Pathophysiology of Hypertension and Endothelial Dysfunction in Patients







 Diabetics—increased metabolic processes that produce reactive oxygen species (ROS) n")


 n Adrenomedullin n Endothelium-derived hyperpolarizing factors n Prostacyclin (PGI")
 n Angiotensin II n")





 n n n Elevated TG, low HDL-c, and elevated IDL—insulin")
 n n n The extent of ROS formation-also be a")

 n")





 oxidase")















 n n n AGEs formed by the nonenzymatic binding")




 n n n There is compelling evidence for endothelial dysfunction in both")
 Reactive oxygen species, overproduced in diabetics, serve as signaling molecules that mediate")
- Slides: 65
Pathophysiology of Hypertension and Endothelial Dysfunction in Patients With Diabetes Mellitus January 24 th 2003 楊純宜醫師
Epidemiology in DM n n n n n >10 million Americans with diabetes 90 -95% of whom have type 2 diabetes 798, 000 new cases of diabetes diagnosed each year 5 million more cases are undiagnosed, untreated 13 million have impaired glucose tolerance All patients are at risk for associated metabolic disorders and micro- and macrovascular complications Annually, CV disease >77, 000 deaths in diabetes-related death The primary risk for a heart attack in type 2 diabetes is as high as in pts with ischemic heart disease Diabetes—”risk equivalent” for CV disease Associated risk factors (lipids) should be treated as aggressively in diabetes as in heart disease
Epidemiology of hypertension in DM Morbidity & mortality associated with DM— macrovascular & microvascular complications n The prevalence is greater in diabetics with hypertension n The prevalence of hypertension in DM pts is higher, especially in younger persons n 40% at age 45 years, and increases to 60% by age 75 years n
