PCICS December 10 2014 Surgical Considerations for Patients

PCICS December 10, 2014 Surgical Considerations for Patients with Heterotaxy Syndrome Jeffrey P. Jacobs, M. D. , FACS, FACC, FCCP Professor of Surgery, Johns Hopkins University Director, Andrews/Daicoff Cardiovascular Program, Surgical Director of Heart Transplantation and Extracorporeal Life Support Programs,

Disclosure 1. Chair of the STS Database Access and Publications Taskforce 2. Chair of the STS Database Task Force on Longitudinal Follow-up and Linked Registries 3. Chair of the STS Database Public Reporting Task Force

Objectives • Define Heterotaxy Syndrome • Understand the “outcomes” of surgical procedures commonly performed patients with Heterotaxy Syndrome

Two Manuscripts Jacobs JP, Anderson RH, Weinberg P, Walters III HL, Tchervenkov CI, Del Duca D, Franklin RCG, Aiello VD, Béland MJ, Colan SD, Gaynor JW, Krogmann ON, The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. In 2007 Supplement to Cardiology in the Young: Controversies Kurosawa H, Maruszewski B, Stellin G, Elliott MJ. and Challenges Facing Paediatric Cardiovascular Practitioners and their Patients, Anderson RH, Jacobs JP, and Wernovsky G, editors. Cardiology in the Young. 2007 Sept; 17(Suppl 2): 1– 28, doi: 10. 1017/S 1047951107001138. . Jacobs JP, Pasquali SK, Morales DLS, Jacobs ML, Mavroudis C, Chai PJ, Tchervenkov CI Heterotaxy: Lessons Learned About Patterns of Practice and Outcomes From the Congenital Heart Surgery Database of the Society of Thoracic Surgeons. The World Journal for Pediatric and Congenital Heart Surgery Lacour-Gayet FG, Walters III H, Quintessenza JA. (WJPCHS). 2011 April; 2(2): 278 -286. DOI: 10. 1177/2150135110397670.
 1. Atrial arrangement, 2. Atrioventricular connections, and")
Cardiac Connections – Sequential Segmental Approach (Anderson) 1. Atrial arrangement, 2. Atrioventricular connections, and 3. Ventriculoarterial connections

Atrial Arrangement Robert Anderson

Atrioventricular Connections Robert Anderson
 • Discordant")
Atrioventricular Connections • Normal atrioventricular connections (Concordant atrioventricular connections in biventricular heart) • Discordant AV connections • Absent left sided AV connection • Absent right sided AV connection • Double inlet AV connection, Double inlet LV • Double inlet AV connection, Double inlet RV • Mixed ("Ambiguous") AV connections (biventricular)
 • Discordant")
Ventriculoarterial Connections • Normal ventriculoarterial connections (Concordant ventriculoarterial connections in biventricular heart) • Discordant VA connections (TGA) • Single outlet VA connection, Common arterial trunk • Single outlet VA connection, Single outlet VA connection via aorta (pulmonary atresia) • Single outlet VA connection, Single outlet VA connection via pulmonary trunk (aortic atresia) • Double outlet VA connections, Double outlet LV • Double outlet VA connections, Double outlet RV • Concordant VA connections with parallel great arteries (anatomically corrected malposition)
 Robert H. Anderson, Paul M. Weinberg.")
Concordant Atrioventricular Connections with Discordant Ventriculoarterial Connections (TGA) Robert H. Anderson, Paul M. Weinberg. The clinical anatomy of transposition. In: Jacobs JP, Wernovsky G, Gaynor JW, and Anderson RH (editors). 2005 Supplement to Cardiology in the Young: Controversies of the Ventriculo-Arterial Junctions and Other Topics, Cardiology in the Young, Volume 15, Supplement 1: 1 - 198, February 2005.

