Patient Monitoring Chronic HIV Care and ART Sandy












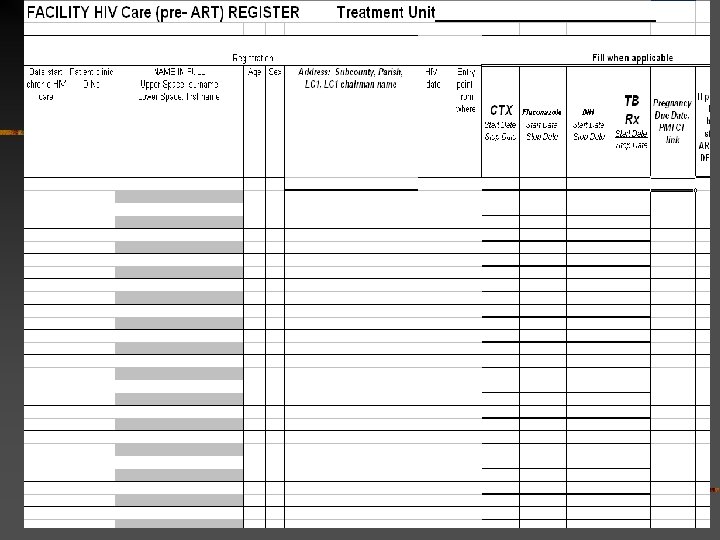
 Chronic HIV Care Pre. ART When registered for HIV care Date")
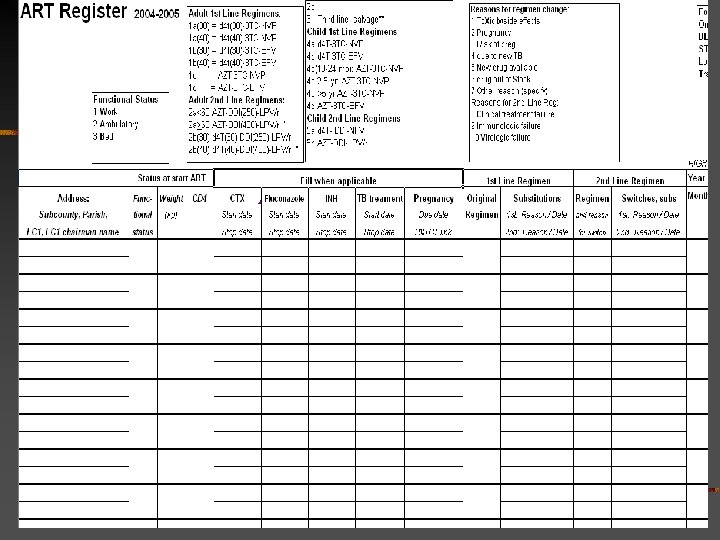
 ART Register (incl. post-ART) n n n Cohorts formed in ART")
 Substitutions within first line and")






















- Slides: 41
Patient Monitoring: Chronic HIV Care and ART Sandy Gove WHO HIV Department
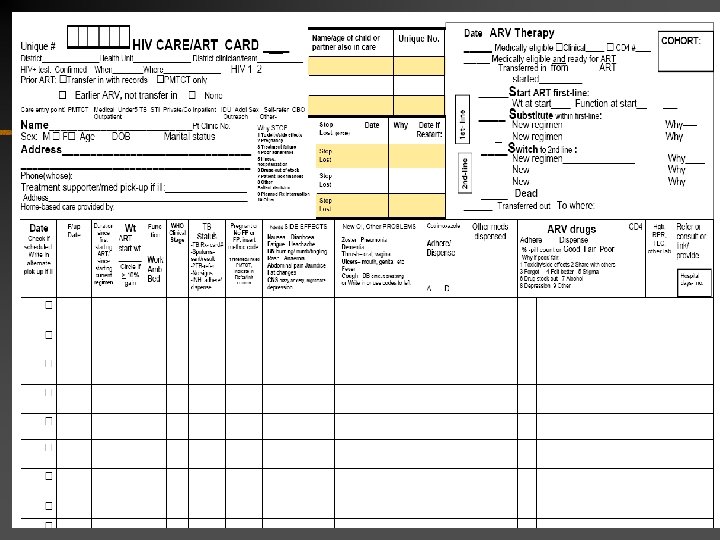
HIV Care/ART Card is on the last 2 pages of this module Patient monitoring needs to be integrated within comprehensive HIV care and ART!
