Patients with Hyperprolactinemia Dr WONG Lap Ming 21


 • Female, 14 year old • Referred from Student Health Service for")
 • Slight breast development only in the past, but cannot recall exact")


 • Height 146")
 • • • Full blood count: normal ESR: 19 mm/1 st hour")
 • Morning 17 -OH progesterone: 0. 7 nmol/L ( ref 0. 64.")
 • CT scan brain: A large hyperdense mass at the left parasellar")
 • MRI brain: A contrast enhanced solid tumor , measuring 4. 6")
 • MRI brain ( cont’d) Laterally the mass was compressing left temporal")
 • Ophthalmologist consulted : Formal perimetry revealed no visual defect.")
 • What is the next investigation ?")
 • Prolactin : 154350 miu/L therefore, working diagnosis of macroprolactinoma made.")

 • Hyperprolactinemia caused by lesion of hypothalamus or pituitary stalk is due")
 • At times, no apparent cause is found for hyperprolactinemia, i. e.")
 • Etiologies of hyperprolactinemia Hypothalamic: craniopharyngioma, LCH, pituitary stalk lesion, other tumors")
 • Evaluation History , physical exam, screening blood test, thyroid function test")
 • Pituitary adenomas contribute <3% of supratentorial tumors in children, and 2.")
 • Microprolactinoma is usually confined to sella turcica. • Macroprolactinoma can be")
 • Prolactinoma can exert effect by: 1. Effect of excessive hormonal production.")
 2. Pressure effect: eg visual field disturbance, headache, cranial nerve palsy, hydrocephalus")
 • In one large series with detailed description of 26 patients under")
 4. For girls: all presented with menstrual disturbance ie primary amenorrhea, secondary")
 1. Observation with careful follow-up ( only for microprolactinoma) 2. Drug 3.")
 • For microprolactinomas, more than 90% do not enlarge over 4 -6")
 • Macroprolactinomas have already indicated a propensity for growth & virtually all")
 • Microprolactinoma: Most suggest drug therapy as about 80 -90% will have")
 • Microprolactinoma: For transphenoidal surgery, about 75% of patients had normalisation of")
 • Macroprolactinoma: Primary treatment is drug which is effective in normalising prolactin level")
 • In general, surgery in indicated for dopamineresistant prolactinomas, poor tolerance to long")
 • Bromocriptine is an ergot derivative that binds to & stimulate dopamine(D 2)")
 • With longer duration of treatment, stopping bromocriptine may not result in a")
 Analysis of 112 patients with macroprolactinomas revealed that >50% reduction in size:")
 • Reduction in tumor size often accompanied by visual filed improvement and")
 • The best approach is to reduce the dose gradually over several")
 • Common side effects are nausea and vomiting. • Can be minimised")
 • The incidence of abortions, ectopic pregnancies or congenital malformations is no")



 Height 138.")




- Slides: 51
Patients with Hyperprolactinemia Dr WONG Lap Ming 21 -9 -06
Patient 1
History (1) • Female, 14 year old • Referred from Student Health Service for premature adrenarche & delayed thelarche • F 2 student with average school performance • Onset of pubarche since 12 year old, with gradual increase in length, number and area of distribution of pubic hair • Axillary hair development since 12. 5 year old
History (2) • Slight breast development only in the past, but cannot recall exact event • No acne, no growth of beard • No deepening of voice, no prominent ‘Adam apple’ • No regular drug or herbs • On & off frontal headache for 2 years with several attacks per month. Each episode lasted for 1 -2 hours & mainly in afternoon, occasionally required paracetamol for relief. Not associated with nausea, dizziness or headache.
Past Health • G 1 P 1, Full term, normal spontaneous delivery, birth weight 2. 8 kg • Fever on Day 2 of life. Full sepsis work-up, including lumbar puncture were performed with all result unremarkable. • Several hospital admissions for pneumonia but recovered fully after treatment • No regular medical follow-up now.