Jacobs JP, Anderson RH, Weinberg P, Walters III HL, Tchervenkov CI, Del Duca D, Franklin RCG, Aiello VD, Béland MJ, Colan SD, Gaynor JW, Krogmann ON, Kurosawa H, Maruszewski B, Stellin G, Elliott MJ. The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. In 2007 Supplement to Cardiology in the Young: Controversies and Challenges Facing Paediatric Cardiovascular Practitioners and their Patients, Anderson RH, Jacobs JP, and Wernovsky G, editors. Cardiology in the Young. 2007 Sept; 17(Suppl 2): 1– 28, doi: 10. 1017/S 1047951107001138. . • Specification of the atrial arrangement, the atrioventricular connections, and the ventriculoarterial connections, does not specify nor imply the ventricular topology, or the relationships of the cardiac chambers and great arteries in space. These variables are separately specified.
 1. the sidedness of the")
Cardiac Relations - Segmental Approach (Van Praagh & Vlad) 1. the sidedness of the atrial chambers, or, in other words, the atrial “situs”, 2. the ventricular topology, in other words, the ventricular “loop”, and 3. the relationships of the arterial trunks in space
 • The viscera and atria:")
Cardiac Relations - Segmental Approach (Van Praagh & Vlad) • The viscera and atria: The types of visceroatrial situs – S solitus – I inversus – A ambiguus • The ventricular topology – D D-loop ventricles, – L L-loop ventricles • Great vessels: The great arterial position – S solitus – I inversus – D dextro – L levo

Visceral Situs William T. Mahle, MD Associate Professor of Pediatrics Emory University School of Medicine

Norman H Silverman Stanford University Lucile Packard Children’s Hospital

Robert Anderson Morphologically Right Ventricle

Robert Anderson Morphologically Left Ventricle

VENTRICULAR TOPOLOGY – Robert Anderson Right hand Left hand

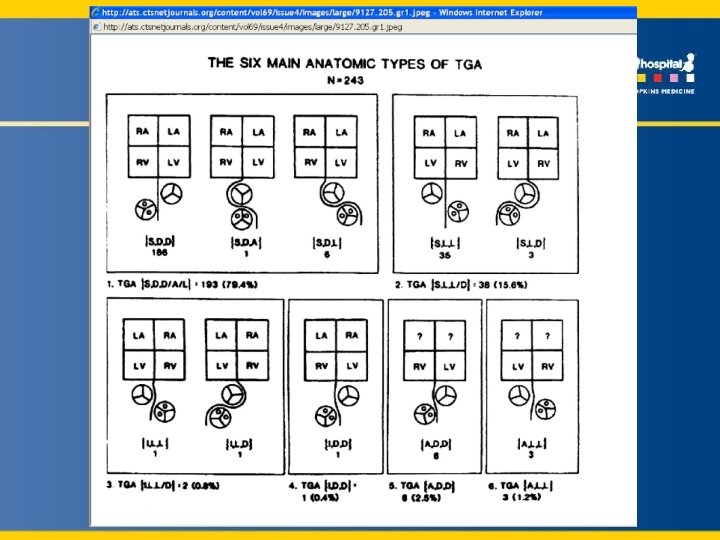
Jaggers JJ, Cameron DE, Herlong JR, et al: The Society of Thoracic Surgeons Congenital Heart Surgery Nomenclature and Database Project: transposition of the great arteries, Ann Thorac Surg 69(suppl): S 205, 2000. In: Mavroudis C, Jacobs JP. Congenital Heart Surgery Nomenclature and Database Project: Ann Thorac Surg. 2000 Apr; 69(4 Suppl): S 1 -372. Anatomic types of transposition of the great arteries (TGA) as described by Van Praagh and colleagues The anatomic subtypes that are included in this nomenclature include: » TGA {S, D, D}; » TGA {S, D, A}; » TGA {S, D, L}; » TGA {I, L, D}; » {A, L, L} » {A, D, D} (Those with situs ambiguous technically cannot be TGA as described by Van Praagh, but may be physiologically

Jacobs JP, Anderson RH, Weinberg P, Walters III HL, Tchervenkov CI, Del Duca D, Franklin RCG, Aiello VD, Béland MJ, Colan SD, Gaynor JW, Krogmann ON, Kurosawa H, Maruszewski B, Stellin G, Elliott MJ. The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. In 2007 Supplement to Cardiology in the Young: Controversies and Challenges Facing Paediatric Cardiovascular Practitioners and their Patients, Anderson RH, Jacobs JP, and Wernovsky G, editors. Cardiology in the Young. 2007 Sept; 17(Suppl 2): 1– 28, doi: 10. 1017/S 1047951107001138. . • Specification of the atrial “situs”, the ventricular “loop”, and the relationships of the arterial trunks in space does not specify the atrioventricular and ventriculoarterial connections. These variables are separately specified.

