Pathophysiology L 9 Disorders of the respiratory system

 may be affected by various disease processes. These")























 1. Mild intermittent: 2")






 : Cause")
 : Used")
. Acute bronchitis: Inflammation of")





 Chronic cigarette smokers > 95%. Chronic inflammation")



 Traumatic chest wound.")





 ARDS is a syndrome associated with destruction of: Alveolar")











- Slides: 66
Patho-physiology L 9 Disorders of the respiratory system Prof. Fakhir Al-Ani fakeralani 2000@yahoo. com
Respiratory structures (airways, alveoli & pleura) may be affected by various disease processes. These respiratory diseases include: 1. Infections: - Pneumonia, Acute bronchitis. 2. Obstructive disorders: - Asthma, ch. bronchitis & emphysema. 3. Restrictive disorders : - Pneumothorax, Atelectasis, respiratory distress syndrome & cystic fibrosis. 5. Exposure to Inhaled particles: - Carbon, Asbestosis Silicosis. 4. Cancers
Respiratory infections Infections of the respiratory tract: 1. Upper respiratory tract 2. Lower respiratory tract 3. Both. Organisms include: 1. Bacteria. 2. Viruses: Most common 3. fungi. 4. Others like Chlamydia, rickettsia The manifestations = Mild severe (even life threatening). Depending on the organism & extent of infection
Upper respiratory tract Infections Common cold Most common virus: - rhinovirus, parainfluenza virus, respiratory syncytial virus, adenovirus. Characterized by: - Seasonal variations. - Spread via respiratory secretions. - Enter body through nasal mucosa & eye surfaces. Clinical Manifestations: Rhinitis (Nasal discharge & congestion) Sinusitis Pharyngitis Headache
Upper respiratory tract Infections Influenza Ø Influenza: Viral infection affects upper & lower respiratory tract. Types: A, B & C. Type A: - most common & causes most serious illness. Ø Influenza virus: Highly transmissible respiratory pathogen. High genetic mutation So forming new variant of virus around the world. Ø Serious pandemics: Seen every 8 - 10 ys as a result of this genetic mutation.
Upper respiratory tract Infections Influenza Symptoms: - Headache, Fever, chills, - Muscle aches - Nasal discharge, Unproductive cough, Sore throat Marked inflammation of respiratory epithelium Acute tissue damage & a loss of ciliated cells (protect respiratory passages from other organisms) Co-infection of the respiratory passages with bacteria. My infect lung tissues cause a viral pneumonia.
Upper respiratory tract Infections Influenza Treatment of influenza: Bed rest, fluids, warmth Antiviral drugs ? ? ? Influenza vaccine : - Protect against A & B influenza - The vaccine must be updated & administered yearly (Not effective against strains not included). - The vaccine is particularly indicated in: Old people Individuals weakened by other disease. Health-care workers
Upper respiratory tract Infections Influenza Drugs for Treating Influenza: Amantidine: Effective only against type A influenza Used orally or aerosol administration Inhibits viral fusion, assembly & release from infected host cell. Neuraminidase inhibitors: Effective against both type A & B influenza - Zanamavir: - Used by inhalation - Oseltamivir: - Used orally Inhibits activity of viral neuraminidase enzyme that is necessary for spread of the influenza virus
Lower respiratory tract Infections The lower respiratory tract is protected by effective defense mechanisms to prevent infection. Ø So organism to reach LR tract must be: - Virulent. - Present in very large number. - The host defense barriers must be weakened. Ø Factor weaken the respiratory defense barriers: - Cigarette smoking: - Paralyze the cilia lining. So impair removal of secretions, particles & microorganism so. - Presence of a respiratory pathogen like virus infection.
Lower respiratory tract Infections Defenses of the Respiratory System 1. Moisture & mucus-covered surfaces: Trap particles & organisms 2. Ciliated epithelium: Clears trapped Particles & Organisms from passages. 3. Cough reflex & epiglottis: Prevents aspiration of particles & irritants 4. Cell surface Ig. A & lysosomes 5. Pulmonary macrophages: Phagocytize foreign particles & organisms in Avelo.
Lower respiratory tract Infections Pneumonia: - Inflammation of the alveoli or interstitial spaces by bacteria or viruses. Ø The prevalence & severity of pneumonia recently due to Antibiotic resistance & HIV &. Ø Pneumonia may be classified according to the pathogen that is responsible for the infection: - Pneumonia in the hospital setting. - Pneumonia in the community setting.
