Patient Empanelment HSAG Webinar July 18 2016 Kevin

Patient Empanelment HSAG Webinar July 18, 2016 Kevin Grumbach, MD Center for Excellence in Primary Care Department of Family & Community Medicine University of California, San Francisco 1

Webinar Objectives • To learn how to define a panel of active patients • To understand how to use empanelment to define numerators and denominators for measuring quality performance • To understand how to stratify a patient panel based on different level of care needs for targeting population health care management strategies • To learn how to use panel size estimates for planning PCP capacity to align with patient 2 demand
 to identify")
Background • Work of UCSF Center for Excellence in Primary Care (CEPC) to identify key attributes of high performing primary care practices 3

Group Health Olympia 23 high-performing practices Fairview Rosemont Clinic Multnomah County Health Dept Harvard Vanguard Medford Theda. Care Allina Mayo Red Center Medical Associates Clinic Ole Clinica Family Health Services Sebastopol Community Health La Clinica la Raza Univ of Utah. Redstone de Cleveland Clinic. Stonebridge Mercy Clinics Quincy, Office of the Future Newport News Family Practice West Los Angeles. VA South Central Foundation Source: Bodenheimer, T. , Ghorob, A. , Willard-Grace, R. , & Grumbach, K. (2014). The 10 building blocks of high-performing primary care. The Annals of Family Medicine, 12(2), 166 -171. 4

10 Building Blocks of High Performing Primary Care T Bodenheimer et al Ann. Fam. Med March 2014 • 5
 as their")
Definition of Empanelment • Patients having a specific primary care physician (PCP) as their regular source of care, such that – Patients are able to identify their “medical home” – The PCP knows who is at home, i. e. can identify and enumerate the patients that constitute his or her active “panel” of patients 6

Empanelment is an Enabler of Other Building Blocks T Bodenheimer et al Ann. Fam. Med March 2014 • 7

Why you should care about empanelment • Better for patient relationship and experience • To succeed in current health care environment – MACRA – MIPS – P 4 P – APMs – ACOs – PCMHs • To promote access and reduce burnout by understanding capacity relative to demand 8

The Mechanics of Empanelment • Formal – Explicit registration with PCP – Usually linked with capitation payment • Less formal – Estimated based on utilization patterns – Fee for service payment context 9

Formal Empanelment • Health plan requires patient to designate a specific PCP • Necessary when payer uses capitation for PCP payment – Uncommon in US • Some HMOs • “Direct Payment” model – More common in Europe 10

Less Structured In Fee For Service Payment Contexts • Rarely formal voluntary vows of mutual commitment • Using PCP field in EMR • Usually estimated based on encounter history – By PCP/practice (e. g. , patients with at least 1 visit in past 2 years) – By payer (e. g. , “attribution” models based on PCP with plurality of billed encounters) 11

Do You Know How Many Active Patients You Have in Your Practice? 12

Getting Started on Enumerating PCP Panel • If EMR, use PCP field • Define lookback period for measuring visit with PCP – Conventions range from 12 months to 36 months, typically 24 months – Decide if any type of visit counts • Does it need to include preventive care visit? • Does a virtual visit count? (telephone call, patient portal, Rx refill) 13

Keeping Panels Clean and Accurate Assign patients who are unassigned Remove patient from panel Run unassigned report

Assignment More Complicated in Larger Group Practices • • • Assigning PCP at or before 1 st visit Validating PCP (and ensuring assignment) at Check-In Identification of unassigned patients & assignment of PCP Transfers (external & internal) New patient assignment

Keeping Panels Clean and Accurate Assign patients who are unassigned Remove patient from panel Run unassigned report

Payer Attribution Model Source: Massachusetts Multi-Stakeholder Attribution Workgroup, Consensus Guideline for Commercial non-HMO Attribution Methodology, August 2015. As reported by Health Care Payment Learning and Action Network https: //hcp-lan. org/groups/pbp/pa-final-whitepaper/ 17