CV events and DM n n n Risk of CV fatal or nonfatal event or renal insufficiency ---is also greater in diabetics Diabetics are at increased risk for all CV events including stroke, recurrent hospitalization for MI or unstable angina, heart failure, and recurrent MI Dr Haffner: the cardiovascular risk of patients with diabetes who have not had an MI is comparable with that of nondiabetic patients who have sustained an MI
Pathophysiology of hypertension in DM The derangements in glucose, lipid, and protein metabolism lead to n functional abnormalities in autonomic nerves n overproduction of vasoconstrictor factors that increase vascular tone n concomitant reductions in the biologic actions of vasodilators resulting in an increase in BP
Vasoactive substances Cause structural changes in the CV system and in the kidney through effects on n Vascular smooth muscle cell hypertrophy n Hyperplasia, angiogenesis, cellular apoptosis, macrophage/fibroblast activation with augmented formation of extracellular matrix n Adhesive interactions of circulating leukocytes and platelets with the vessel wall
Processes important in the development or perpetuation of hypertension in diabetics n n Alterations in the balanced production of vasodilator & vasoconstrictor substances from the endothelium Altered vascular smooth muscle responses to these substances Resistance of peripheral tissues & selected lipid metabolic processes to the actions of insulin Alterations in the cellular & extracellular elements that comprise the vessel wall
Reactive oxygen species (ROS) Diabetics—increased metabolic processes that produce reactive oxygen species (ROS) n ROS serve as signaling mechanisms mediate many of the functional & structural vascular abnormalities observed in diabetics n Thus, hypertension in diabetics probably results from a series of interrelated, complex functional and structural abnormalities n
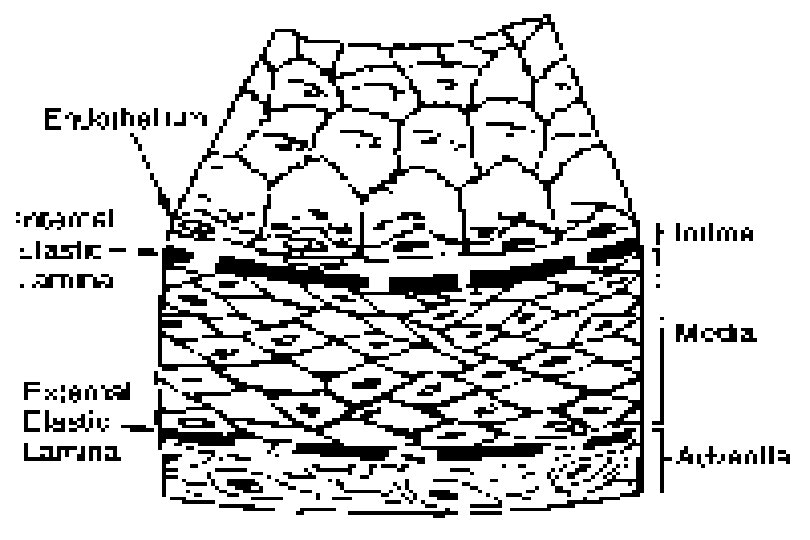
Endothelial dysfunction in DM
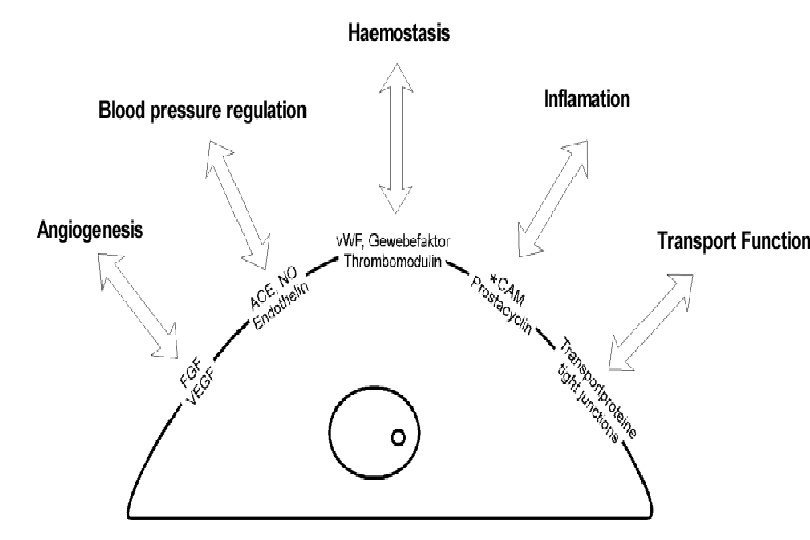
