PCSK9 Inhibitors Paul J Kovack DO FACC FACOI

PCSK-9 Inhibitors Paul J Kovack, DO, FACC, FACOI

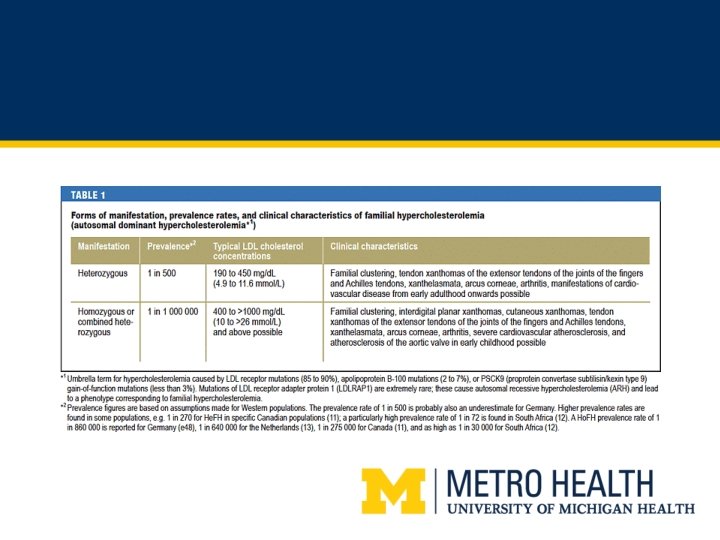
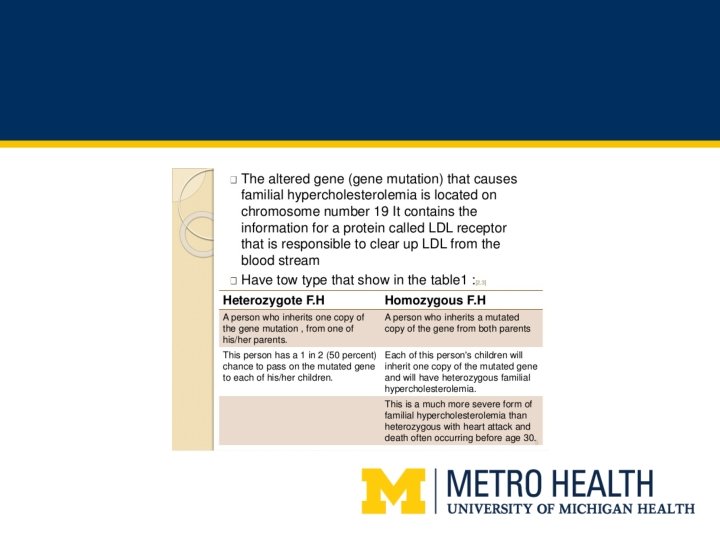
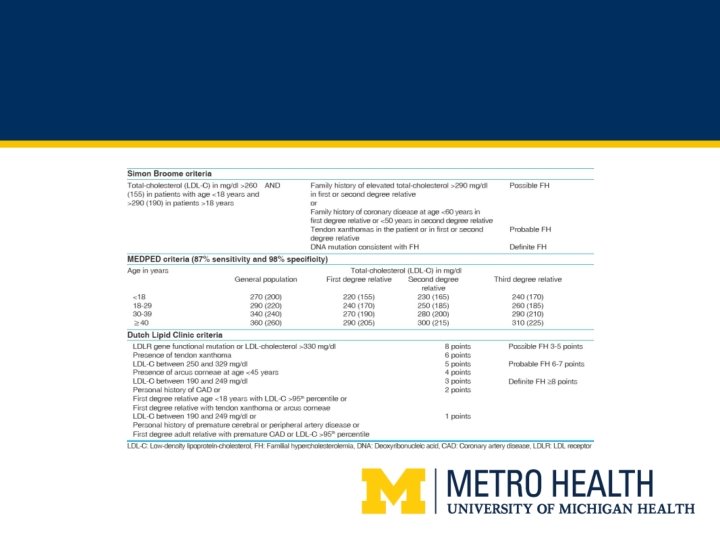
Diagnosis of He. FH • • Lipid screening Phenotypic characteristics Heterozygous versus Homozygous Family history British Simon Broome Registry MED PED Dutch Lipid Clinic criteria