Pneumonia Individuals at Risk for Pneumonia 1. Old age 2. Smokers 3. Viral infection 4. Chronic illness 5. Patients with chronic respiratory disease e. g. bronchial asthma. 5. AIDS or immuno-suppressed patients
Potential Pathogens Typical - Streptococcus pneumoniae - Hemophilus influenzae - Mycobacterium catarrhalis - Klebsiella pneumoniae Atypical - Chlamydia pneumoniae - Legionella pneumophila - Mycoplasma pneumoniae. - Viruses (in adult) - Fungi
Potential Pathogens Less Common pathogens - N. meningitidis - Chlamydia psittaci - B. anthracis - Y. pestis
Pneumonia Classification / Causes 1. Community acquired pneumonia 2. Aspiration pneumonia 3. Hospital - Hospital acquired pneumonia - Ventilator associated pneumonia - Healthcare associated pneumonia
Pneumonia Classification/Path. 1. Broncho Penumonea. 2. Lobar Penumonea. 3. Atypical Penumonea.
Pneumonia Classification/ Clinical 1. Typical pneumonia - Usually bacterial in origin. - Organisms replicate in the alveoli. Manifestations: - Purulent sputum. - Some degree of hypoxemia. - Inflammation + WBCs infiltration - High fever, chest pain, chills, & malaise. - Fluid accumulation in the alveoli & Exudation seen by X-ray.
Pneumonia Classification 2. Atypical pneumonia: - Usually viral in origin. - Organisms replicate in spaces around the alveoli. Manifestations: Milder symptoms. Lack of WBCs infiltration in alveoli. Lack of fluid accumulation in the alveoli. Not usually evident on radiographs. May make the patient susceptible to bact. pneumonia.
Pneumonia Opportunistic organisms - Organisms not commonly associated with respiratory illness in healthy individuals. - Occurs in patients with HIV & immunocompromised patients. - These organisms include mycobacteria, fungus (Histoplasma) & protozoa (Pneumocystis carinii). - Treatment of these organisms requires specific drug therapy & in the case of protozoa & fungi the organisms are very difficult to treat.
Pneumonia Treatment of pneumonia: - Antibiotics: In bacterial infection. Consider possibility that antibiotic-resistant. - Oxygen therapy for hypoxemia. - Vaccine: For pneumococcal pneumonia. It available & highly effective. Important in high-risk individuals.
Obstructive Respiratory Disorders Bronchial asthma Asthma: - Reversible broncho-spasm - Inflammation of airway passages due to “hyper reactivity” on exposure to certain “triggers”. - The exact etiology is still uncertain: Genetic predisposition may be a cause. - The incidence has been steadily recently.
Obstructive Respiratory Disorders Bronchial asthma Ø Asthmatic patients produce large amounts of the antibody Ig. E attached to the mast cells present in many tissues. Ø Exposure to "a trigger" like pollen result in the allergen-binding mast cell-bound Ig. E, causes the release of inflammatory mediators such as Histamine , Leukotrienes and Eosinophilic Chemotactic factor. Ø The response of a patient with asthma to these triggers can be divided into an “early phase” & a “late phase. ”
Mechanism of Asthma
Obstructive Respiratory Disorders Bronchial asthma Some Potential Asthma Triggers ü Allergens (Pollen, pet dander, fungi, dust mites) ü Cold air ü Pollutants ü Cigarette smoke ü Strong emotions ü Exercise ü Respiratory tract infections
Pathological changes in asthma
Obstructive Respiratory Disorders Bronchial asthma Clinical Classification of Asthma (Friquency) 1. Mild intermittent: 2 times / week or less 2. Mild persistent: > than 2 times/ week 3. Moderate persistent: Daily & severe enough to affect activity 4. Severe persistent: Very frequent & persist for a long period
Obstructive Respiratory Disorders Bronchial asthma Early phase of asthma: 1. Bronchospasm. 2. Edema of the airways 3. Excess mucus. 4. Bronchiole obstruction (early phase of asthma) Bronchospasm> inflammation Release of inflam. mediators Histamine, PGs & Bradykinin
Obstructive Respiratory Disorders Bronchial asthma Late phase of asthma: 1. Several hours after initial onset of symptoms. 2. Inflammatory response > edema 3. The inflammatory response is via Eosinophils which stimulate mast cell degranulation & release subs. that attract other WBCs. Subs. infiltration of the airway tissues with WBCs such as Neutrophils & lymphocytes also contributes to the overall inflammatory response of the late phase.
Obstructive Respiratory Disorders Bronchial asthma Manifestations of asthma : ØCoughing, wheezing ØDifficulty breathing ØRapid, shallow breathing ØExcess mucus production ØSignificant anxiety
Obstructive Respiratory Disorders Bronchial asthma Severity staging of an Acute Asthma Attack Stage I (Mild): - Stage II (Moderate): Stage III (Severe): - Mild Dyspnea Diffuse wheezing Adequate air exchange Respiratory distress at rest Marked wheezing Marked respiratory distress Cyanosis Marked wheezing or absence of breath sounds Stage IV (Respiratory failure): - Respiratory distress, lethargy, confusion, prominent pulsus paradoxus