Questions on Mechanics? ? 18
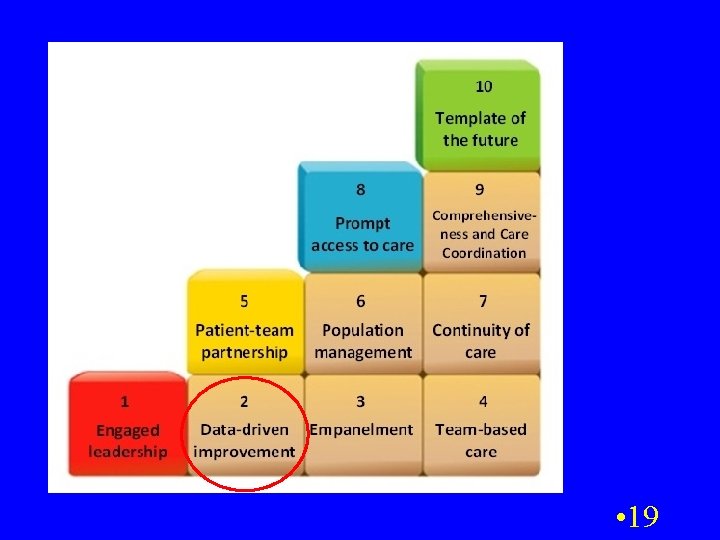

Putting Empanelment to Use: Data Driven Improvement • Era of denominator medicine – Not just reporting quality, safety, errors for individual cases (old M&M model) – Measuring rates of achievement for a defined population of patients • % with up-to-date cancer screening • % with Hgb. A 1 C and BP at target level • Denominators for particular measures are subset of total panel – E. g. , age 50 -75 for colon cancer screening 20

Active “Clean Up” of panel registry particularly important when using panel as denominator for quality performance reporting • Removing patients whom you know have left the practice • You do not want to be held accountable for performance on patients no longer under your care – Inflated denominator results in lower quality rates • You do want to actively outreach to close care gaps if still empanelled 21
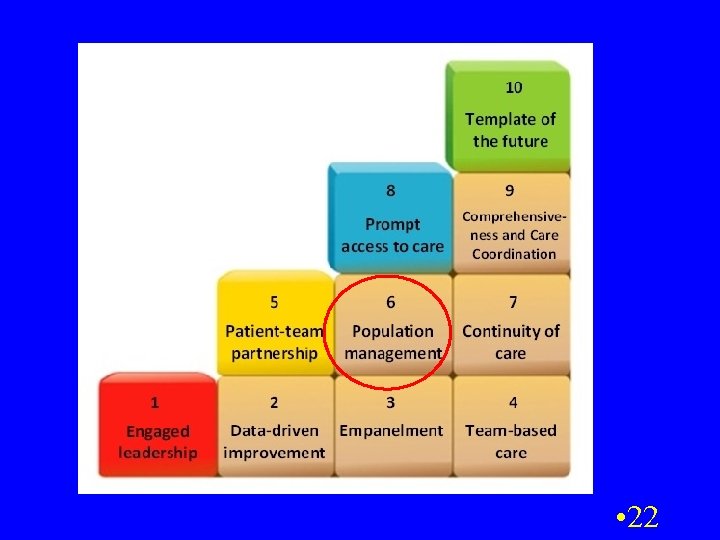

Putting Empanelment to Use: Population Management • Knowing your active patient panel and the different care needs of different strata within the panel 23
 40 -50% costs Chronic Conditions (40%) At")
Adult Population Risk Distribution Severe Problems (5%) 40 -50% costs Chronic Conditions (40%) At Risk for Poor Health (20%) Generally Healthy (35%) 24
")
Adult Population Risk Distribution Population Health Severe Strategies : Problems 1. Manage patients (5%) effectively and efficiently at each level Chronic Conditions 2. Keep patients from (40%) moving up the pyramid 3. Ensure a good At Risk for Poor Health medical home (20%) Generally Healthy (35%) 25

Tailor Care Model to Population Strata Health Coaches Panel Management Prompt Advice & Urgent Care Access Source: San Francisco Health Plan and UCSF Center for Excellence in Primary Care

Questions on Data Driven Improvement and Population Management ? 27
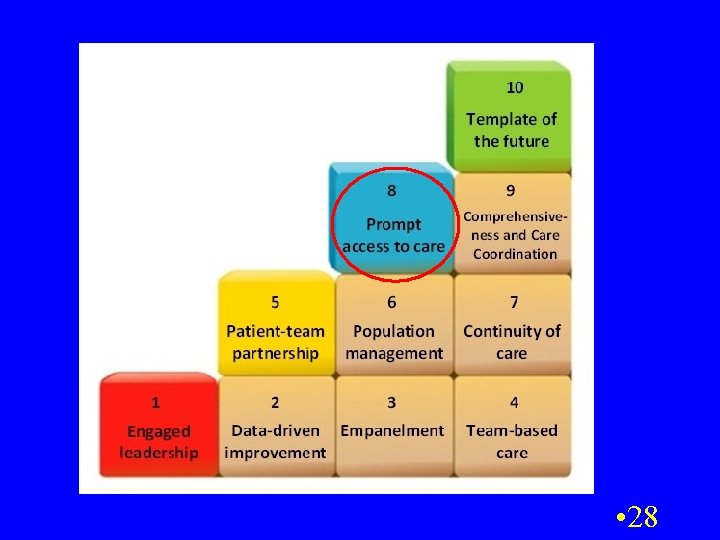