Patient monitoring guidelines are based on: n n n Standardized core and other data elements- agreed by WHO, CDC, USAID, PEPFAR, multiple NGOS attending a WHO Patient Monitoring meeting in March 2004 Collecting and analyzing only what is needed for patient management and for clinic, district and national management Allowing flexibility for additional data collection and analysis However: n n n Clear distinction is made between what is essential and what should be reserved for extra operational research or data summaries. If data collection is not simple, it can be a barrier to scaling-up ART. MORE IS NOT BETTER!
TB experience… TB n n n n Standardized treatment card Standardized register Globally standardized definitions Deliberately constrains data collected Based on long experience Recently, new TB-HIV indicators Disease-specific (vertical) ART/ chronic HIV caren Builds on TB experience but with key alterations n Also requires a simplified disease-specific system n n Can pave the way or fit with similar methods for diabetes, other 'true' chronic illnesses Paper base is important for feasibility
New in HIV care and not yet eligible for ART A New in HIV care and eligible for ART C Non-naïve patients to ART who are not Transfer In with records Enrolled in HIV care and not yet eligible for ART B (Total = new + continuing) Enrolled in HIV care and eligible for ART D (Total = new + continuingincludes those who decline ART) Died in pre. ART care Lost Transferred out Enrolled in HIV care and eligible and ready for ART E New on ART this month G Total ever started on ART in this facility F
New on ART this month G TI = Transfer In with records Add to cohort according to ART start date Start or continue on original first-line ARV regimen H Substituted to alternative first-line ARV regimen I Switched to second-line (or higher) ARV regimen J DEAD after starting ART TO = Transfer out LOST STOPped ART (some Restart)
HW fills out HIV care/ART card. If switch to second line, substitutions, stop, etc. —> MO decides, Card defines consults, log book, clinician coding listminimal data to be collected. record on card HW codes are on the card Pre-ART register Monthly ART register Cohort analyses at 6, 12 months then yearly— Calculate indicators for clinic use only ▪ Calculate agreed district, national, international indicators ▪ Monthly (cross-sectional) report Input to monthly drug orders if required District Regional team to MOH to AFRO, HQ, agencies
Patient monitoring system n Paper system is based on 6 items: n n A patient-held card A facility-held chronic care card n n n n HIV Care/ART Card or Same data elements in another format HIV Care pre-ART register ART Register Monthly report (updated from Cohort analysis report Format of the card can be changed. Standardized variables and codes are what is important. This can serve multiple needs: n n n Direct patient care (facilitates paradigm shift from Acute to Chronic Care) Drug supply monitoring and preparation of facility drug orders Data summarized and reported to meet district and national programme needs and track progress to targets (3 x 5; 2, 7, 10; etc)
HIV care/ART card- adapt in country during IMAI adaptation n Agreement is being finalized on the standardized data elements n n n Definitions Coding Freedom to: n n n Use different formats including full patient chart Collect additional data Country adaptation, as clinical guidelines are adapted n n If no INH prophylaxis for HIV patients, no column on card Etc
HIV Care/ART Card adaptation n Most important to standardize system nationally with allowances for collecting more data/different formats for patient cards or charts: n Number pages per patient- visit n n Wide range from. 05 (multiple visits on single card; extract key data) to 8 pages Card versus multiple page chart
Substantial variation in data retained on card/chart Simplest, limit paper: n n Clinical review assisted by laminated form Record key treatment data and pertinent positives Other details may be in patient-held exercise book or 'patient passport' Example: IMAI; Malawi More elaborate: n n n All positives and negatives of clinical review recorded Detailed treatment data Requires full chart What is really needed?
