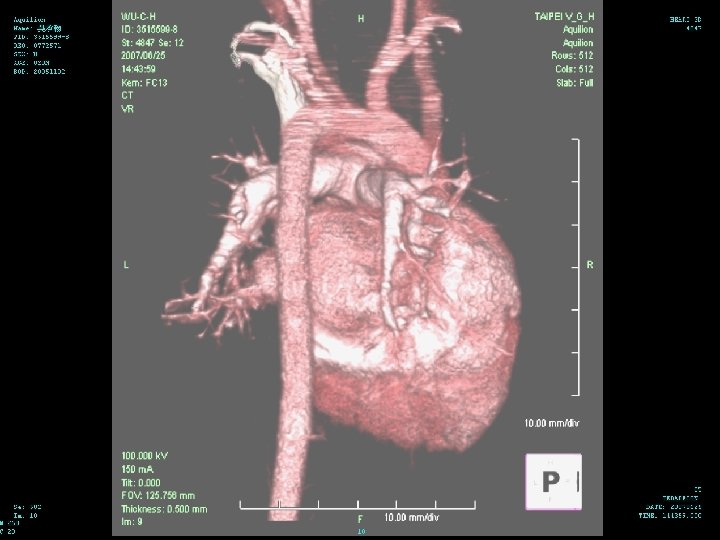
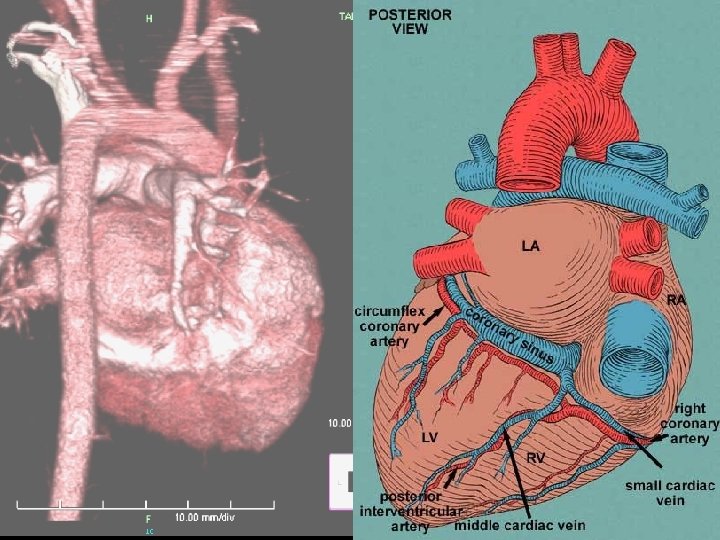
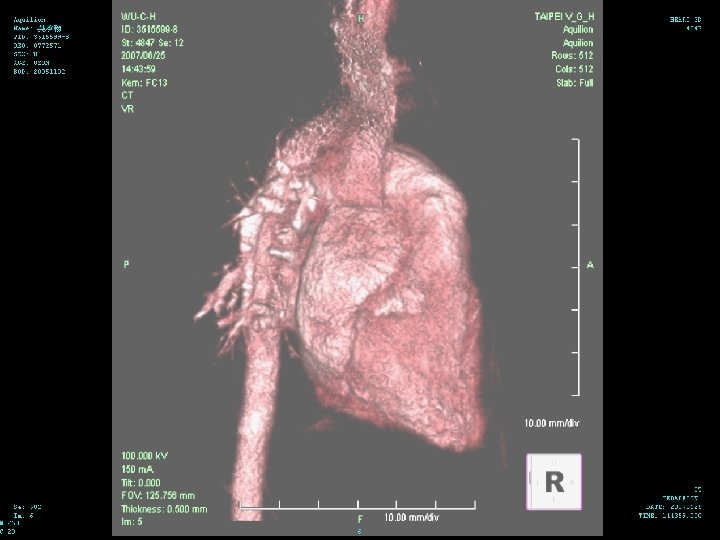
Hospital Course (6/25 -28) 3 D CT of chest performed on 6/25 n There is narrowing of the trachea in the level of aortic arch with narrowest diameter about 0. 25 cm about 1. 2 cm in length n There is dextrocardia with left side aortic arch n There is double SVC with left SVC drainage to coronary sinus n
Difficult Feeding / Dysphagia
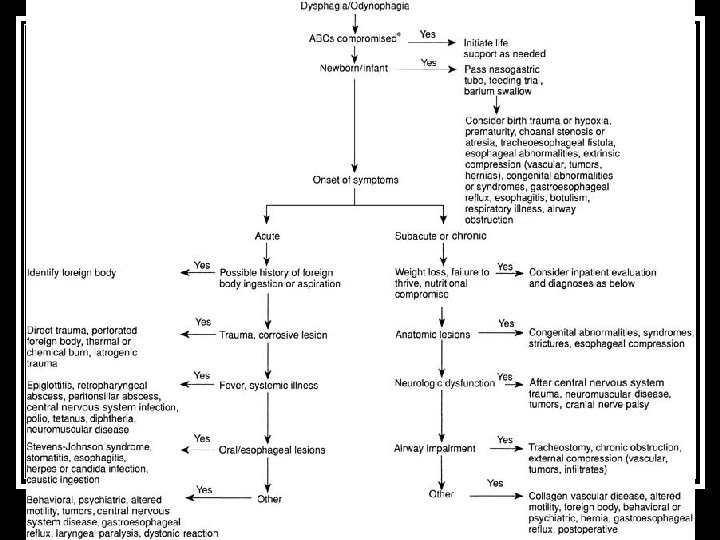
Dysphagia any difficulty or abnormality of swallowing n may be life threatening if respiration or nutrition are compromised n Odynophagia (pain on swallowing) n sialorrhea (drooling) n
How to Approach Dysphagia n n n n Timing:Onset Age / Acute / Intermittent Nutrition:weight / develop Chewing / Solid / Liquid Pain / Fever Cough / dyspnea / stridor / Choking Drooling / Regurgitation / vomit Birth Hx / Pregnant Hx / Family Hx Trauma ?