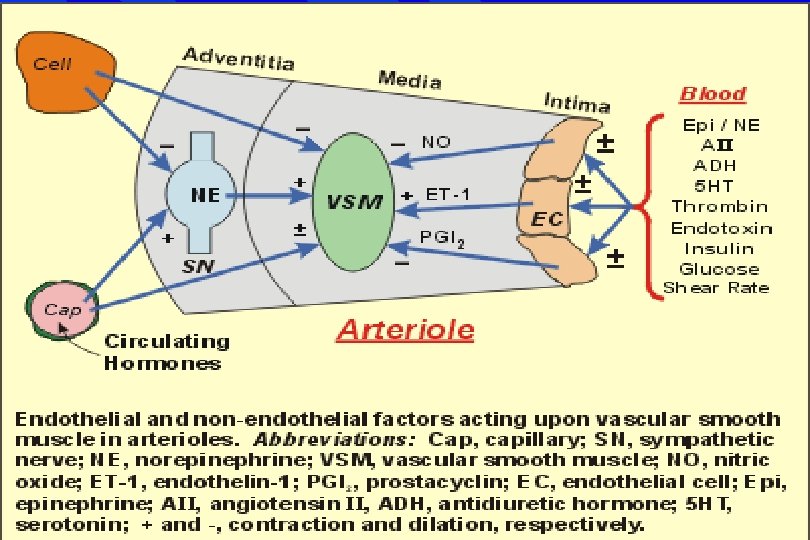
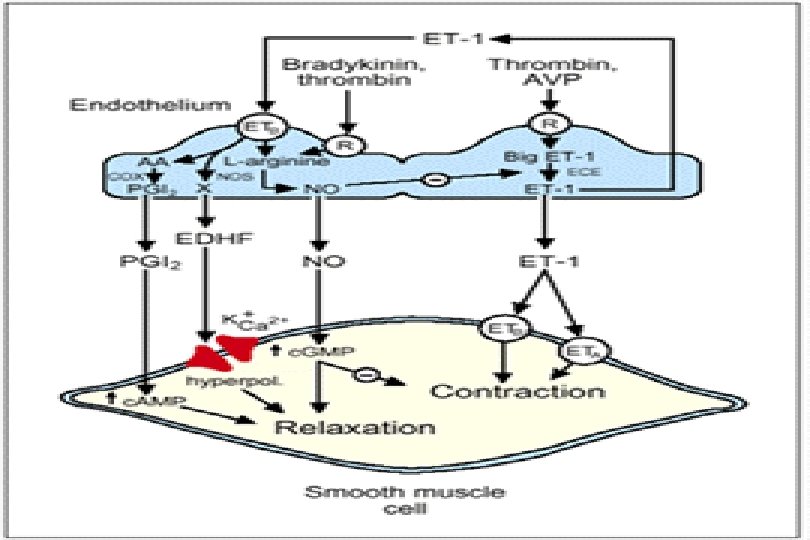
Endothelial production of vasoactive factors Normal endothelium is pivotal in the maintenance of normal vascular homeostasis through a balanced production of vasodilator and vasoconstrictor substances n Endothelium-derived vasodilators n Endothelium-derived vasoconstrictors
Endothelium-derived vasodilators Nitric oxide (NO) n Adrenomedullin n Endothelium-derived hyperpolarizing factors n Prostacyclin (PGI 2) è relax vascular smooth muscle in both arteries and veins è NO and PGI 2 also inhibit platelet aggregation è NO also interferes with the vascular inflammatory process by decreasing the adhesive interactions between the endothelium and circulating leukocytes, thus interfering with the atherosclerotic process n
Vasoconstrictors From the sympathetic nerves, circulation, endothelium n Norepinephrine (NE) n Angiotensin II n Thromoxane A 2 n 5 -hydroxyeicosatetaraenoic acid (5 -HETE) n Endothelin (ET)-1
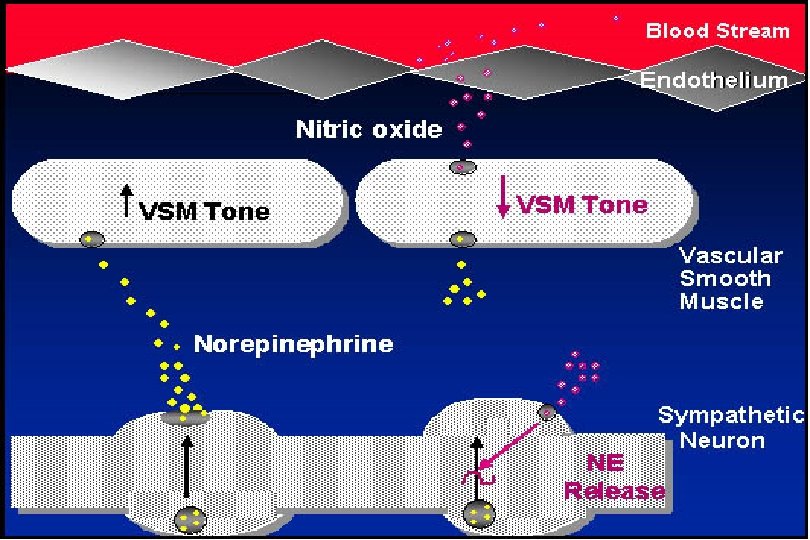
Endothelium-dependent vasodilator and vasoconstrictor mechanisms
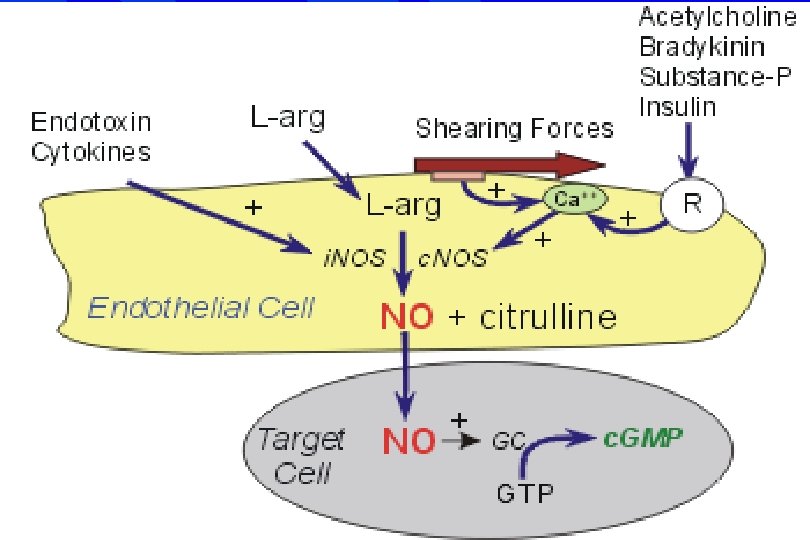
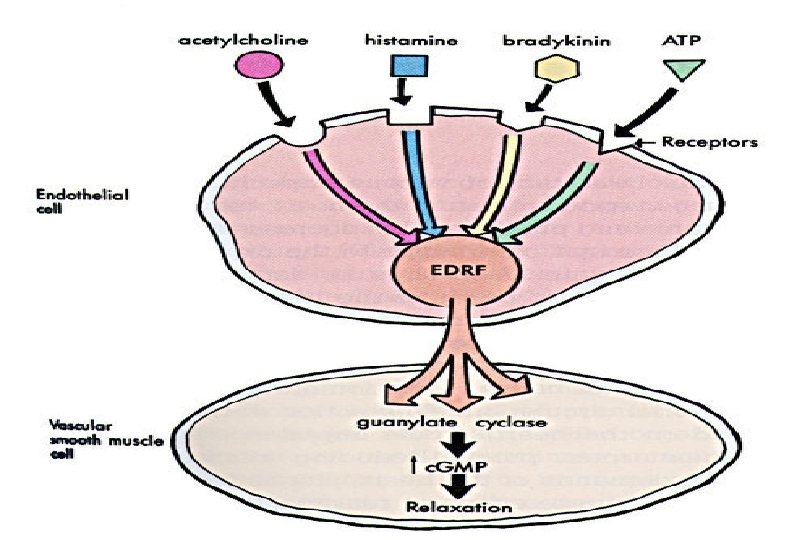
Endothelium-derived NO & vascular tone n n NO-a potent mediator of vascular relaxation through action on soluble c. GMP in VSMC to inhibit ca-dependent contraction NO synthesis & release occurs continuously under basal conditions & can be increased through activation of muscarinic, thrombin, purinergic, and ETB receptors in the endothelial-cell plasma membrane that mediate the actions of acetylcholine, thrombin, ADP, and ET-1 respectively Changes in vascular wall shear forces associated with increased flow also increase NO release Sustained increase in BP-by continuous administration of stereoselective inhibitors of NO synthase further indicates. NO is important in maintenance a vasodilated state.
