Pediatric Case Conference hip pain R 1 General

")
 T: 36. 1/℃ P: 76/min R: 18/min BR: 129/71/mm. Hg")

 n Localized(+) pain in post right thigh area without")
 , eardrum not injected tonsil enlargement(-) exudate(-) n Chest: clear")


 sinusitis admission hx, no OP hx n Drug allergy: NKA")

 Check CBC DC, CRP, CR , B/C, on saline lock n")





 Severe right thigh pain and fever r/o pyomyositis ( 10/26 12:")
 n n n WBC 18. 3 1000/u. L H M")
 Creatinine(B) 1. 1 mg/d. L n CRP 365. 49 mg/L")

 Check SUGAR BUN ALT/GPT ALK-P NA K n")
 n n n n Color YELLOW Yellow Turbidity CLEAR")
 n n n Sugar 149 mg/d. L H")
")









 n n n Avulsion of right ischial tuberosity probably by")


 Gm(+) cocci n Final diagnosis in ER: 1. Avulsion")
 Oxacillin 500 mg/vial(inj. ) 2 PC Q 6 H (10/26~)")







-septic arthritis The hip is the joint infected second most frequently")


-Osteomyelitis of the femur or pelvis can present with hip pain n The")
 n n n Transient synovitis — Transient synovitis (TS) is a")