How to Approach Dysphagia GI tract / Respiratory / Systemic n Pre-esophagus / Esophagus / Stomach / Intestine n Mechanical / Anatomy / Neurology / Inflammation / Miscellaneous n
Life-threatening Causes of Dysphagia n n n n Foreign-body aspiration/ingestion Tracheoesophageal fistula Upper airway obstruction Traumatic esophageal perforation Epiglottitis Retropharyngeal abscess Botulism n n n n Tetanus Polio Diphtheria Central nervous system infection/abscess Stevens-Johnson syndrome Corrosive ingestion Laryngeal paralysis
Vascular Ring
Vascular Ring n n n congenital condition anomalous configuration of the arch and/or associated vessels surrounds the trachea and esophagus forming a complete or incomplete ring around them usually occur without associated cardiovascular anomalies. Ventricular septal defect is the most common associated anomaly
Epidemiology less than 1% of all congenital cardiac defects n equal frequency in both sexes n Some vascular rings are associated with other congenital heart defects; others may be isolated deficits n
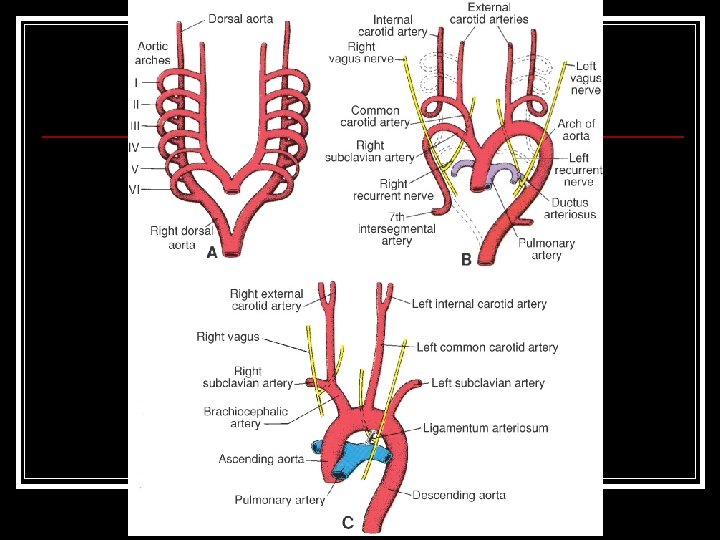
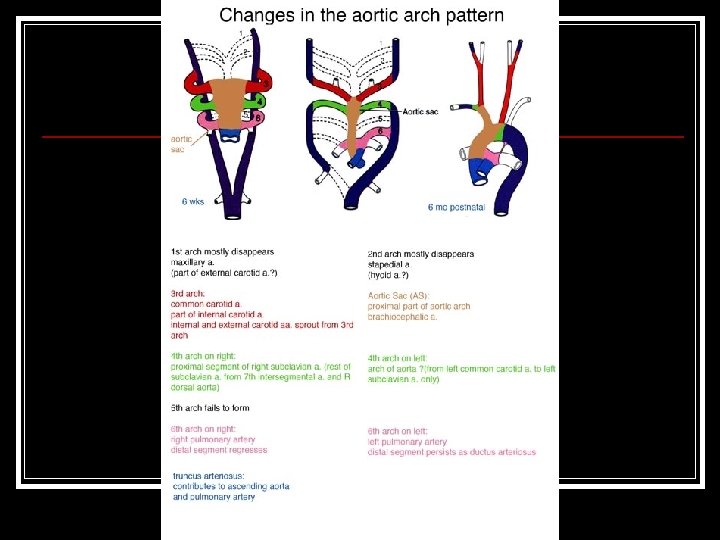
Etiology from the abnormal or incomplete regression of 1 of the 6 embryonic branchial arches n Several recent papers report the close association of band 22 q 11 deletion (20% of patients ) n
Arch Develop n Early in normal development, both a dorsal and a ventral aortic arch are present. The 2 arches are connected by 6 embryonic branchial arches
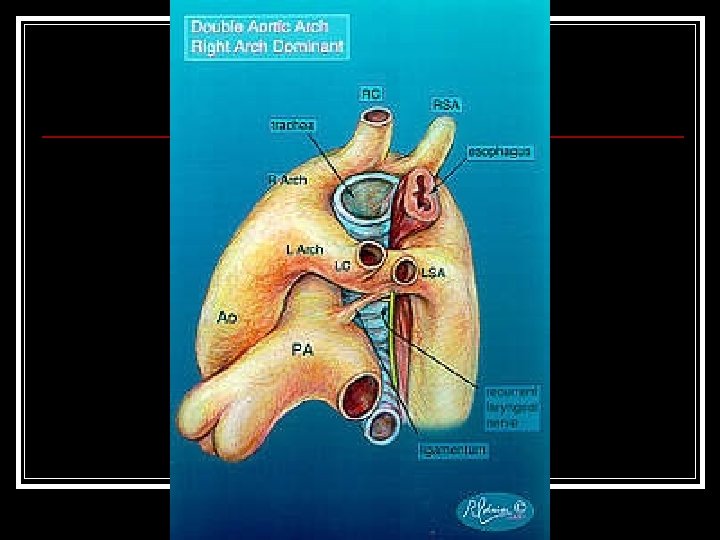
Subtype - 1 n n n Double aortic arch Complete Most
Subtype - 2 n n n Right aortic arch with left ligamentum arteriosum Complete These make up 8595% of the cases.
Subtype - 3 n n n Right aortic arch with mirror-image branching and retroesophageal ligamentum arteriosum Complete 小於 1%
Subtype - 4 n n n Left aortic arch with right descending aorta and right ligamentum arteriosum Complete 小於 1%
Subtype - 5 n n Retroesophageal right subclavian artery with left aortic arch and left ligamentum arteriosum not complete
Subtype - 6 n n Aberrant left pulmonary artery or pulmonary artery sling not complete
Clinical n n airway or esophageal compression. present with symptoms in infancy or very early in childhood stridor, cyanosis, wheezing, respiratory distress, apnea, and/or a characteristic high-pitched, brassy cough history of asthma, recurrent pneumonia, or evidence of dysphagia or difficulty with feedings