NO and endothelial dysfunction in diabetes n n Type 1 diabetes--impaired endothelium-dependent vasodilation in response to acetylcholine and similar agonists that stimulate the release of NO Type 1 and 2 diabetes—endothelium-dependent vasodilatory responses to brachial artery infusions of acetylcholine, methacholine, and similar agonists are impaired in the forearm In normotensive type 2 diabetes—demonstration of blunted endothelium-dependent vasodilation suggests that the endothelial abnormalities cannot be ascribed solely to the impaired endothelium-dependent vasodilation Contribution of prostaglandins to abnormalities in endothelial function is minimal
Mechanisms of impaired endotheliumderived vasodilation in diabetes Biologic actions of NO are diminished in diabetes, but production of NO is actually increased n Increase in the production of ROS by several vascular components in diabetics n Interactions of NO & superoxide anion within the microenvironment of the vessel wall-inactivation of NO & formation of the potent oxidant radical, peroxynitrite (OONO-) n
Hyperglycemia in DM n n Associated with diminished biologic actions of NO Tesfamariam: impaired vasodilatory responses to high glucose levels--caused by increased oxygen-derived free radicals through a protein kinase C-mediated mechanism that stimulates the formation of vasoconstrictor prostanoids The vasoconstrictor effect can be abolished by aldose reductase inhibitors High glucose increase both NO synthase expression & superoxide anion generation by aortic endothelial cells.
Dyslipidemia in DM (1) n n n Elevated TG, low HDL-c, and elevated IDL—insulin resistance syndrome Hypercholesterolemia is associated with impaired endothelium-dependent vasodilation in human forearm & pig coronary arteries & rabbit aorta These functional vascular changes associated with Increase generation of ROS Persistence of endothelial NO release Increased generation of OONOOxidative modification of LDL
Dyslipidemia in DM (2) n n n The extent of ROS formation-also be a determinant of endothelial NO release-it may affect the proportion of circulating and tissue cholesterol that has been oxidized Oxidatively modified LDL--impair endothelium-dependent vasodialtion more than native LDL in vascular ring Hypertriglyceridemia-independent risk factor for CAD Postprandial hypertriglyceridemia--cause a transient impairment of endothelium-dependent vasodilation in normal volunteers Postprandial hypertriglyceridemia is more exaggerated in type 2 diabetics & associated with higher forearm venous free radical & greater impairment of flow-dependent vasodilation
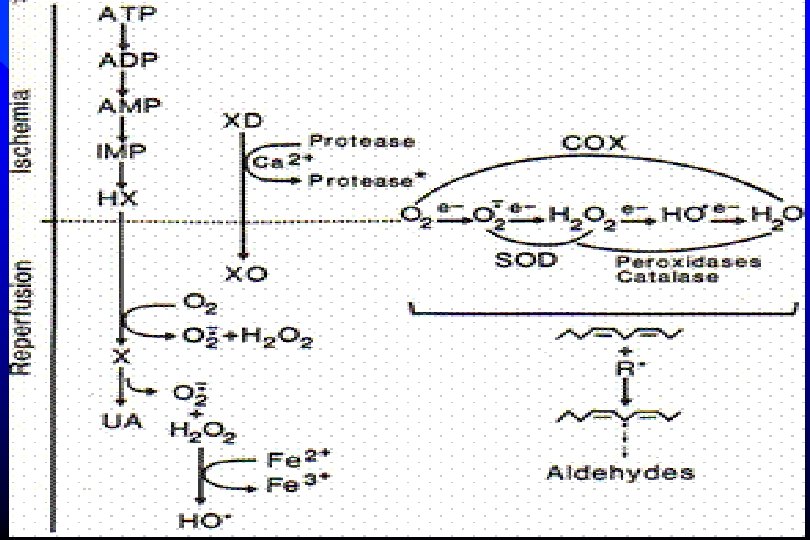
Increased oxidative stress in diabetes n n n Oxidative stress—imbalance between the production of ROS and the numerous antioxidant defense mechanisms present in biologic systems Reactive oxygen species (ROS) include superoxide anion that is converted to hydrogen peroxide both enzymatically and by several isoforms of the enzyme superoxide dismutase In diabetes, overproduction of ROS overwhelms normal antioxidant defenses with consequent alterations in both the function and the structure of the CV system