Cardiac Position

Cardiac Position Can be surgically important – for example – Pathway for extracardiac Fontan • • Dextrocardia (right sided ventricular mass) Levocardia (left sided ventricular mass) Mesocardia (central/midline ventricular mass) Dextroversion (ventricular apex points to the right) • Levoversion (ventricular apex points to the left)

Jacobs JP, Anderson RH, Weinberg P, Walters III HL, Tchervenkov CI, Del Duca D, Franklin RCG, Aiello VD, Béland MJ, Colan SD, Gaynor JW, Krogmann ON, Kurosawa H, Maruszewski B, Stellin G, Elliott MJ. The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. In 2007 Supplement to Cardiology in the Young: Controversies and Challenges Facing Paediatric Cardiovascular Practitioners and their Patients, Anderson RH, Jacobs JP, and Wernovsky G, editors. Cardiology in the Young. 2007 Sept; 17(Suppl 2): 1– 28, doi: 10. 1017/S 1047951107001138. . “Heterotaxy is synonymous with “visceral heterotaxy” and “heterotaxy syndrome”. Heterotaxy is defined as an abnormality where the internal thoraco-abdominal organs demonstrate abnormal arrangement across the left-right axis of the body. By convention, heterotaxy does not include patients with either the expected usual or normal arrangement of the internal organs along the left-right axis, also known as “situs solitus”, nor patients with complete mirrorimaged arrangement of the internal organs

LATERALIZED BODILY ARRANGEMENT 1 2 3 RAA 1 1 2 2 L om h c a St Usual 2 3 RAA LAA r ive 1 n e e l p S Robert Anderson Sp le en St Liv om ac er h Mirror-imagery Supported by:

Isomerism In chemistry, isomers are defined as different compounds that have the same molecular formula. Isomers are classified as enantiomers when their molecules are mirror reflections of each other.

Jacobs JP, Anderson RH, Weinberg P, Walters III HL, Tchervenkov CI, Del Duca D, Franklin RCG, Aiello VD, Béland MJ, Colan SD, Gaynor JW, Krogmann ON, Kurosawa H, Maruszewski B, Stellin G, Elliott MJ. The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. In 2007 Supplement to Cardiology in the Young: Controversies and Challenges Facing Paediatric Cardiovascular Practitioners and their Patients, Anderson RH, Jacobs JP, and Wernovsky G, editors. Cardiology in the Young. 2007 Sept; 17(Suppl 2): 1– 28, doi: 10. 1017/S 1047951107001138. . “Isomerism in the context of the congenitally malformed heart is defined as a situation where some paired structures on opposite sides of the left-right axis of the body are, in morphologic terms, symmetrical mirror images of

VISCERAL HETEROTAXY 1 1 2 3 1 1 2 2 ? ? Mid-line Liver Malrotated gut “Asplenia” “Polysplenia” Robert Anderson Supported by:

Isomeric Lungs

Isomeric Bronchial Arrangements

Jacobs JP, Anderson RH, Weinberg P, Walters III HL, Tchervenkov CI, Del Duca D, Franklin RCG, Aiello VD, Béland MJ, Colan SD, Gaynor JW, Krogmann ON, Kurosawa H, Maruszewski B, Stellin G, Elliott MJ. The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. In 2007 Supplement to Cardiology in the Young: Controversies and Challenges Facing Paediatric Cardiovascular Practitioners and their Patients, Anderson RH, Jacobs JP, and Wernovsky G, editors. Cardiology in the Young. 2007 Sept; 17(Suppl 2): 1– 28, doi: 10. 1017/S 1047951107001138. . “Isomerism of the right atrial appendages is a subset of heterotaxy where the atrial appendages on both sides of the body have the appearance of the morphologically right atrial appendage. ”