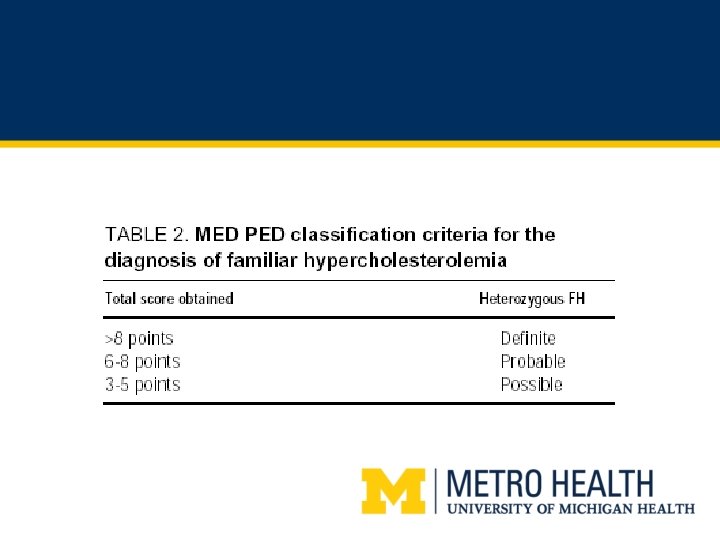
MED PED score

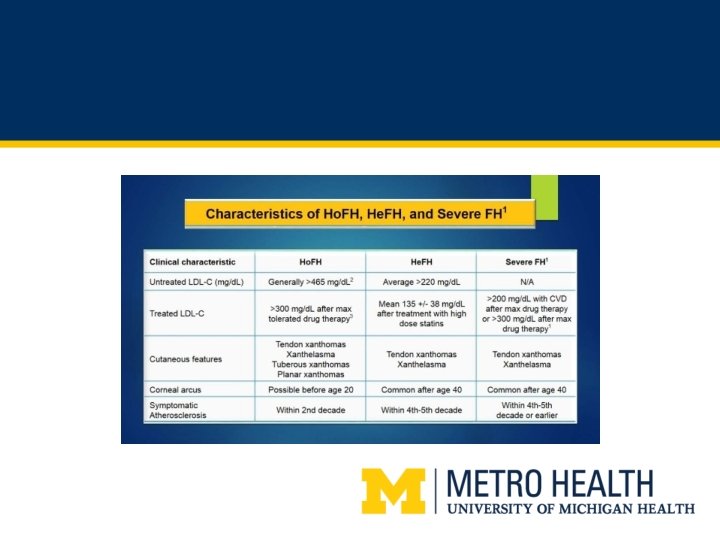
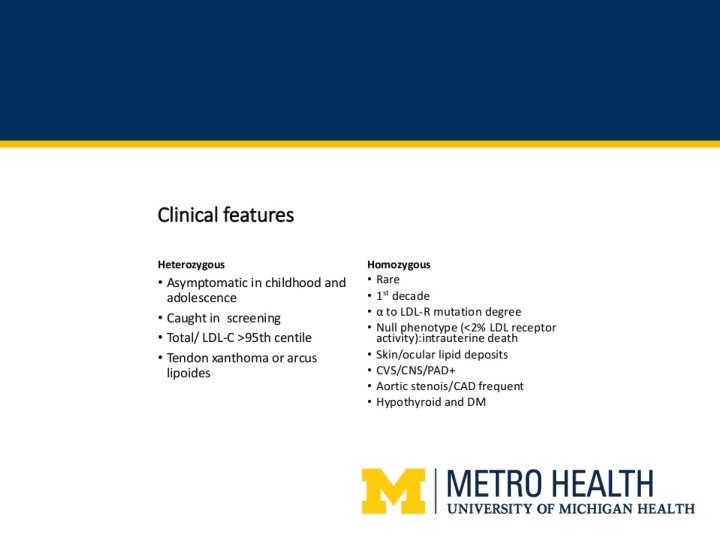
Phenotypic characteristics He. FH