The reduction of oxygen O 2+ e- -------- O 2. - (superoxide radical) n O 2. - + 2 H+ +e- ---- H 202 (hydrogen peroxide) n H 2 O 2 + e- ------ OH- + OH. (hydroxyl radical) n OH. + e- ------- OH- (hydroxyl ion) n 2 OH- + 2 H+------- 2 H 2 O n Overall O 2 +4 H+ + 4 e- ---- 2 H 2 O n
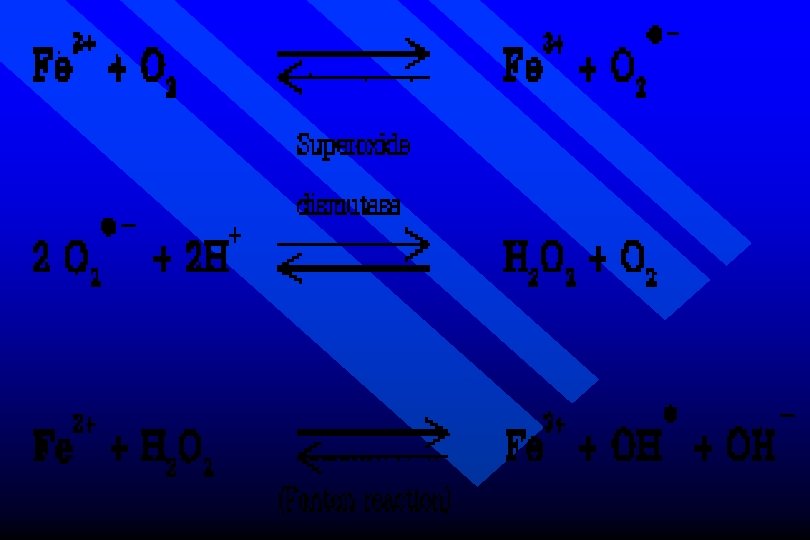
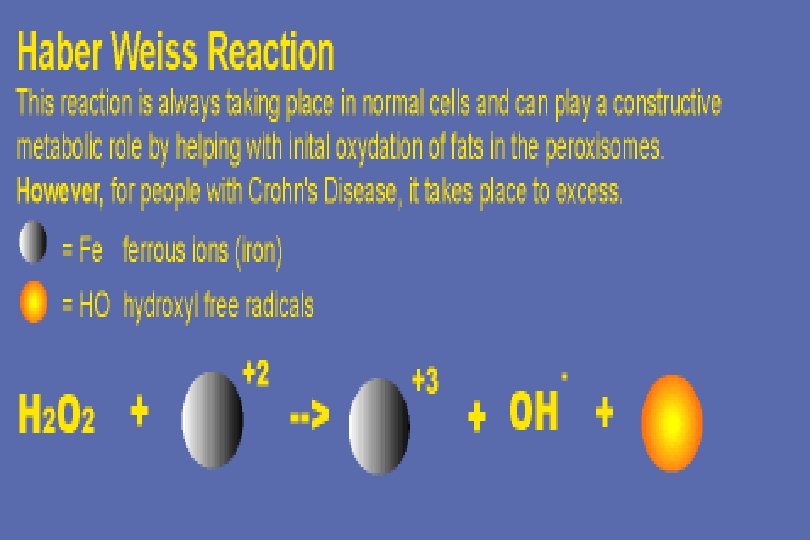
Fe 2+, Cu can cause biological damage O 2 + Fe 2+ Fe 3+ + O 2. n 2 O 2. - +2 H+ H 2 O 2+ O 2 n H 2 O 2 + Fe 2+ OH. + OH- + Fe 3+ (Fenton reaction) n This makes highly damaging hydroxyl radical n O 2. - + H 2 O 2 Cu, Fe OH. + OH- + O 2 n
Source of OH. Might be the reaction. of O 2 with NO O 2. - + NO. ONOO- (peroxynitrite) n ONOO- + H+ ONOOH n ONOOH “ OH-like species” n
Sources of reactive oxygen species in DM Enzyme or processes Tissue source NADP(H) oxidase VSMCs, leukocytes Hemeoxygenase-1 Endothelium, VSMCs Mitochondrial oxidation All cells Cyclooxygenase, lipoxygenase Endothelium, VSMCs Cytochrome P 450 monooxygenases All cells Xanthine oxidase Endothelium, VSMCs
Production of ROS by circulating leukocytes ROS generated by isolated lymphocytes without stimulation or after exposure to the formyl tripeptide, f. MLP, was significantly higher in type 2 DM n Most of the increased ROS was blocked by the addition of sodium azide, a scavenger of singlet oxygen and of hydrogen peroxide, but not by superoxide dismutase n
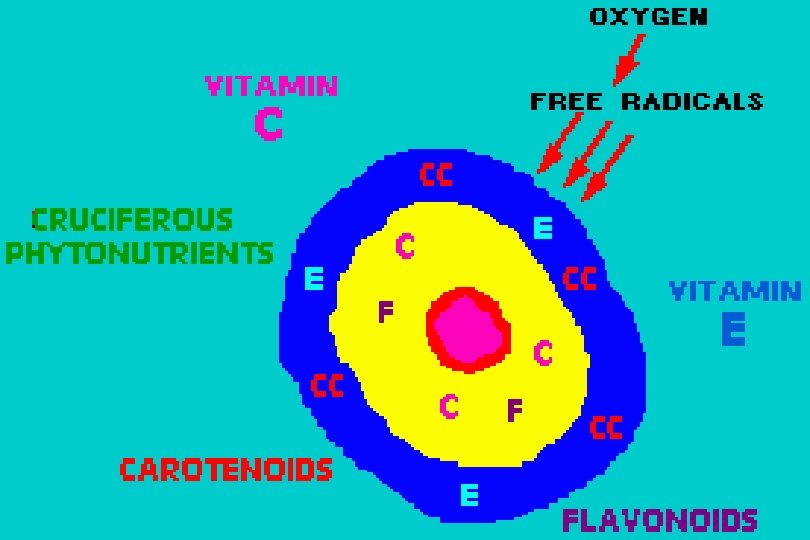
Antioxidants n n n Antioxidants reported to reverse the pathologic alterations for which ROS are thought to be resposible Acute exposure of isolated tissues or intact animals with experimental diabetes to superoxide dismutase either alone or in combination with catalase reported to improve or normalize impaired endothelium-dependent vasodilation Simultaneous infusion of ascorbate and methacholine into the brachial artery of type 1 or type 2 diabetes was reported to augment forearm blood flow compared with the response to methacholine alone
Antioxidants n n n The investigators reported that no effect of vitamin C on endothelium-independent vasodilation produced by either sodium nitroprusside or verapamil and didnot improve endothelium-dependent vasodilation in nondiabetic subjects Recently reported that ascobate restores the trnsient blunting of endothelium-mediated vasodilation in nondiabetic individuals with acute hyperglycemia The results of chronic supplementation with vitamin C, vitamin E, and b-carotene have shown no significant retardation of CV disease progression