Jacobs JP, Anderson RH, Weinberg P, Walters III HL, Tchervenkov CI, Del Duca D, Franklin RCG, Aiello VD, Béland MJ, Colan SD, Gaynor JW, Krogmann ON, Kurosawa H, Maruszewski B, Stellin G, Elliott MJ. The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. In 2007 Supplement to Cardiology in the Young: Controversies and Challenges Facing Paediatric Cardiovascular Practitioners and their Patients, Anderson RH, Jacobs JP, and Wernovsky G, editors. Cardiology in the Young. 2007 Sept; 17(Suppl 2): 1– 28, doi: 10. 1017/S 1047951107001138. . “Isomerism of the left atrial appendages is a subset of heterotaxy where the atrial appendages on both sides of the body have the appearance of the morphologically left atrial appendage. ”

Jacobs JP, Anderson RH, Weinberg P, Walters III HL, Tchervenkov CI, Del Duca D, Franklin RCG, Aiello VD, Béland MJ, Colan SD, Gaynor JW, Krogmann ON, Kurosawa H, Maruszewski B, Stellin G, Elliott MJ. The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. In 2007 Supplement to Cardiology in the Young: Controversies and Challenges Facing Paediatric Cardiovascular Practitioners and their Patients, Anderson RH, Jacobs JP, and Wernovsky G, editors. Cardiology in the Young. 2007 Sept; 17(Suppl 2): 1– 28, doi: 10. 1017/S 1047951107001138. . “Situs ambiguus is defined as an abnormality in which there are components of situs solitus and situs inversus in the same person. Situs ambiguus, therefore, can be considered to be present when the thoracic and abdominal organs are positioned in such a way with respect to each other as to be not clearly lateralised and thus have neither the usual, or normal, nor the mirror-imaged arrangements. ”

Jacobs JP, Anderson RH, Weinberg P, Walters III HL, Tchervenkov CI, Del Duca D, Franklin RCG, Aiello VD, Béland MJ, Colan SD, Gaynor JW, Krogmann ON, Kurosawa H, Maruszewski B, Stellin G, Elliott MJ. The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. In 2007 Supplement to Cardiology in the Young: Controversies and Challenges Facing Paediatric Cardiovascular Practitioners and their Patients, Anderson RH, Jacobs JP, and Wernovsky G, editors. Cardiology in the Young. 2007 Sept; 17(Suppl 2): 1– 28, doi: 10. 1017/S 1047951107001138. . “Asplenia syndrome” can be defined as a subset of heterotaxy with components of bilateral right -sidedness, usually associated with absence of the spleen.

Jacobs JP, Anderson RH, Weinberg P, Walters III HL, Tchervenkov CI, Del Duca D, Franklin RCG, Aiello VD, Béland MJ, Colan SD, Gaynor JW, Krogmann ON, Kurosawa H, Maruszewski B, Stellin G, Elliott MJ. The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. In 2007 Supplement to Cardiology in the Young: Controversies and Challenges Facing Paediatric Cardiovascular Practitioners and their Patients, Anderson RH, Jacobs JP, and Wernovsky G, editors. Cardiology in the Young. 2007 Sept; 17(Suppl 2): 1– 28, doi: 10. 1017/S 1047951107001138. . “Polysplenia syndrome” can be defined as a subset of heterotaxy with components of bilateral leftsidedness, usually associated with multiple spleens.

Complete description of both the cardiac relations and connections: 1. 2. 3. 4. 5. 6. 7. 8. 9. the arrangement of the atrial appendages the ventricular topology the atrioventricular connections the ventriculoarterial connections the infundibular morphologies the relationships of the arterial trunks in space the position of the heart in the chest the orientation of the cardiac apex In heterotaxy, particular attention is required for the venoatrial connections, since these are so often abnormal.

Heterotaxy • • Nomenclature is important Less than perfect association between the state of the spleen and the form of heart disease. • Splenic morphology should be investigated in all forms of heterotaxy, regardless of the type of cardiac disease. • The splenic morphology should not be used to stratify the form of disease within the heart • The form of cardiac disease should not be used to stratify the state of the spleen.