- Slides: 57
Pediatric Case Conference hip pain 報告:R 1 林琪峻 指導醫師: 吳孟書醫師
General Data 14 -year-old boy n No. 3371856 n Body weight: 80 Kg(>97 percentile) n TPR: T: 36. 1/℃ P: 76/min R: 18/min BP : 129/71/mm. Hg n 到院時間: 10/26 11: 34 n
Pediatric assessment triangle (PAT) T: 36. 1/℃ P: 76/min R: 18/min BR: 129/71/mm. Hg Respiration Appearance n Retraction (-) E 4 V 5 M 6 Tachypnea (-) Not Pale Ill-looking Circulation CRT < 2 sec
Present illness Right thigh injury about 4 months ago due to practice跆拳道, then he suffered from chronic hip pain since than n The right thigh pain aggrevated in these days n Intermittent fever(+) up to 38 for 3 days n Cough(+), rhinorrhea(+) in recent days n he was sent to LMD where antipyretic was prescribed but fever off and on was still noted n
Present illness No Trauma hx(-) n Localized(+) pain in post right thigh area without radiation, tender point(+) n Walk by walk stick n
Physical examination Throat injected(+) , eardrum not injected tonsil enlargement(-) exudate(-) n Chest: clear breathing sound n Abdoman: no tendeness, no rebounding pain n Extremities: movement smoothly without pain n Right post upper thigh pain aggrevated when passive movement n Right thigh area: no erythematous change, no swelling, no open wound , local heat(+), symmetric bil lower extremities, pitting edema(-) n No prei-anal abscess n
What’s your impression? What else do you want know?
討論可能的D/D Muscle strain n Septic hip n Pyomiositis n Psoas abscess n Osteomyositis n
Past History Admission history(2006) sinusitis admission hx, no OP hx n Drug allergy: NKA n Travel hx(-) n
Impression URI n r/o pyomyositis, septic hip n
Management( 10 min) Check CBC DC, CRP, CR , B/C, on saline lock n Pelvic view , chest P-A view n Keto 1 AMP stat n
Any question about the management?
應該要再增加的 ESR , echo quided aspiration of joint fluid n Na, K , myoglobin , CK n
現場的初步診斷是? URI n pyomyositis n
CXR
Management (1 hr) Severe right thigh pain and fever r/o pyomyositis ( 10/26 12: 53) n NPO n Arrange CT of pelvic(+) n
Lab data( 1 hr) n n n WBC 18. 3 1000/u. L H M 3. 9 -10. 6 F 3. 5 -11 RBC 5. 00 million/u. L M 4. 5 -5. 9 F 4. 0 -5. 2 Hemoglobin 15. 1 g/d. L M 13. 5 -17. 5 F 12 -16 Hematocrit 44. 2 % M 41 -53 F 36 -46 MCV 88. 4 f. L 80 -100 MCH 30. 2 pg/Cell 26 -34 MCHC 34. 2 g/d. L 31 -37 RDW 13. 3 % 11. 5 -14. 5 Platelets 208 1000/u. L 150 -400 Segment 89. 0 % H 42 -74 Lymphocyte 4. 0 % L 20 -56 Monocyte 7. 0 % 0 -12
Lab data( 1 hr) Creatinine(B) 1. 1 mg/d. L n CRP 365. 49 mg/L H < 5 n
Impression Avulsion fracture n Fever cause unknown r/o pyomyositis n
Management ( 1 hr 30 min) Check SUGAR BUN ALT/GPT ALK-P NA K n Check U/A n Admission n Ceftriaxone 500 mg/vial(inj. ) 2 PC STAT IVF n
Lab dat U/A (2 hr) n n n n Color YELLOW Yellow Turbidity CLEAR Clear SP. Gravity 1. 021 1. 005 -1. 030 p. H 6. 0 4. 5 - 8. 0 Leukocyte Negative Nitrite Negative Protein 25 mg/d. L H Negative Glucose Negative g/d. L Negative Ketone Negative Urobilinogen 0. 1 EU/d. L 0. 1 - 1. 0 EU/d. L Bilirubin Negative Blood 3+ H Negative RBC 59 /u. L H <20/u. L WBC 17 /u. L <30/u. L Epith-Cell 3 /u. L <30/u. L
Lab data (2 hr 30 min) n n n Sugar 149 mg/d. L H 70 -105 BUN (B) 18 mg/d. L 6 -21 ALT/GPT 21 U/L 0 -36 ALK-P 118 U/L 28 -94 Na 141 meq/L 134 -148 K 4. 3 meq/L 3. 0 -4. 8
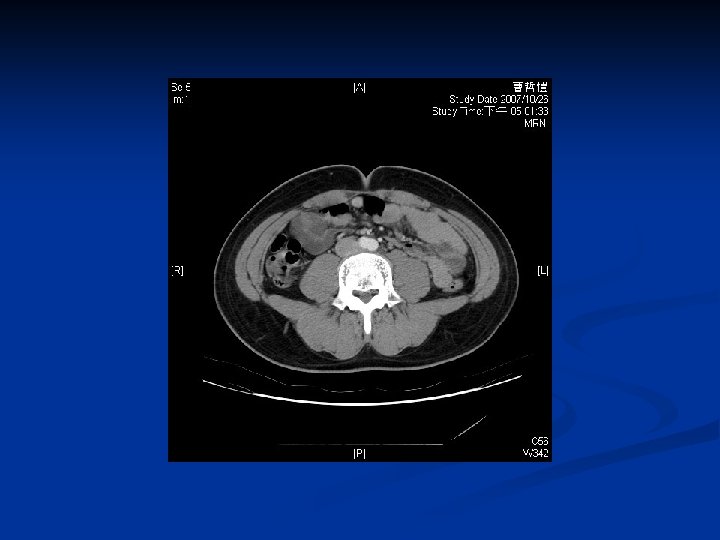