HIV Care/ART Card backside in IMAI: patient education and support n Education: n n n Adherence n n Support n n HIV basics, disease progression Treatments available n Psychosocial Disclosure Family Prevention n n Preparation Decide when readyresults clinical team meeting Support Problem solving
2 registers: (1) Chronic HIV Care Pre. ART When registered for HIV care Date HIV+ Entry point Start/stop dates prophylaxis- CTX, fluconazole Pregnancy, TB **When medically eligible for ART **When medically eligible and ready for ART (prepared for adherence, clinical team has met) **When ART started plus unique patient identifier Dead before ART Lost or Transfer out before ART
2 registers: (2) ART Register (incl. post-ART) n n n Cohorts formed in ART register (not Pre. ART register)– by month Date ART started, unique identity number Why eligible 1=clinical only 2=CD 4 3=TLC At start ART: function, weight, (CD 4) Same as Pre. ART register (transfer) n n Start/stop dates prophylaxis- CTX, fluconazole Pregnancy, TB
ART register- continued n n n Original regimen (coded) Substitutions within first line and switches to second line-- reason (code) and date Months 0 to 24: n n n Each month: current regimen (coded) At 6, 12 months: function, weight gain > 10%, (CD 4) Then each year: function, (CD 4)
Why STOP ART- reason codes 1 Toxicity/ side effects 2 Pregnancy- planned treatment interruption 3 Treatment Failure 4 Poor Adherence 5 Illness, Hospitalization 6 Drug out of Stock 7 patient lacked financial Resources 8 other patient Decision 9 planned treatment Interruption (put reason 10 Other )
Why change ARV drug or regimen 1 Toxicity/ side effects 2 Pregnancy 3 Risk of pregnancy 4 due to new TB 5 New drug available 6 Drug out of Stock 7 0 ther reason (specify)_______ Reasons for switch to 2 nd-Line Regimen only: 8 Clinical treatment failure 9 Immunologic failure 10 Virologic failure
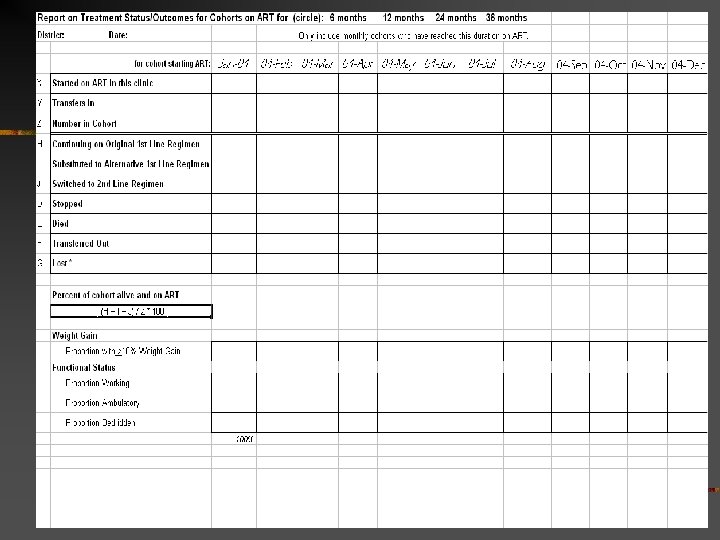
2 registers 2 reports Monthly report: n New and cumulative ever: Enrolled in HIV care n Started on ART at this facility Disaggregated by sex, pregnancy, age n n n Transfer in (already on ART) Restart ART Patients eligible for ART but not started ARV regimens- number on n Each regimen n First-line n Second-line Lost, Dead, Stopped, Transfer out Cohort data for last month: Median CD 4: baseline, 6 and 12 mo on ART Picked up ARVs 5/6 or 10+/12 months n Cohort analysis (quarterly or other periodicity) n Patient status: n n n n Alive- on or off ART, regimen Dead Lost Transferred out Functional status Proportion with > 10% weight gain Proportion with CD 4>200
Cohort analysis: 6 mo, 12 mo, yearly n Proportion of patients on ART with weight gain > 10% (6, 12 mo) Proportion working, ambulatory, bedridden n Proportion alive and on ART at 6, 12 months then yearly n Proportion still on a first-line regimen Proportion still on original first-line regimen Proportion who have substituted to an alternative first-line regimen Proportion switched to a second-line (or higher) regimen n n n Proportion of CD 4 counts done which are >200 (optional) Proportion of viral loads which are below 400 copies/ml (optional)
Treatment Centre at District Hospital/HC IV Register at Health centre Clinical team Nursing assistant, lay providers CO, RN Consult, refer, back-refer, visit MO, MD RN, CO, medical RN aid Clinical team Visits by district or regional ART team/coordinator. Help with registers, reports, cohort analysis Nursing assistant, lay providers
Malawi cohort and 'cumulative' analyses Cumulative- Total registered on ART since start Cohort- Number registered in that quarter n Alive and on ART n n n n On original first-line regimen (Start) On alternative first-line (Substituted) On second-line regimen (Switched) Stopped Defaulted– ? call 'Lost' to distinguish from TB Transferred out Of those alive: ambulatory, at work, side effects, drug adherence >95%
Malawi- logistics in managing many patients on ART n n Hanging files- cards are stored sequentially Patient held cards with number and date starting ART
Matching electronic version Designed so it can enter at various steps and be interchangeable with paper n Paper card- electronic generate register n Paper card to paper register electronic entry n Paper card to paper register to monthly report, cohort reports send or call by mobile phone computer entry n Computer generated paper register n n For 2006 -2007 For use in facilities without electronics For back-up when computer doesn't work Compatible Palm entry (Satellife project)
Computer system centrally needed by all: n n For monthly and cohort report data To handle Transfer In and Transfer Out patients n Needs to link with drug supply
Country adaptation of the card, register, report forms n n Do at the same time as the adaptation of the clinical guidelines In Ethiopia, added 7 hours to first 3 day adaptation workshop
HIV Care /ART Card, pre-ART and ART registers in Uganda n First pre-tested in Masaka region (4 districts), Uganda when training 70 health workers in February 2004. n Registers introduced during post-training on-site visits in March and April 2004 n n Many health workers had made up their own registers. Used in Hoima Region (4 districts) Uganda with pretest of training materials to support use of the registers
HIV Care /ART Card in Uganda n n Variables in the card and registers (TB status, clinical stage, prophylaxis, FP status, ART eligibility /regimen, etc) are embedded in the 4. 5 day Basic ART clinical training course. Health workers learn the clinical care process and how to fill out the card at the same time, with exercises and practice.