The Report of the 2010 STS Congenital Heart Surgery Practice and Manpower Survey ♥ undertaken by the Society of Thoracic Surgeons Workforce on Congenital Heart Surgery ♥ 125 centers in the United States of America perform pediatric and congenital heart surgery ♥ 8 centers in Canada perform pediatric and congenital heart surgery Jacobs ML, Daniel M, Mavroudis C, Morales DLS, Jacobs JP, Fraser CD, Turek JW, Mayer JE, Tchervenkov C, Conte JV. Report of the 2010 Society of Thoracic Surgeons Congenital Heart Surgery Practice and Manpower Survey. The Annals of Thoracic Surgery, 2011; 92: 762– 9, August 2011.

Growth in the STS Congenital Heart Surgery Database Participating Centers Per Harvest 120 100 80 60 40 20 0 Participating Centers 2002 16 2003 18 2004 21 2005 34 2006 47 2007 58 2008 68 2009 79 2010 93 2011 101 2012 105 2013 111 2014 114 Jacobs JP, Jacobs ML, Mavroudis C, Lacour-Gayet FG, Tchervenkov CI, Pasquali SK. Executive Summary: The Society of Thoracic Surgeons Congenital Heart Surgery Database - Twentieth Harvest – (January 1, 2009 – December 31, 2013). The Society of Thoracic Surgeons (STS) and Duke Clinical Research Institute (DCRI), Duke University Medical Center, Durham, North Carolina, United States, Spring 2014 Harvest.

Growth in the STS Congenital Heart Surgery Database Operations per averaged 4 year data collection cycle 160000 140000 120000 100000 80000 60000 40000 20000 0 Operations 2002 12787 2003 16461 2004 28351 2005 37093 2006 45635 2007 61014 2008 72002 2009 91639 2010 103664 2011 114041 2012 130823 2013 136617 2014 142933 Jacobs JP, Jacobs ML, Mavroudis C, Lacour-Gayet FG, Tchervenkov CI, Pasquali SK. Executive Summary: The Society of Thoracic Surgeons Congenital Heart Surgery Database - Twentieth Harvest – (January 1, 2009 – December 31, 2013). The Society of Thoracic Surgeons (STS) and Duke Clinical Research Institute (DCRI), Duke University Medical Center, Durham, North Carolina, United States, Spring 2014 Harvest.

Growth in the STS Congenital Heart Surgery Database Cumulative operations over time 350000 300000 250000 200000 150000 100000 50000 0 Cumulative Operations 2000 4237 2001 9747 2002 16537 2003 26404 2004 39988 2005 58181 2006 79399 2007 98406 2008 119266 2009 148110 2010 179697 2011 213416 2012 257932 2013 292828 2014 314674 Jacobs JP, Jacobs ML, Mavroudis C, Lacour-Gayet FG, Tchervenkov CI, Pasquali SK. Executive Summary: The Society of Thoracic Surgeons Congenital Heart Surgery Database - Twentieth Harvest – (January 1, 2009 – December 31, 2013). The Society of Thoracic Surgeons (STS) and Duke Clinical Research Institute (DCRI), Duke University Medical Center, Durham, North Carolina, United States, Spring 2014 Harvest.
 is")
STS Database Penetrance in USA • The STS Congenital Heart Surgery Database (STSCHSD) is the largest clinical database in the world for congenital and pediatric cardiac surgery. • The Report of the 2010 STS Congenital Heart Surgery Practice and Manpower Survey, undertaken by the STS Workforce on Congenital Heart Surgery, documented that 125 hospitals in the United States of America and 8 hospitals in Canada perform pediatric and congenital heart surgery. • The STS-CHSD contains data from 119 of the 125 hospitals (95. 2% penetrance by hospital) in the United States of America and 3 of the 8 centers in Canada.