Nutrients and antioxidant defence Nutrient Examples of useful roles in the human body Iron Catalase, correct functioning of mitochondri, Hb Manganses Mn-SOD in mitochondria Copper Cu, Zn-SOD, caeruloplasmin Zinc Cu, Zn-SOD: more generalized antioxidant properties? Stabilizer of membrane structure Proteins Sulphur-containing amino acids are needed to make GSH. SODs, catalase, glutathione reductase and peroxidases, metal transport, and storage proteins. Albumin may be a “sacrificial” antioxidant carrier of copper in plasma Riboflavin Glutathione reductase, correct functioning of mitochondria, needed to make FMN and FAD Selenium Glutathione peroxidases; thyroid funciton; may aid detoxification of carcinogens Vitamin E Protection against lipid peroxidation; may also help to stabilize membrane structure Vitamin C Hydroxylase enzymes, water-soluble antioxidant, recycles vitamin E, reduces nitrosamine carcinogens B-carotene Precursor of vitamin A. May have some antioxidant properties-powerful scaverger of singlet O 2, may react with peroxyl radicals. Some reports that it inhibits lipid peroxidation in membranes, but only at low O 2 concentrations Lycopene Orange-red pigment in tomatoes. Powerful scavenger of singlet )2. Suggested to be an antioxidant in vivo, but this has not yet been established Retinol (Vit A) Some antioxidant properties demonstrated in vitro, but no good evidence that it acts as an antioxidant in vivo Nicotinamide Needed to make NAD+, NADH, NADP+, NADPH—needed for glutathione reductase.
Insulin resistance syndrome and endothelial dysfunction n Syndrome of insulin resistance may precede the onset of overt type 2 diabetes The clinical features include hyperinsulinemia, truncal obesity, hypertension, and dyslipidemia characterized by elevated serum TG, low HDL-C, and increased IDL These hallmarks are thought to result from relative insensitivity of selected tissues, particularly skeletal muscle, to the action of insulin
Insulin resistance syndrome n n n It is hypothesized that compensatory hyperinsulinemia maintains the serum glucose within the normal range until pancreatic islet b-cells can no longer produce sufficient insulin, and overt type 2 diabetes occur Insulin resistance is associated with a clustering of CV risk factors that predispose patients with this metabolic syndrome to later CV events There is evidence of sympathetic nervous system activation that may contribute to the hypertension that develops.
Insulin resistance syndrome Insulin itself promotes vasodilation, in part through stimulation of endothelial NO release n This vasodilatory action may be counterbalanced in the insulin resistance syndrome by the development of hypertension, which independently impairs endothelium-dependent vasodilation n
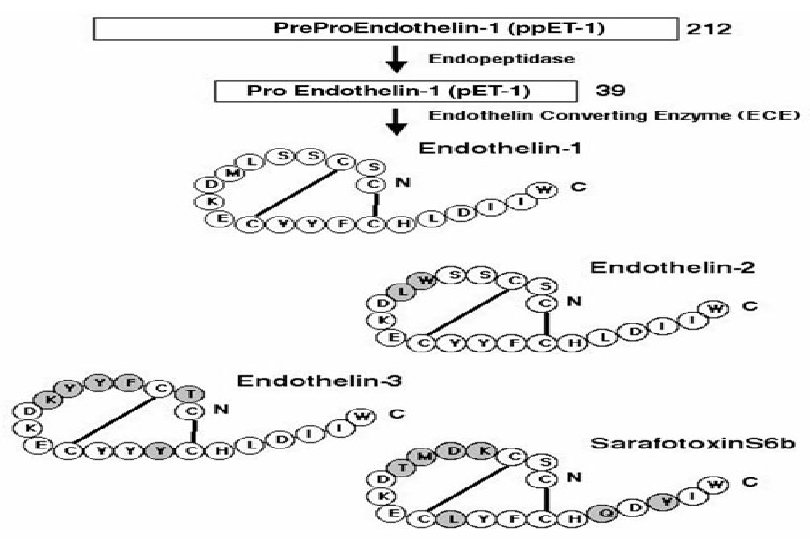
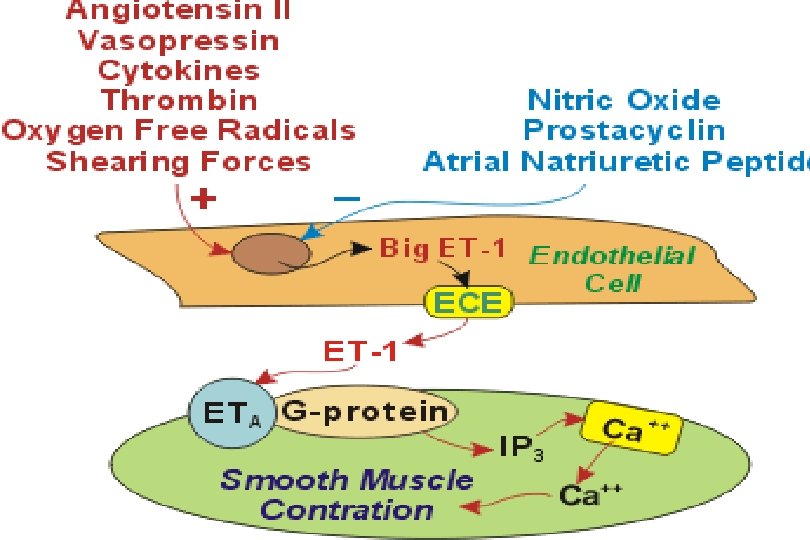
Endothelin and endothelial dysfunction in diabetes Endothelin-1, a 21 -amino-acid peptide, is the predominant isoform of the endothelin peptide family that includes ET-2, ET-3, and ET-4 n Endothelin-1 is produced primarily by endothelial cells but can also be synthesized by vascular smooth muscle cells (VSMCs) and by macrophages n The action of ET-1 are mediated by 2 receptor subtypes, ETA and ETB receptors n
