PEA arrest Chest compressions arent enough Susan P


 Andrew E Resuscitation 85:")








 Bergum D, et al. Resuscitation 87: 63, 2015. Total")







- Slides: 23
PEA arrest: Chest compressions aren’t enough Susan P. Torrey, MD, FAAEM, FACEP Associate Professor of Emergency Medicine UMass Medical School – Baystate Medical Center
I have nothing to declare, but… www. Torrey. EKG. com
Outcomes following out-of-hospital cardiac arrest with asystole or PEA (Australia) Andrew E Resuscitation 85: 1633 -1639, 2014 • 38, 378 non-shockable OHCA / 10 years – 12% PEA – Survival to hospital discharge – 6% • No trend toward improved survival over 10 years – Follow-up at 1 year • Death, vegetative state or severe disability – 45% 150 patients survived PEA arrest without severe disability at 1 year
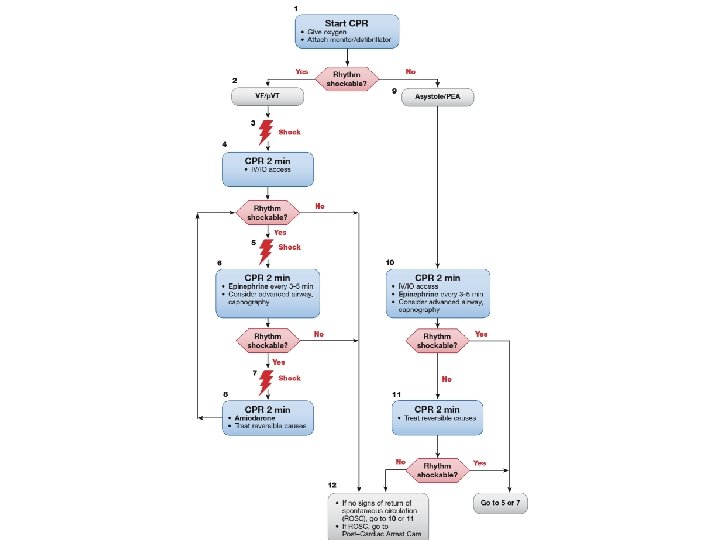
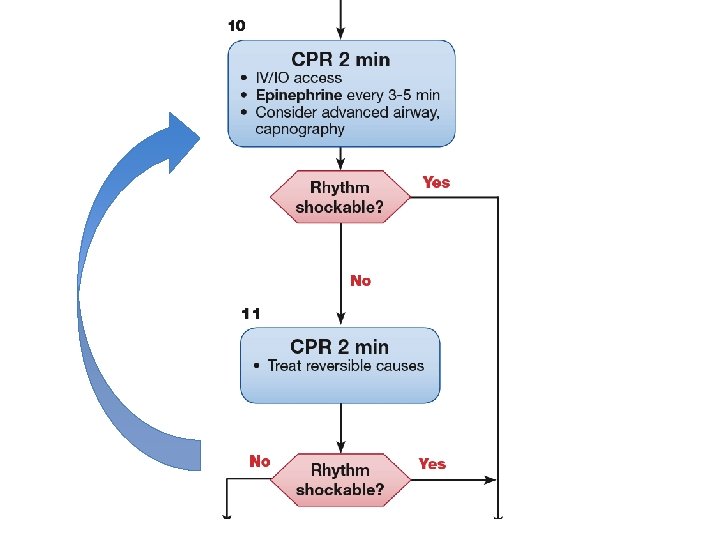
PEA…what next?
5 H’s and 5 T’s • • • Hypovolemia Hypoxia Hyperkalemia Hypothermia H+ ions (acidosis) • • • Tension pneumothorax Tamponade Toxins Thrombosis (PE) Thrombosis (MI)
Pulseless Electrical Activity • SCA -- >300, 000 cases/year in US – Accounts for 50% of cardiovascular deaths – PEA/asystole #’s have NOT changed in 30 years – Reduction in VT/VF during same interval • Subsets – Non-cardiac (5 H’s & 5 T’s) – Cardiac • Primary – initial rhythm • Secondary – following shock of VT/VF
Factors associated with out-of-hospital cardiac arrest with PEA: population-based study Ko DT Am Heart J 177: 129 -137, 2016 • Toronto, 2005 -2010, nontraumatic cardiac arrest • 9, 882 patients – 24% PEA 26% shockable 50% asystole • Patients with PEA vs shockable rhythm – Older (age 72 vs 65) – More likely female (41% vs 22%) – More comorbid diagnoses – More recent healthcare (ED 1 month 20% vs 10%)
ECG patterns in early PEA Bergum D, et al. Resuscitation 104: 34, 2016
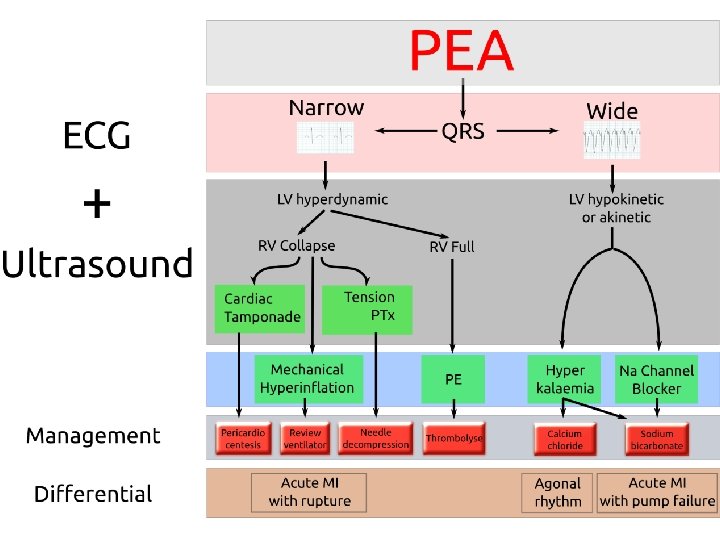
RUSH exam Rapid Ultrasound in Shock Cardiac IVC & Lungs Aorta - Tamponade - IVC collapsibility - Aorta - LV size and fx - Lungs ? pneumo - Legs ? DVT - RV size ? PE - Abd ? free fluid
PEA in PE thrombolysis Sharifi M, et al. Am J Emerg Med 34: 1963, 2016 • • • 23 pts with PEA receiving CPR due to massive PE Rx 50 mg t. PA IV push in 1 minute during CPR Initiation of CPR to t. PA was 6. 5 ± 2. 1 min (all IHCA) 22/23 pts - ROSC in 2 – 15 min after t. PA At 22 ± 3 months – 20 pts alive (87%) – Survivors all returned to pre-event functional capacity • Low-dose systemic t. PA at 50 mg is very safe – No major bleeding – Safe to administer as bolus over 1 minute