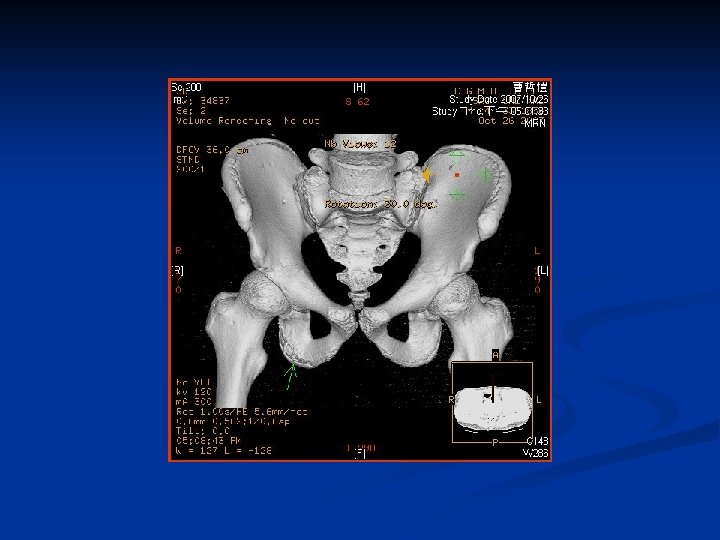
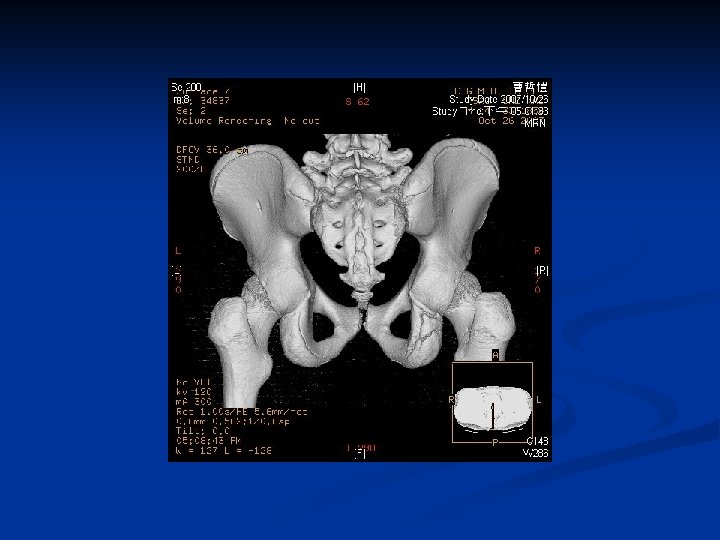
CT (4 hr 30 min)
CT report (next day) n n n Avulsion of right ischial tuberosity probably by adductor magnum. Minimal separation of nearly fused epipysis of the ischial tuberosity is seen. grossly there is no obvious muscle tear. No obvious abnormality of right thigh muscle is seen. No obvious fracture of pelvic girdle. Incidental finding of bilateral L 5 pars articularis fracture. Please take lumbar bilateral oblique views.
Impression Avulsion fracture n Fever cause unknown => pyomyositis less likely by CT image n
Management Consult Otho for avulsion fracture n => no surgery indication n =>antibiotic changed to Oxacillin 500 mg/vial(inj. ) 4 PC STAT IVF Ceftriaxone 500 mg/vial(inj. ) 2 PC Q 12 H IVF n Waiting for admission n
Lab data B/C (36 hr) Gm(+) cocci n Final diagnosis in ER: 1. Avulsion fracture 2. Fever cause unknown r/o pyomyositis, or septic hip n
Admission course (first day) Oxacillin 500 mg/vial(inj. ) 2 PC Q 6 H (10/26~) n Ceftriaxone 500 mg/vial(inj. ) 2 PC Q 12 H (10/26~28) n Aztreonam 1 PC Q 8 H (10/29~) n Arrange Sonography of Hip n
Lab data in admission n n B/C showed Staph. aureus 1/1 Clindamycin S , Erythromycin S , Oxacillin______ S ______, Penicillin . R , Sufamethoxazole-Trimethoprim . S , Teicoplanin_____ S ______, Tigecycline . S , Vancomycin
Progress note n -Discuss with radiologist Dr. 饒啟明: -osteomyelitis was not likely in this study of CT -the B/C yielded OSSA and right thigh pain may indicat: -> muscle injury with hemangioma formation and bacterial infection -> consider to arrange soft tissue echo to evaluate -> no need to arrange bone scan now
Discussion hip pain
Acute Hip pain n Pain — Acute onset of hip pain, particularly when it is severe, is associated with infectious processes (eg, septic arthritis, bacterial osteomyelitis), transient synovitis (TS), and major trauma.
Hip pain with fever n Fever >38. 5ºC is associated with acute infections but also may be present in both acute and chronic inflammatory processes
Hip pain with fever Recent upper respiratory tract infection can suggest transient synovitis; however, recent viral infections also are common in children with traumatic arthropathy or septic arthritis. n The recent use of antibiotics can alter the presentation of septic arthritis or osteomyelitis. Avid sports participation, a fall, or other injury suggests traumatic hip pain n
Hip examination n n Symmetry or asymmetry of the pelvis, thighs, and knees. Position partial flexion and external rotation of the hip may be indicative of increased intraarticular pressure. Swelling, heat, and overlying erythema rarely are identifiable on physical examination regardless of the severity of hip disease. The pelvis should be stabilized during examination of range of motion of the hip. Hip extension is best evaluated with the patient in the prone position The presence of muscle spasm should be evaluated. Can bear weight?
Hip pain ( infection)-septic arthritis The hip is the joint infected second most frequently in children, after the knee n Overall average 3 -6 y/o n potential for rapid joint destruction and longterm morbidity that can accompany delay in diagnosis and treatment n