Putting Empanelment to Use: Access 29

Empanelment and Panel Size • Actual number of patients that “belong” to a team/PCP Panel Capacity • The # pts PCP/team can care for • Based on current FTE, productivity, and utilization

Managing Panel Size – Why Bother? • Panel size too large – Difficult to achieve adequate access, patient experience, and quality – Burned out PCPs • Panel size too small – Inefficient and financially challenged

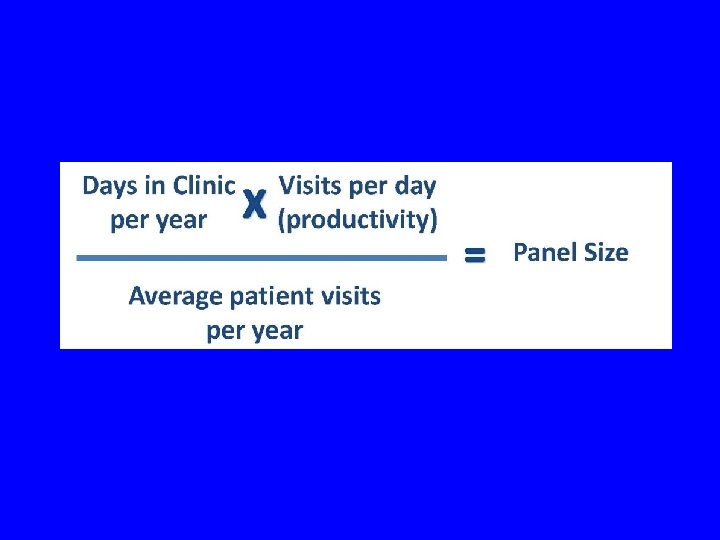
Visit Based Method for Comparing Supply and Demand B C D Solve for Supply = Demand
 B. Days in Clinic")
Example Calculate Panel Size Capacity (B x C / D) B. Days in Clinic per year 250 C. Avg Slots per day of patient care 20 D. Avg pt Panel Size visit per year Capacity (Return Rate) 1667 5000 3 Can then compare panel size capacity to actual active panel size to determine if PCP is over- or under-empanelled
:")
Adjustment for Specialty • For clinics with multiple specialty practices (IM, FP, Peds, etc): – The average patient visits per year will be different by specialty. Example from 1 practice: Specialty Avg. Pt. Visits/Yr Internal Medicine 4. 5 Family Practice 3. 5 Pediatrics 2. 8

But are visits the best metric for panel capacity estimates? • Growing amount of non-visit work effort for PCPs • Negotiated panel size targets based on “reasonable” panel size expectations • Adjusting targeted panel size for differences in patient complexity and required PCP work effort (panel weighting) 36

Questions on Panel Size Management? ? 37

Take Home Points • Empanelment is an essential building block for high performing primary care • Enables – Continuity of care – Data driven improvement and reporting – Population management – Access and balancing capacity and demand • First step is creating registry of active empanelled patients • Then active cleaning and maintaining panel 38 registry and applying it for practice improvement

References • Grumbach K, Olayiwola JN. Patient empanelment: the importance of understanding who is at home in the medical home. J Am Board Fam Med. 2015 Mar-Apr; 28(2): 170 -2. http: //www. jabfm. org/content/28/2/170. full • Murray M et al. Panel size: how many patients can one doctor manage? Fam Pract Manag. 2007 Apr; 14(4): 44 -51. http: //www. aafp. org/fpm/2007/0400/p 44. pdf • Safety Net Medical Home Empanelment Guide http: //www. safetynetmedicalhome. org/change-concepts/empanelment • Health Care Payment Learning and Action Network: Accelerating and Aligning Population-Based Payment Models: Patient Attribution https: //hcp-lan. org/groups/pbp/pa-final-whitepaper/ 39

kevin. grumbach@ucsf. edu http: //cepc. ucsf. edu/ 40
- Slides: 40