Causes of in-hospital cardiac arrest Bergum D, et al. Resuscitation 87: 63 -68, 2015. • 302 episodes over 5 years at 1000 -bed hospital • Causes of arrest – Cardiac causes – 60% – Hypoxia – 20% PE Hypovolemia – 8% Tamponade – 6% – 5% • Survived to hospital discharge – 25% – VT/VF – 53% – PEA – 13% – Asystole – 17%
Initial rhythm in PEA (IHCA) Bergum D, et al. Resuscitation 87: 63, 2015. Total n = 302
If we are going to improve survival in PEA arrest… • EMS has to return to “scoop and run” – Excellent CPR and IV fluid resuscitation – Beyond ACLS – think hyperkalemia, hypoxia • Early diagnostic ultrasound and interventions
CPR isn’t enough, but it is important • Improved blood flow during CPR results in survival – Mechanical CPR devices – consistency • Monitoring cardiac function during CPR – Echocardiographiy for – End-tidal CO 2 > 16 mm. Hg – predicts survival • Pharmacological interventions – Epinephrine vs. vasopressin – Atropine no longer recommended SOS-KANTO study (2011) - 30 -day survival
If we are going to improve survival in PEA arrest… • EMS has to return to “scoop and run” – Excellent CPR and IV fluid resuscitation – Beyond ACLS – think hyperkalemia, hypoxia • Early diagnostic ultrasound and interventions • If all else fails ECMO in certain situations
VA-ECMO • Cannulation – During CPR – For cardiogenic shock – Shock after ROSC / CPR • Complications – CVA – Acute renal failure – Major bleeding
Extracorporeal CPR for IHCA Singal RK, et al. Can J Card 33: 51, 2017 • ELSO (Extracorporeal Life Support Org) – 2379 cases E-CPR with 30% survival to discharge • Initiation ECMO < 30 minutes • V tach/v fib >> PEA • Age < 65 years – Bridging to: • CABG, myocardial recovery, insertion LVAD, transplant • PE, cardiotoxic OD, hypothermia
Indications: CA refractory to ACLS of suspected reversible origin: Cardiac, PE, toxins, hypothermia - Age < 65 Witnessed CA CPR <40 min Reversible cause - + Contraindications: - Asystole as initial rhythm - ETCO 2 < 13 - Lactate > 13 - Prior poor prognosis - Unavailability of team Medical Management - E-CPR + Singal R, at al. Can J Card 2017
Summary PEA is a spectrum of disease CPR must be very good Attempt IV fluid resuscitation Early identification of reversible causes – Decrease pre-hospital times – ± rhythm analysis – Ultrasound evaluation – RUSH • ECMO for a select group • •