Family History • Maternal uncle died at neonatal period of unknown cause • No family history of ambiguous genitalia or female infertility • Father height 168 cm. Mother height 155. 9 cm
Physical Exam • Body weight 42. 6 kg ( 25 -50%) • Height 146 cm (3 -10%) • Neurological system: muscle tone & power normal. No cerebellar sign. • Visual field: normal by confrontation test • Fundi-no papilloedema. • Chest, cardiovascular, abdomen: normal • Pubertal stage: B 1 P 3 A 1 Mo, many curled pubic hairs on both labia majora.
Investigation (1) • • • Full blood count: normal ESR: 19 mm/1 st hour Renal/Liver function Ca. Po: normal Anti-nuclear factor: negative Morning cortisol: 323 nmol/L Estradiol: 67 pmol/L Testosterone: 1. 29 nmol/L a feto-protein: 1. 7 ng/ml ( ref <6. 0) B-HCG: <0. 6 iu/L ( ref <5. 3)
Investigation (2) • Morning 17 -OH progesterone: 0. 7 nmol/L ( ref 0. 64. 0) • X-ray left hand: RUS score 650 ie bone age of 12. 7 yr at chronological age of 14. 0 • Luteinising hormone-releasing hormone stimulation test: Time( min) 0 20 60 FSH(iu/L) 3. 9 7. 3 8. 7 LH(iu/L) 0. 1 13. 1 11. 8
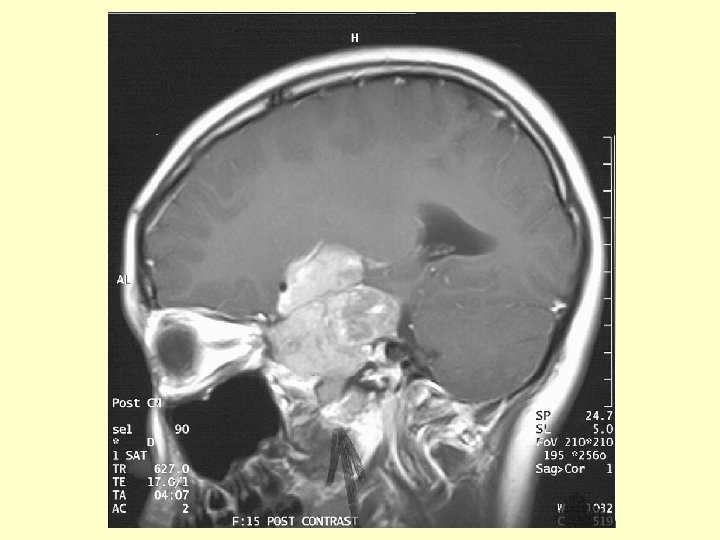
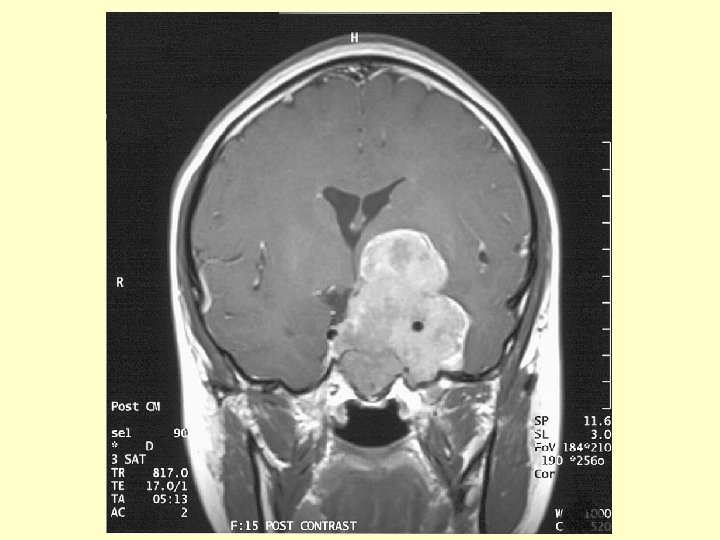
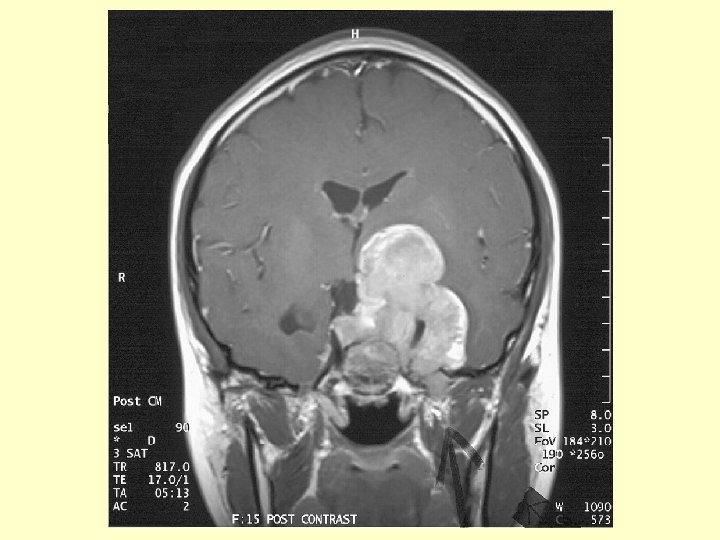
Investigation (3) • CT scan brain: A large hyperdense mass at the left parasellar region. It measured 4. 6 x 4. 4 cm. No calcification or cystic component found. It was extra-axial in location & extended into the pituitary fossa, middle & posterior cranial fossae. The left carotid artery was encased. The optic chiasm was compressed. There was mild hydrocephalus noted due to compression at level of Foramen of Monro.