Septic arthritis n n Hip: physis is intracapsular, allowing ready inoculation of the joint space from infection in the proximal femoral metaphysis. The most common organisms are Staphylococcus aureus and streptococcus. Bacterial enzymes and the products of inflammatory cells can destroy the joint or the growth plate, and pressure buildup within the capsule can impede blood flow, resulting in avascular necrosis. Reduced leg length and decreased joint mobility are commonly occurring sequelae. Outcome in children in whom diagnosis and therapy are delayed may be poor, particularly if an associated femoral osteomyelitis is present
Septic arthritis Weight-bearing and motion of the affected hip are quite painful and strongly resisted in all patients n Diagnosis is confirmed by ultrasound-guided aspiration of inflammatory hip fluid with identification of a causative organism by blood or synovial fluid culture n
Hip pain(infection)-Osteomyelitis of the femur or pelvis can present with hip pain n The proximal femur is the most common site of osteomyelitis in children. Pelvic osteomyelitis, a rare condition, also typically presents with hip pain and limp n The diagnosis of osteomyelitis may be strongly suggested by plain film, bone scan, or MRI n
Hip pain (infection) n n n Transient synovitis — Transient synovitis (TS) is a relatively common disorder characterized by pain and limitation of motion in the hip Legg-Calvé-Perthes — Legg-Calvé-Perthes disease is a syndrome of idiopathic osteonecrosis (avascular necrosis) of the hip (familiar hx) Slipped epiphysis — In slipped capital femoral epiphysis (SCFE), the femoral epiphysis slips posteriorly, resulting in a limp and impaired internal rotation (obese child)
Pyomyositis n n Pyomyositis is a bacterial infection of skeletal muscle characterized by muscle pain and swelling Tropical pyomyositis has two age peaks: two to five years and 35 to 40 years Staphylococcus aureus is the predominant organism PATHOGENESIS — Bacterial invasion of muscle is assumed to occur after transient bacteremia leads to seeding of a site of prior muscle injury. Infection of the gastrointestinal, urinary respiratory tracts, or of indwelling catheters may predispose to bacteremia with secondary pyomyositis
pyomyositis Pyomyositis typically affects large skeletal muscles such as the thigh, calf, and, less often, gluteal regions n Pyomyositis should be suspected in patients with localized pain and usually fever n
Pyomyositis staging n n n Stage 1 is characterized by crampy local muscle pain, swelling, and low-grade fever. Mild leukocytosis and induration of the affected muscle may be present. no obvious signs on physical examination. Stage 2 occurs 10 to 21 days after the onset of symptoms and is characterized by fever, exquisite muscle tenderness, and edema. Marked leukocytosis is usually present, and eosinophilia is common in tropical pyomyositis. Aspiration of the affected muscle typically yields pus. More than 90 percent of the patients are seen at this suppurative stage. Stage 3 is characterized by bacteremia and a toxic appearance. The affected muscle is fluctuant. Complications of S. aureus bacteremia such as septic shock, endocarditis, pneumonia, pericarditis, septic arthritis, brain abscess, and acute renal failure may be present. Rhabdomyolysis complicating pyomyositis has been described
n Thank you !!