Endothelin n ETA receptor mediate the vasoconstrictor effects of the peptide, ETB receptors on the endothelium stimulates synthesis of NO Increased ET-1 associated with decreased endotheliumdependent vasodilation, a reduction in the biologic actions of NO, and an increased production of oxygen-derived free radicals These effects are thought to contribute to heightened vasoconstriction and increased blood pressure increased monocyte adhesion to the vascular wall increased thrombosis a vascular inflammatory response augmented proliferation of VSMCs
Endothelin in DM n n n Plasma ET-1 are increased in type 2 diabetes Most of the ET-1 cause vasoconstriction of VSMCs through a paracrine effect mediated by ETA receptors Infusion of ET-1 cause sustained increases in BP Nonselective ETA/ETB antagonist, bosentan, lowers BP in patients with essential hypertension Plasma ET-1 -may be a marker for atherosclerotic disease in type 2 diabetic patients ET-1 participate in the fibrotic process--an essential component of the glomerulosclerosis, cardiac and vascular remodling, and atherosclerosis that occur at an accelerated rate in hypertensive type 2 diabetics
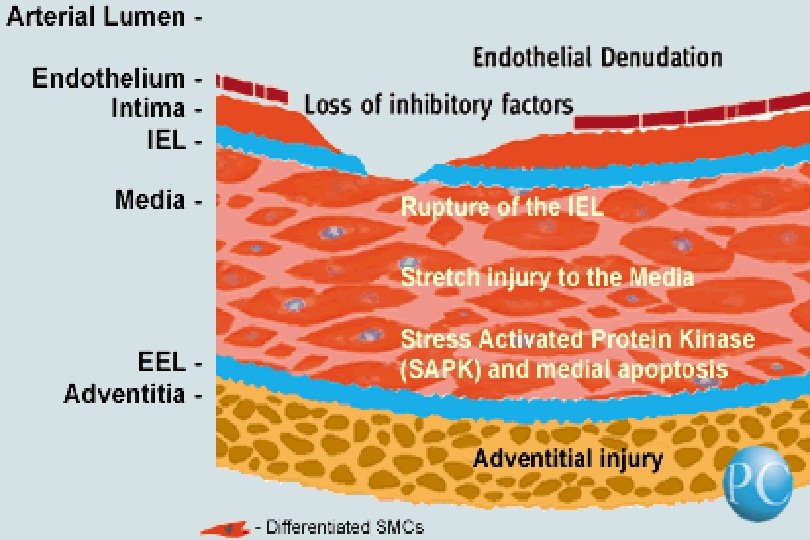
The contribution of diminished arterial compliance to hypertension in diabetes n n n The large conduit arteries, such as aorta, and major muscular arteries, such as carotid, brachial, radial, renal, and femoral arteries, tend to become less distensible with advancing age and in diabetic pts independent of age The loss of arterial compliance is associated with an increase in systolic BP, a fall in diastolic BP, and a widening of the pulse pressure Widened pulse pressure is an independent predictor of CV risk, more potent than either systolic or diastolic BP
Diminished arterial compliance to hypertension in diabetes n n Distensibility is reduced by arterial wall structural alterations produced by atheroscelrotic plaques Accompanied by a change in the protein composition of the extracellular matrix of the arterial wall--as the replacement of elastic collagen with less distensible collagen Expansion of the acellular extracellular matrix accompanied by a reduction in vascular wall cellularity Vasoactive substances such as endothelin, angiotensin, and diminished NO may contribute to these changes in arterial wall structure
Advanced glycation end products (AGEs) n n n AGEs formed by the nonenzymatic binding of glucose to lipids or to free amino groups on proteins The formation of AGEs is inhibited by NO, whose biologic actions are blunted in diabetics The increased stiffness of the arterial wall contributes to isolated hypertension The increased systolic pressure in turn produces an increased workload on the left ventricle, resulting in increased left ventricular mass Reduction arterial wall compliance linked to increased CV risk in type 1 & 2 diabetics and occur early in the course of DM before vascular disease is clinically apparent
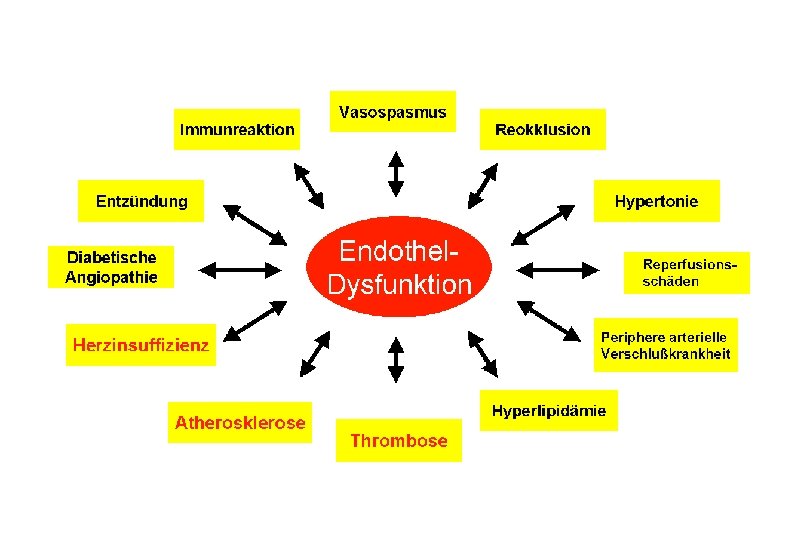
