Patient Positioning Rachel BrightThomas Consultant Surgeon WAHNHST r

Patient Positioning Rachel Bright-Thomas Consultant Surgeon WAHNHST r. bright-thomas@nhs. net

To cover the curriculum topics Peri-operative Care • To assess & manage pre-operative risk • To prepare patient for theatre • To conduct safe surgery in the operating theatre environment Intra-operative Care • To know the principles of positioning & pressure area care • To have technical skills to be able to safely position a patient on the operating table • General Principles Aims Specific Positions Documentation
 Provide physiologic")
Provides optimal exposure of the surgical site Airway management and ventilation (FRC) Provide physiologic safety (BP) Maintenance of the patient’s temperature and dignity by controlling unnecessary exposure. Maintain body alignment & prevent nerve, vessel & soft tissue injury Minimise risk VTE The Importance of Proper Positioning

Patient Transfer from Bed to Operating Table • HAVE A PLAN • Always under the leadership of 1 person (anaesthetist) with correct no. of TRAINED staff (? ? ? ) • Generally best to anaesthetise the pt first • Need brakes on, moving aids ready, and table attachments to hand • Pt is supported in all areas • All monitoring equipment is safeguarded • Pressure care is given • VTE prophylaxis • Temp & Dignity is maintained

Patient Transfer from Bed to Operating Table Avoid Friction burns when moving, Avoid Pressure on soft tissues, vessels & nerves and ears with appropriate padding Avoid Contact with metal Avoid Leaning on patient Protect Note Eyes from extra-ocular pressure and close lids to prevent corneal abrasions Pt position relative to table “breaks” Consider Any physical abnormalities & avoid hyperextension of joints Consider Pt tolerance to position (including length of op & type of anaesthesia)

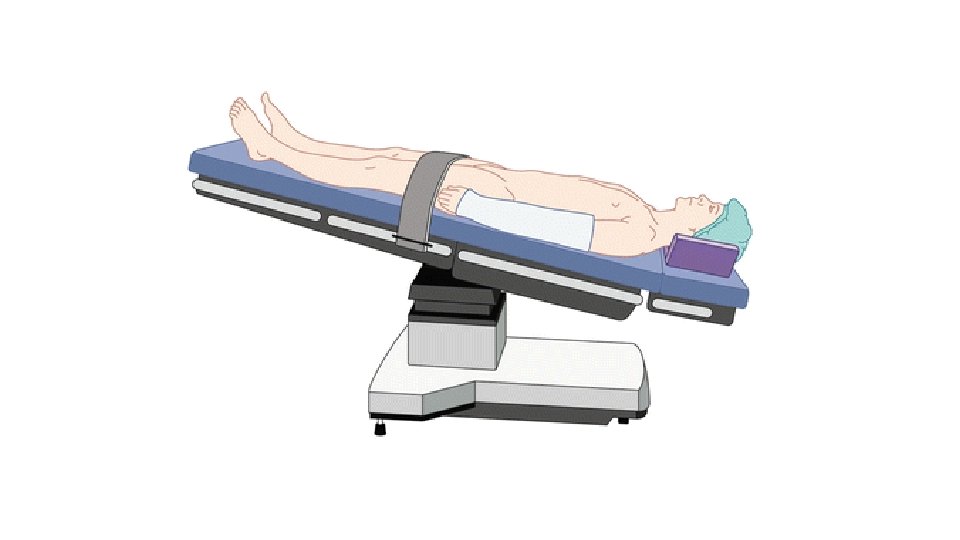
• Hips & spine aligned, legs parallel & ankles uncrossed. • Head in a neutral position ? ? why? ? ? • Arm boards at <90 degrees ? ? ? Why? ? ? • Pressure relief required for occiput, sacrum, ankles, heels & elbows Issues: • Reduces ventilation by ↓FRC • Most common neuropathy ? ? ? Supine- For Majority of Procedures

Specific Problems • Pregnant Patient • Leg Traction • Counter traction provided by a perineal post. • Must be well broad & well padded & rest against the pubic ramus • It should not press against the external genitalia, ischium or the pudendal nerve
 • Ideal for some abdominal, laparoscopic &")
Trendelenburg (Head down- approx. ? ? o) • Ideal for some abdominal, laparoscopic & gynaecological surgery. • Can allow better access to organs located in the pelvis or for hernia repair. • May be useful in hypotension • Issues- ↑intracranial pressure; risk of vomiting; restriction of lung movements due to pressure on diaphragm, facial and eye swelling • Need a secure non-slip mattress

 1 2 Useful for H&N surgery (?")
Reverse Trendelenburg (Head Up 15 -20 o) 1 2 Useful for H&N surgery (? less bleeding) + Upper GI surgery In obese patients Good laryngeal exposure ↑pulmonary compliance 3 Pt must be well secured and normovolaemic

Supine position with legs separated, flexed and supported in raised stirrups.