Phenotypic characteristics He. FH

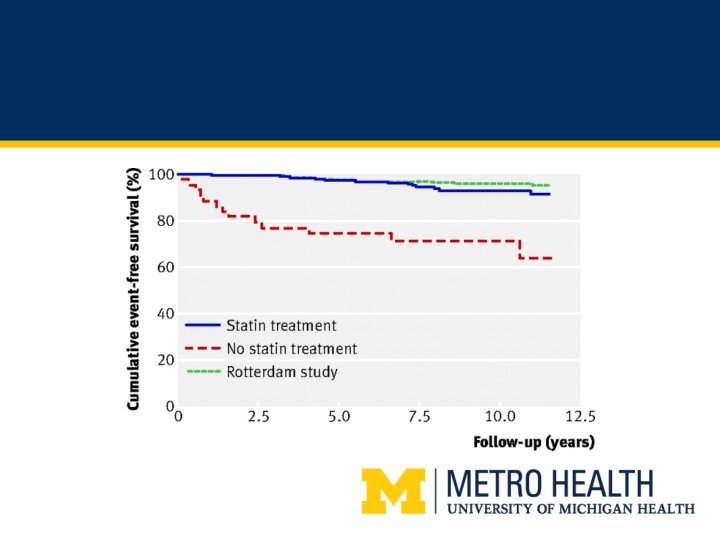
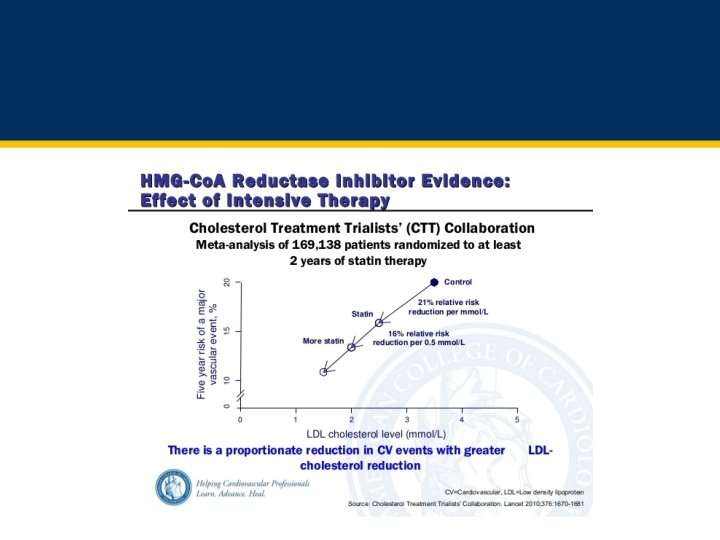
CV events and LDL
 • • Bile Acid Sequestrates")
Medications currently indicated for Heterogeneous Familial Hyperlipidemia (He. FH) • • Bile Acid Sequestrates Statins Ezetimibe PCSK 9 inhibitors

Diet and He. FH • Limit alcohol intake • Low calorie diet with total fat intake less that 3 percent
 • Hunters and gatherers, fishing, farming • 85%")
Exercise • The Bolivians (the Tsimane) • Hunters and gatherers, fishing, farming • 85% aged 45 to 90 had no coronary calcium. 13% had scores less than 100 • Average LDL was 92 and HDL was 40 • ACC/AHA Current recommendations are 30 minutes moderate exercise 5 times per week