Clinical airway symptoms are worsened or aggravated by feedings n Others may try to maintain a position in which the head is hyperextended to improve breathing and minimize the obstruction n
Clinical n n n Dysphagia and symptoms related to the esophagus are the more likely presenting findings in older children and adults slow breast or bottle feeding, fatigue with feeding, frequent regurgitation, and aspiration pneumonias In most cases, workup is initiated when solid foods are introduced, which causes more pronounced dysphagia
Clinical The double aortic arch is the anomaly that usually produces the most severe airway compression in the youngest patients n some patients with a complete vascular ring have minimal symptoms or remain asymptomatic n
Diagnosis identification of a right aortic arch on chest radiograph n An ill-defined arch location is often observed in patients with double aortic arch n compression of the trachea and hyperinflation and/or atelectasis of some of the lobes of either lung n chest radiography is not very sensitive n
n n barium esophagram to be the most important study Double aortic arch produces bilateral and posterior compressions of the esophagus
Diagnosis n n n Echocardiographic studies have been increasingly used for the diagnosis of a vascular ring Structures without a lumen, such as a ligamentum arteriosum or an atretic arch, have no blood flow and are difficult to identify identification of compressed midline structures and their relationship to encircling vascular anomalies may be difficult to detect
Diagnosis CT/MRI/Angio:These expensive radiological studies are rarely necessary to evaluate vascular rings n Although these modalities provide excellent delineation of all of the associated structures, they should be reserved for cases in which the results of barium esophagram do not provide a clear diagnosis n
Diagnosis Bronchoscopy has been used in the evaluation of children with symptoms of airway obstruction or compression n In the presence of a vascular ring, pulsatile external tracheal compression is easily observed n
Treatment No medical therapy exists n Surgical division of symptomatic vascular rings is the only appropriate form of therapy n surgery should not be delayed in the presence of a respiratory tract infection n
Prognosis About 95% of patients who undergo surgical correction of a vascular ring survive long term n most of these are soon relieved of their symptoms n
Discussion Time
Thank You For Attention