Heterotaxy in the EACTS-STS Congenital Heart Surgery Databases: 10 TERMS • 3 Preoperative Factors • 7 Diagnostic terms

Heterotaxy in the EACTS-STS Congenital Heart Surgery Databases: 10 TERMS • 3 Preoperative Factors: 1. Heterotaxy syndrome 2. Heterotaxy syndrome, Asplenia syndrome 3. Heterotaxy syndrome, Polysplenia syndrome

Heterotaxy in the EACTS-STS Congenital Heart Surgery Databases: 10 TERMS • 7 Diagnostic terms 1. 2. 3. 4. 5. 6. 7. Single ventricle, Heterotaxia syndrome Atrial Isomerism, Left {CAN NOT BE PRIMARY DIAGNOSIS} Atrial Isomerism, Right {CAN NOT BE PRIMARY DIAGNOSIS} Dextrocardia {CAN NOT BE PRIMARY DIAGNOSIS} Levocardia {CAN NOT BE PRIMARY DIAGNOSIS} Mesocardia {CAN NOT BE PRIMARY DIAGNOSIS} Situs inversus {CAN NOT BE PRIMARY DIAGNOSIS}

Heterotaxy syndrome • Heterotaxy is synonymous with ‘visceral heterotaxy’ and ‘heterotaxy syndrome’. Heterotaxy is defined as an abnormality where the internal thoracoabdominal organs demonstrate abnormal arrangement across the left-right axis of the body. By convention, heterotaxy does not include patients with either the expected usual or normal arrangement of the internal organs along the left-right axis, also known as ‘situs solitus’, nor patients with complete mirrorimaged arrangement of the internal organs along the left-right axis also known as ‘situs inversus’.

Heterotaxy syndrome, Asplenia syndrome • “Asplenia syndrome” can be defined as a subset of heterotaxy with components of bilateral rightsidedness, usually associated with absence of the spleen.

Heterotaxy syndrome, Polysplenia syndrome • “Polysplenia syndrome” can be defined as a subset of heterotaxy with components of bilateral leftsidedness, usually associated with multiple spleens.

1. 2. 3. 4. 5. 6. 7. 8. Single Ventricle Single ventricle, DILV Single ventricle, DIRV Single ventricle, Mitral atresia Single ventricle, Tricuspid atresia Single ventricle, Unbalanced AV canal Single ventricle, Heterotaxia syndrome Single ventricle, Other Single Ventricle + Total anomalous pulmonary venous connection (TAPVC)

STS Congenital Heart Surgery Database • All Index Operations in Database over 12 years – January 1, 1998 - December 31, 2009 • Excludes participants with > 15% missing for discharge mortality or non-cardiac abnormalities, and individual records missing discharge mortality or non-cardiac abnormalities • Excludes patients weighing less than or equal to 2, 500 g undergoing PDA ligation as their primary procedure

STS Congenital Heart Surgery Database • 77, 153 total operations • 1, 144 with asplenia • 361 with polysplenia

Percentage Discharge Mortality All Index Operations in Database Asplenia Polysplenia No Asplenia or Polysplenia STS-EACTS Category 1 0. 5% 5. 5% 10. 6% 0. 5% STS-EACTS Category 2 1. 7% 4. 6% 7. 6% 1. 6% STS-EACTS Category 3 2. 7% 4. 3% 1. 7% 2. 6% STS-EACTS Category 4 8. 2% 15. 1% 14. 1% 7. 8% STS-EACTS Category 5 20. 8% 30. 8% 16. 1% 20. 4%

STS Congenital Heart Surgery Database • All Index Operations in Database over 12 years – January 1, 1998 - December 31, 2009 • Include all patients with Single Ventricle who underwent Shunt, Glenn, or Fontan • Excludes participants with > 15% missing for discharge mortality
 • 1669 Glenn")
STS Congenital Heart Surgery Database • 804 Shunt (148 with heterotaxy) • 1669 Glenn (201 with heterotaxy) • 1936 Fontan (240 with heterotaxy)

Percentage Discharge Shunt Mortality All Single Ventricle except Heterotaxy Single ventricle, Heterotaxia syndrome Glenn Fontan 7. 3% 1. 4% 2. 1% 6. 6% 1. 4% 1. 8% 10. 8% 1. 5% 4. 2%

Heterotaxy: Lessons learned from the STS Database 1. STS Database is largest Congenital Heart Surgery Database in North America 2. Review of Data allows for unique picture of Patterns of Practice and Outcome 3. Heterotaxy is a challenging problem with increased discharge mortality in most subgroups.

DATA

DATA is Power

- Slides: 59