Let’s get real about diet. Important to set appropriate expectations regarding LDL and diet with our patients • MEGA Trial, decreased LDL cholesterol by only 3% (Pravastatin is same trial decreased LDL by 18%) • Dean Ornish (diet, exercise, stress reduction, and social support) can decrease LDL by almost 40% (But TOUGH!) • Vegan diet (JAHA October, 2015) Tchol decreased by 14 mg/dl, LDL reduced by 13 mg/dl • Overall, expect a person who is very motivated with their diet to drop their cholesterol by 5 -10%

Helpful information for your patients: Diet in addition to appropriate medical therapy • DASH Diet • Mediterranean diet: The South Beach Diet • Vegan diet: Prevent and Reverse Heart Disease (Caldwell B Esselstyn, Jr, MD) • Dean Ornish Diet: Reversing Heart Disease
")
PREDIMED • N Eng J med 2013; 368: 1279 -1290 • Mediterranean diet (MD) vs MD plus 1 tablespoon olive oil per day vs 1 handful of tree nuts per day • 7500 patients followed for 5 years • Endpoint was MI, stroke or death (MACE) • Either group, olive oil or tree nuts were 30% Less likely to achieve the major endpoint (driven primarily by stroke)

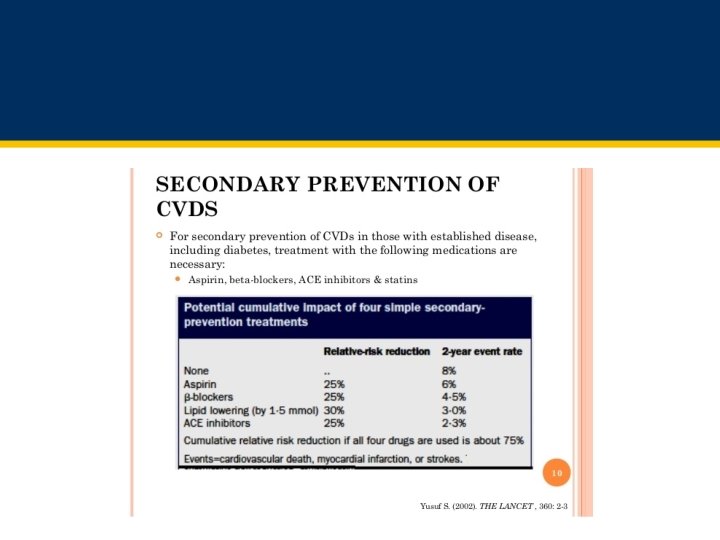
Medications that are indicated for secondary prevention of CAD and PAD • • • Statins ASA ACEI Beta blockers Plavix

Effect of statins on mortality in patients with CAD

Lower is better: There is no too low!

Statin Intolerant Patients have worse prognosis after MI JACC 2017; 69: 1386 -95 • Increased risk for recurrent MI and CHD events • Statin discontinuation associated with elevated risk of ischemic stroke, all cause mortality, all major events and any hospitalization • 50% increased risk of MI • 51% increased risk of all CV events

Outcomes in patients who discontinued vs maintained statins after stroke JAHA 2017; doi: 10. 1161 Outcome Discontinued group Maintained group Adjusted Risk (95% CI) Ischemic Stroke 5. 6% 3. 9% 1. 45 All-cause mortality 1. 4% 1% 1. 37 All major events 7. 8% 5. 6% 1. 38 Any hospitalization 31. 7% 27. 1% 1. 19

What is the nocebo effect? • nonpharmacological, harmful, or undesirable effects occurring after active or inactive therapy • frequency of adverse events can dramatically increase by informing patients about the possible side effects of the treatment, and by negative expectations on the part of the patient • eg; Patients who were told that they might experience sexual side effects after treatment with β-blocker drugs reported these symptoms between three and four times more often than patients in a control group who were not informed about these symptoms