Lithotomy Issues/Risks- esp with prolonged surgery > 2 hrs Note time of surgery starting Compartment Syndrome Nerve injury consider resting legs for 10 mins every 2 hrs Note any suggestive signs and Sx post operatively Obstruction to venous drainage- need DVT prophylaxis Increased central venous return on leg elevation & hypotension when put back down
")
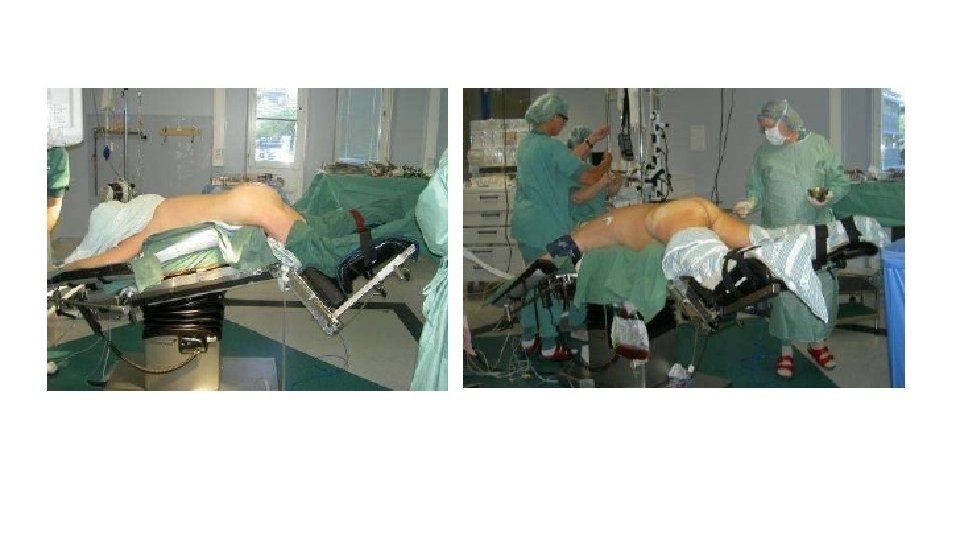
Lloyd Davies Position (? ? Head Down Lithotomy Or Legs Apart Trendelenburg? ? ) • For pelvic and rectal surgery where access is required from both abdominal and perineal aspects ie anterior resection; laparoscopic surgery • Key difference from lithotomy is lesser degree of hip & knee flexion- allows longer surgery • Position legs first and then tilt • The patient’s hands should be padded and tucked in to avoid table attachments • Risks- as for Lithotomy & Trendelenburg

Prone • Intracranial & spinal surgery; achilles tendon repair • General Issues • Airway difficult to access • needs to be secured without damaging face • Recheck tube after turn • Keep anaesthetised until turned back over • Keep head neutral (nerve & vessel injury) • Variable effects on ventilation (so avoid abdominal compression) • Venous access difficult (avoid antecubital fossa) • Many pressure points Staffing needed to roll Pt? ? ? CPR difficult

Lateral Position • For thoracic, hip & shoulder surgery • Issues • Airway • V/Q mismatch → hypoxia • BP cuff ideally on upper arm • Nerve injuries ? ? • Lower ear

Sitting/ Beach Chair • Shoulder surgery; breast reconstruction; intracranial surgery • Issues • Access to airway (secure well) • Hypotension ( sit slowly; keep filled) • Monitor BP (keep MAP >70 mm. Hg) on non-operated arm • Complications • Cerebral ischaemia • Venous air embolism • Excessive neck flexion-quadriplegia

Preop • Discuss patient’s positioning & specific requirements at team briefing • Operating table & equipment checked for function, size & cleanliness Information to be recorded in the patient’s notes Position Pressure relieving padding used VTE equipment used Skin integrity before and after the procedure Names and designation of staff members positioning the patient Documentation

• Table height • Sitting vs standing • Lighting • Assistants Surgeons Position

Any Questions?
- Slides: 21