HIV Care /ART Card, pre-ART and ART registers training n As part of the 4. 5 day Basic ART Clinical Course workshop n As 4 hour additional training for those who will do patient tracking and monitoring in the health facility n Training "refreshed" during on site posttraining visits: individual training
HIV Care /ART Card, pre-ART and ART registers in Masaka n Used in 18 facilities (1 Regional Hospital AIDS Clinic, 1 ART Clinic -600 patients, 4 District Hospital AIDS Clinics, 12 HC IV and III) n Slightly revised after first 4 weeks of use
HIV Care /ART Card, pre-ART and ART registers in Masaka Feedback during on-site visits after training (not quantitative due to the limited number of facilities and recent introduction): n HW: Useful tool providing streamlined information Easy to fill out the card while doing the clinical review- part of the same process Easy to transfer info into the register Easy to quickly perform clinical review on the basis of data collected during previous visits n Trainers: 45 minutes needed to "refresh" on how to fill out the card and show to use the register.
HIV Care /ART Card, pre-ART and ART registers in ART Clinic, Masaka n Progressively replacing a 4 page HIV Care /ART record as ART is scaled-up from 100 to 600 patients Feedback from health workers: n HW: Useful tool providing streamlined information n n Around 20 minutes per patient are saved since using this card They like "everything on one page" – demographic, clinical and ART data
Where electronics might enter: n n District outpatient, health centre III/IV: paper card Agreed data into paper register; monthly reports, clinical team uses date n Mobile phone n n n District or regional team enters register data into computer cohort analyses, indicators Enter agreed data into palm or computergenerate monthly reports Computer generation of cohort analyses and indicators
Number and percent of people with advanced HIV infection receiving ART In clinics with ART services, a more specific indicator: Numerator: Patients on ART Denominator: Patients medically eligible and ready for ART These patients have all accessed services. UNGASS indicator based on total patients receiving ART Denominator: estimated patients with AIDS (15% those infected)
Monthly analyses possible without a register or electronics n % patients with good adherence n Review reasons for fair or poor adherence Patients with special problems n % patients referred n Identify patients for review at clinical team meetings n Patient monitoring as tool for quality improvement Card sorts, stickers, flags Motivation, needs to be satisfying and possibly fun n
Training materials n n n Training to fill out HIV Care/ART Card integrated within WHO Basic ART Clinical Training course Module on how to fill out registers, do card sorts, monthly reports, use data- for health worker or 'professional' lay provider or HW Module on supervising and summing monthly and cohort analysis reports (similar to TB district coordinator training module)– district coordinator
Current concerns n Importance of supporting card/register with training materials n n Timelinessn n Need rapid regional review and further pretesting Programmes are starting to treat patients Training is happening Staff are making up cards and registers in absence of simple standards Urgent need to address children n Draft card for further expert input
Further work & national adaptation needed to deal with: n Logistic and information system to handle Transfer in/Transfer out-- with records n n n Add retrospectively to cohort according to when started ART Will become an increasing proportion of patients over time, with return to work, normal mobility Restart after treatment interruption n When is restart permitted? Different circumstances-n n Goes back into the same patient record (line in the register) n n Deliberate treatment interruption in first trimester pregnancy Lost or very poor adherence- ? Restart Adjust if planned treatment interruptions later recommended Number, weeks of each treatment interruption retained on cardcould be used in special analyses Non-naïve patient on ART from other sources n Goes into HIV Care Pre. ART register (queue in rationed system)must qualify (determine that medically eligible) and be ready