What is the nocebo effect? • ASCOT-LLA trial, 10, 000 patients – Almost all had never been on a statin before • Blinded phase events muscle related events similar between groups (2%) • Unblinded phase AE when patients knew they were on a statin, incidents of myalgias rose 41%

Treating Statin Intolerance • • 1 -5% in clinical studies 11 -29% in observational cohorts Nocebo Effect Change dose, change statin Hydration Exercise, stretching supplements

Cleveland Clinic Observational Study of Statin intolerant Patients • 1600 patients referred with history of statin intolerance • 73% remained on statin therapy for 31 months – 63% daily dosing – 9% intermittent dosing • Lower dose • Different statin • Combine with zetia or BAS

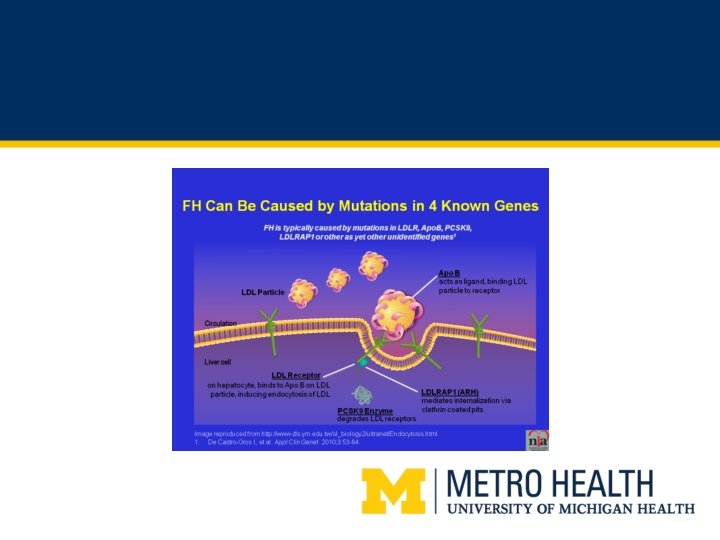
Mechanism of PCSK-9 inhibitors • LDL receptors bind to LDL in the liver and remove LDL paticles • LDL-R then return to cell surface to repeat the process • PCSK 9 binds to the LDL-R and promotes degradation • Block PCSK 9 and increase availability or LDL -R to remove LDL from the circulations
 He. FH")
Current Approved Indications of PCSK 9 inhibitors in the US Praluent (alirocumab) He. FH or CVD Adjunct to diet and maximally tolerated statin for treatment of adults with He. FH or clinical atherosclerotic CVD who require additional lowering of LDL-C Repatha (evolocumab) He. FH or CVD Adjunct to diet and maximally tolerated statin for treatment of adults with He. FH or clinical atherosclerotic CVD who require additional lowering of LDL-C Ho. FH Adults and adolescents > 13 years with Ho. FH in combination with other lipid lowering therapies

Samples of efficacy of PCSK 9 inhibitors an a small group of the trials done thus far Trial Drug Result LONG TERM Alirocumab in addition to maximally tolerated LLT LDL reduced by 61% vs placebo COMBO II Alirocumab in addition to maximally tolerated LLT LDL reduced by 50. 6% CHOICE I Alirocumab in addition to maximally tolerated LLT LDL reduced by 58. 7% LAPLACE-2 Evolocumab +/-statin LDL reduced by 75% GAUSS-2 Trial Evolocumab, statin intolerant LDL reduced by 56% RUTHERFORD-2 Trial Evolocumab in He. FH on maximally tolerated LLT LDL reduced by 60%

PCSK 9 – The good • Highly effective, up to 70% reduction in LDL • Safe • Well tolerated