Investigation (4) • MRI brain: A contrast enhanced solid tumor , measuring 4. 6 x 4. 8 x 6. 3 cm , was occupying whole sella with superior & inferior extension. Superiorly it extended to suprasellar cistern compressing left hypothalamus with the left cerebral peduncle being compressed & elevated. The frontal horn of left lateral ventricle was compressed from below. The left carotid artery was encased by tumor. The optic chiasm could not be identified but was likely to be compressed & encased.
Investigation (5) • MRI brain ( cont’d) Laterally the mass was compressing left temporal lobe & was occupying cavernous sinuses & Meckel’s cave. The mass also occupied right cavernous sinus & encasing right carotid artery. Inferiorly, the mass eroded through sellar floor & occupied sphenoid sinus with floor of sphenoid sinus preserved. Posteriorly the mass extended into left cerebellopontine angle cistern and caused compression of left of pons. Fourth ventricle not distorted.
Investigation (6) • Ophthalmologist consulted : Formal perimetry revealed no visual defect.
Investigation (6) • What is the next investigation ?
Investigation (7) • Prolactin : 154350 miu/L therefore, working diagnosis of macroprolactinoma made.
Treatment • Bromocriptine 2. 5 mg nocte with food started. • Initially with mild nausea, but subsided few days later, dose then increased to 2. 5 mg BD • Patient’s condition stable with no CSF rhinorrhea or visual filed impairment. • Prolactin level 3300 miu/L one week after treatment and was normalised 3 months later.
Discussion (1) • Hyperprolactinemia caused by lesion of hypothalamus or pituitary stalk is due to disinhibition of the tonic Prolactin-inhibiting factor ( dopamine) acting at the level of lactotrophs. • Level for such lesion is almost always < 3000 miu/L • Treatment for such lesion usually requires surgery • When prolactin level is >4000 miu/L, the chance of finding a prolactinoma by CNS imaging is high
Discussion (2) • At times, no apparent cause is found for hyperprolactinemia, i. e. idiopathic. • Such cases might be due to small prolatcinomas that is too small to be detected by current radiological techniques or presumed hypothalamic dysfunction. • Over 2 -6 years follow-up, only about 10% developed evidence of microadenomas and none developed macroadenomas.
Discussion (3) • Etiologies of hyperprolactinemia Hypothalamic: craniopharyngioma, LCH, pituitary stalk lesion, other tumors Pituitary disease: prolactinoma, acromegaly Drugs: neuroleptics, methyldopa etc Neurogenic: chest wall lesion, breast stimulation, Others: pregnancy, hypothyroidism, chronic renal failure, ectopic prolactin production Idiopathic
Discussion (4) • Evaluation History , physical exam, screening blood test, thyroid function test & pregnancy test will virtually exclude all causes except for hypothalamic-pituitary disease.