Adverse consequences associated with endothelial dysfunction in diabetes mellitus n n n Decreased NO formation, release, and action Increased formation of reactive oxygen species Decreased prostacyclin formation and release Increased formation of vasoconstrictor prostanoid Increased formation and release of ET-1 Increased lipid oxidation Increased cytokine and growth factor production Increased adhesion molecule expression Hypertension Changes in heart and vessel wall structure Acceleration of the atherosclerotic process
Endothelial dysfunction in hypertension and diabetes: effects of treatment n n Treatment of HTN with any agent that lowers BP could improve impaired endothelium-dependent vasodilation BP reduction with nonselective agents may have a different effect in diabetics than in nondiabetics with HTN, because shear stress abnormalities seem to contribute to endothelial dysfunction in hypertensives but not in type 2 diabetics ACEI seem to be particularly beneficial in improving or normalizing blunted endothelium-dependent vasodilation in some patients with type 1 and type 2 diabetes Recently, restoration of impaired endothelium-dependent vasodilation in type 2 diabetics occurred after Tx with angiotensin II AT 1 receptor antagonist, losartan
Effects of treatment n n Reduction in the formation of or a blockade of the action of angiotensin II, a potent vasoconstrictor that is responsible for increasing ROS formation by VSMCs Angiotensin II is also either directly or indirectly responsible for additional vascular effects, including increased proinflammatory adhesion molecule expression, increased cytokine and growth factor expression, increased ET-1 formation, and an increase in endothelial scavenger receptors for oxidized LDL cholesterol
Effects of treatment n n Thus, ACEI inhibit all these deleterious downstream effects and potentiate the action of bradykinin by inhibiting its breakdown These selective angiotensin II-mediated adverse effects on the vasculature, on the heart, and on the kidney may account for the substantial benefit on morbidity and mortality observed in diabetic patients at risk for CV and renal disease treated with an ACE inhibitor compared with placebo
Summary (1) n n n There is compelling evidence for endothelial dysfunction in both type 1 and type 2 diabetics This dysfunction is manifest as blunting of the biologic effect of a potent endothelium-derived vasodialtor, NO, and increased production of vasoconstrictors such as angiotensin II, ET-1, and cyclooxygenase and lipoxygenase products of arachidonic acid metabolism These agents and other cytokines and growth factors whose production they stimulate cause acute increases in vascular tone, resulting in increases in BP, and vascular and cardiac remodling that contributes to the microvascular, macrovascular, and renal complications in diabetes
Summary (2) Reactive oxygen species, overproduced in diabetics, serve as signaling molecules that mediate many of the cellular biochemical reactions that result in these deleterious effects n Treatment with antioxidants and with inhibitors of the renin-angiotensin system may reverse some of the pathologic vascular changes associated with endothelial dysfunction n