PCSK 9 – The Bad • Adverse events – Muscle related symptoms similar to placebo – Rhabdomyolysis 0. 1%, same as placebo – Transaminases greater than 3 times normal 1. 5%, same as placebo – Creatine kinase greater than 5 times 0. 7%, same as placebo. • Injection site reactions (2. 1% vs 1. 6% in placebo) • In trials, discontinuation rates the same for drug vs placebo • Limited outcomes data for CV events

PCSK 9 – The Ugly • Sticker shock -$14, 000 per year • Overcoming this barrier is difficult and time intensive but there is help – Copay cards – Proper documentation • Diagnosis details • Recent lipid panel • History of other lipid lowering treatments – Appeals

Insurance Coverage • Patient has established CVD • Patient has tried high efficacy statin and failed to get LDL less than 100 mg/dl (or less than 70 mg/dl) • May also require adding Zetia first

Amgen Safety Net Foundation can cover at no cost up to 500% federal poverty level (FPL) 1 -844 -REPATHA Family Size 100% FPL 500% FPL 1 $12, 060 $60, 300 2 $16, 240 $81, 200 3 $20, 420 $102, 100 4 $24, 600 $123, 000

GAUSS-3 trial • 511 patients intolerant to 3 or more statins • Randomized to zetia vs PCSK 9 inhibitor • No difference in muscle related side effects • 53% reduction LDL evolocumab • 17% reduction with zetia

FOURIER Trial N Eng J Med 2017; 376: 1713 -1722 • 1242 sites in 49 countries • 27, 564 patients • Patients with prior MI, stroke, and/or symptomatic PAD with 70 mg/dl or higher LDL on high or moderate efficacy statin • Repatha 140 mg every 2 weeks or 420 mg every month vs placebo average FU 2. 5 years • Primary endpoint major CV event (MI, stroke, CV death, hospitalization for USA or coronary revascularization
")
FOURIER Trial: Results • Primary endpoint, ARR 1. 5% (11. 3 vs 9. 8%) 15% RRR • Secondary endpoint CV death, MI stroke (MACE) ARR 1. 5% (9. 9 vs 7. 9%) 20% RRR • Extra 59% reduction of LDL beyond statin alone (median 92 mg/dl to 30 mg/dl)

FOURIER Trial • No difference in /adverse events • Rare injection site reactions • Discontinuation rate similar between each group

FOURIER trial: Results in PAD • PAD without history of stroke or MI, MACE events with placebo 10. 3% (7. 6% if MI or Stroke but no PAD) – Treatment group had event rate of 5. 5% – NNT 21 for 2. 5 years • PAD with history of MI or stroke, MACE events was 14. 9% – Treatment group had event rate of 11. 4% – NNT 29 for 2. 5 years
 in")
FOURIER trial: Results in PAD • MACE or MALE* (major adverse leg events) in patients with PAD but no MI or stroke was 12. 8% in control goupd and 6. 5% of treatments group. – 6. 3 absolute risk reduction • NNT 16. • Bottom line, get LDL as low as possible inpatients with PAD. • *MALE includes: acute limb ischemia, major amputation or urgent revascularization

ODYSSEY Outcomes study • 18, 000 patients post ACS patients randomized to alirocumab • Results due early 2018

PCSK 9 Inhibitors, Economics and Policy JACC 2017; 70: 2677 -87 • “The list prices of PCSK 9 inhibitors in the United States are over 100 -fold higher than statins, and only a small fraction of their higher cost will ever be recouped by prevention of cardiovascular events, especially in lower-risk patients. The projected cost-effectiveness of PCSK 9 inhibitors does not meet generally accepted benchmarks for good value, but would improve if their prices were cut substantially. ”

How can we best help our patients with He. FH and CAD and PAD? • Get them on the right medications and work with them to make sure they tolerate them (and can afford them) and therefore, stay on them. • Strive to be evidence based and guideline driven • Keep your patients focused on statin benefits • Remember the nocebo effect • Remember what the Cleveland Clinic accomplished • Fourier Trial and more to come regarding PCSK 9 inhibitors

- Slides: 52