Discussion (5) • Pituitary adenomas contribute <3% of supratentorial tumors in children, and 2. 3 -6% of all intracranial tumors. • The average annual incidence of pituitary adenomas in children has been estimated to be 0. 1 per million children. • According to tumor size, prolactinoma can be divided into microprolactinoma when < 10 mm or macroprolactinoma when >10 mm in greatest diameter respectively
Discussion (6) • Microprolactinoma is usually confined to sella turcica. • Macroprolactinoma can be totally intrasellar, but is usually extrasellar, extending inferiorly to the sphenoid sinus but more often superiorly to the suprasellar space owing to lower resistance. During the process of extension, optic chiasm may be compressed or the cavernous sinuses can be involved.
Discussion (7) • Prolactinoma can exert effect by: 1. Effect of excessive hormonal production. In female, primary or secondary amenorrhea, galactorrhea, menstrual disturbance can occur. In male, gynecomastia, galactorrhea, decreased libido or impotence can occur.
Discussion (8) 2. Pressure effect: eg visual field disturbance, headache, cranial nerve palsy, hydrocephalus etc, notably in macroprolactinoma 3. Other pituitary hormone insufficiency: more common in macroprolactinoma e. g growth hormone deficiency, hypogonadism
Discussion (9) • In one large series with detailed description of 26 patients under 18 of age at diagnosis, several importance observation made. 1. All except one boy ( at 7 yr old) were >10 yr old 2. Macroprolactinoma & microprolactinoma were in 15 & 11 patients respectively. 3. For boys , 8 out of 9 had macroprolactinomas. The one with microprolactinoma presented with galactorrhea while others presented with headache or visual field defect.
Discussion (10) 4. For girls: all presented with menstrual disturbance ie primary amenorrhea, secondary amenorrhea or oligomenorrhea. All girls with headache were found to have macroprolactinomas. 5. Overall, pituitary hormone insufficiency at presentation were found in 2 out of 26 patients. 6. For microprolactinomas, serum prolactin ranged from 1400 to 10, 000 miu/L, with median of 2100 miu/L. For macroprolactinomas, serum prolactin ranged from 2900 to 66, 000 miu/L, median at 14400 miu/L
Treatment (1) 1. Observation with careful follow-up ( only for microprolactinoma) 2. Drug 3. Surgery 4. Irradiation
Treatment (2) • For microprolactinomas, more than 90% do not enlarge over 4 -6 years period with only 7 % will grow into macroprolactinomas. • It is unlikely for a prolactinoma to grow significantly with no increase in serum prolactin level. Therefore , most patients with microprolactinomas can just be followed with serial prolactin levels and only one or two repeat scan is indicated.
Treatment (3) • Macroprolactinomas have already indicated a propensity for growth & virtually all should be treated. Local or diffuse invasion or compression of adjacent structure, such as the stalk or optic chiasm, are additional indication for therapy. • Other indication for treatment are relative e. g. menstrual disturbance, premature osteoporosis, infertility, sexual dysfunction, galactorrhea.
Treatment (4) • Microprolactinoma: Most suggest drug therapy as about 80 -90% will have normalisation of serum prolactin level over several weeks & regression of tumor in about 70% within 3 -6 months. No consensus for duration of drug treatment. In general, 2 to 6 years of continuous treatment are recommended before considering tapering off treatment.
Treatment (5) • Microprolactinoma: For transphenoidal surgery, about 75% of patients had normalisation of serum prolactin level, followed by clinical improvement few weeks later, with recurrence rate about 20% at 10 years later.
Treatment(6) • Macroprolactinoma: Primary treatment is drug which is effective in normalising prolactin level in about 85% & reduce tumor size in 70%. Also no consensus for duration of treatment but at least 4 -6 years of therapy is recommended. Surgery is indicated for failed drug therapy after 3 -4 months of treatment or compression on optic chiasm. Normalisation of prolactin level can be achieved in up to 60 -70% for intra-sellar macroprolactinomas. However, recurrence rate of 20 -50% are likely over 10 years.
Treatment(7) • In general, surgery in indicated for dopamineresistant prolactinomas, poor tolerance to long term dopaminergic treatment or rare complication to drug therapy eg CSF rhinorrhea. • Radiation therapy is indicated for failed drug or surgical treatment.
Bromocriptine(1) • Bromocriptine is an ergot derivative that binds to & stimulate dopamine(D 2) receptors on normal & adenomatous lactotroph cells. • Single dose study showed that serum level peaked at 3 hours with undetectable level 11 -14 hours later. • Bromocriptine decrease prolactin synthesis, cell multiplication & tumor growth. • When bromocriptine is stopped for 1 week after 2 weeks of therapy, there is rapid re-growth of tumor cells.
Bromocriptine(2) • With longer duration of treatment, stopping bromocriptine may not result in a reversal of cell atrophy & tumor re-growth does not always occur. • Bromocriptine results in normal prolactin level or return of ovulatory cycles in 80 -90% of patients.
Bromocriptine (3) Analysis of 112 patients with macroprolactinomas revealed that >50% reduction in size: 40. 2% 25 -50% reduction in size: 28. 6% <25% reduction in size: 12. 5% no reduction: 18. 7% Time course of regression is variable. Some patients had improvement in visual filed in 24 -72 hours with significant change on scan in 2 weeks. Others started to have clinical improvement in 6 weeks.
Bromocriptine (4) • Reduction in tumor size often accompanied by visual filed improvement and restoration of other pituitary hormonal axes. • After prolonged therapy of 3 -4 years, bromocriptine withdrawal results in resumption of hyperprolactinemia in about 80 -90% of patients but tumor growth in 10 -20%. • In patients with very large tumor having excellent tumor regression, stopping therapy must be done very carefully, if at all.
Bromocriptine (5) • The best approach is to reduce the dose gradually over several months, following prolactin level, and only discontinue the drug if no more increase in prolactin level or tumor size while on just 2. 5 mg or less per day. • Overall, about 20% of patients can stop bromocriptine and maintain normal prolactin level.
Bromocriptine (6) • Common side effects are nausea and vomiting. • Can be minimised by starting with 1. 25 mg daily with snack at bedtime. Then gradually increase to 2. 5 mg BD with meals over 7 -10 days and prolactin level checked after 1 -2 months. • Most patients respond within 1 -2 months if they are going to respond. • Dose higher than 7. 5 mg per day are usually not necessary except for very large tumor.
Bromocriptine (7) • The incidence of abortions, ectopic pregnancies or congenital malformations is no higher in infants born to mothers who conceived while taking bromocriptine than that in the general population. • However, it is best to limit the exposure of the embryo to such drugs as much as possible. • It is recommended that bromocriptine be stopped once the first menstrual period has been missed and a positive pregnancy test is obtained.
Suggested reading • Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. FF Casanueva et al. Clinical Endocrinology; 2006; 65: 265 -273. • Advances in the Treatment of Prolactinomas MP Gillam et al Endocrine Review 2006; 27: 485 -534
Patient 2
History • Presented at 9. 0 years old for pubic hair development since 8. 1 years old. • No breast development, no axillary hair • Growth spurt since 8. 5 years old • No headache, no visual field problem • No regular drugs or herbs • No family history of neonatal death
Physical examination • • • Body weight 29 kg ( 50 -75%) Height 138. 4 cm ( 75 -90%) Pubertal stage: B 1 P 2 A 1 Mo External genitalia: no clitoromegaly No hirsutism Visual field: normal by confrontation test Fundi: normal Other systems: normal BP 104/62 mm. Hg
Investigation • • TSH 1. 66 miu/L, f. T 4 13. 5 pmol/L Estradiol <37 pmol/L Testosterone 0. 34 nmol/L a-feto protein 1. 8 ng/ml B-HCG <2. 0 iu/L Basal FSH 4. 3 IU/L basal LH 0. 4 IU/L Cortisol 530 nmol/L Morning 17 -OHprogesterone 9. 4 nmol/L ( ref 0. 314. 4) • Prolactin 1022 miu/L
Investigation • MRI brain including hypothalamo-pituitary region: normal ( at 9. 4 years old and at 10. 7 years old)
Progress • Breast development since 9. 4 years old • No symptoms all along • Serial prolactin level showed persistent increase.
Serial prolactin level • Age 9. 0 9. 1 10. 6 10. 7 11. 1 Prolactin 1022 1333 1558 3125 3248 3016 • Age 11. 4 Prolactin 2679 11. 7 12. 3 204 300 At 11. 7 years old, laboratory applied precipitation for macroprolactin & result corrected.