Obstructive Respiratory Disorders Bronchial asthma Complications of asthma can include : Status asthmatics: A life-threatening condition of prolonged bronchospasm that is often not responsive to drug therapy. Pneumothorax : Due to lung Pr. that can result from the extreme difficulty involved in expiration during a prolonged asthma attack. Respiratory failure: Marked hypoxemia & acidosis might occur.
Obstructive Respiratory Disorders Bronchial asthma Treatment of asthma: Based on the frequency & severity of asthma attacks Include the following: 1. Avoidance of triggers & allergens. Improved ventilation of the living spaces. Use of air conditioning. 2. Bronchodilators: - (albuterol, terbutaline) Short acting β-Adrenergic agonist. Given on need in the form of a nebulizer solution. or may be given subcutaneously. They block bronchoconstriction but do not prevent the inflammatory response.
Obstructive Respiratory Disorders Bronchial asthma Treatment of asthma: 3. Xanthine drugs (theophylline) : Cause bronchodilation & inhibit late phase asthma. They are used orally as second-line agents in combination with other asthma therapies (steroids). They have significant CNS, CVS & GIT side effects that limit their overall usefulness. 4. Cromolyn sodium : Anti-inflammatory (blocks both early & late asthma). They may involve mast cell function or response to allergens.
Obstructive Respiratory Disorders Bronchial asthma Treatment of asthma: 5. Anti-inflammatory drugs (corticosteroids) : Used orally or inhalation to stope inflammatory response of asthma. The most significant unwanted effects occur with longterm oral use of corticosteroids (immunosuppression , increased susceptibility to infection, osteoporosis & effects on other hormones such as the glucocorticoids). 6. Leukotrienes modifiers (Zafirlukast) : New class of agents that blocks the synthesis of the key inflammatory mediators, leukotrienes.
Obstructive Respiratory Disorders Bronchitis: Obstructive respiratory disease (acute & chronic). Acute bronchitis: Inflammation of the bronchi most commonly caused by infection (bacteria or viruses). It is generally a self-limiting condition in healthy individuals but it is of severe consequences in individuals who are weakened with other illness or who are immunocompromised. Symptoms of acute bronchitis often include productive cough, Dyspnea & possible fever.
Obstructive Respiratory Disorders Bronchitis Chronic bronchitis: Chronic obstructive pulmonary disease most frequently associated with: - Cigarette smoking (90% of cases). - prolonged exposure to inhaled particulates (coal dust or other Air pollutants). Chronic bronchitis is characterized by excess mucus production in the lower respiratory tract.
Obstructive Respiratory Disorders Bronchitis Mucus production in lower respiratory tract. Function of the ciliated epithelium Prevent the clearing of debris & organisms. Patients often suffer repeated bouts of acute respiratory infection Patients sufferers “blue bloaters” as a result of the cyanosis & peripheral edema.
Obstructive Respiratory Disorders Bronchitis Manifestations of chronic bronchitis: ü Productive, chronic cough ü Production of purulent sputum ü Frequent acute respiratory infections ü Dyspnea ü Hypoxia, cyanosis ü Symptoms of cor pulmonale ü Fluid accumulation (edema) in later stages
Obstructive Respiratory Disorders Bronchitis Treatment of chronic bronchitis: 1. Cessation of smoking or exposure to irritants 2. Bronchodilators to open airway passages 3. Expectorants to loosen mucus 4. Anti - inflammatory to relieve airway inflammation and reduce mucus secretion 5. Prophylactic antibiotics for respiratory infections 6. Oxygen therapy
Obstructive Respiratory Disorders Emphysema Respiratory disease that is characterized by Destruction & permanent enlargement of terminal bronchioles & alveolar air sacs
Obstructive Respiratory Disorders Emphysema Etiology: - (Uncertain) Chronic cigarette smokers > 95%. Chronic inflammation of the alveolar airways (infiltration by lymphocytes & macrophages). Excess release of protease enzymes such as trypsin from lung tissues & leukocytes can digest & destroy the elastic walls of the alveoli. Decrease levels of a protective enzyme α-1 -antitrypsin They can not inactivates protease enzymes (trypsin) in lung tissue. α-1 -antitrypsin smoker individuals
Obstructive Respiratory Disorders Emphysema alveolar elasticity Destruction of alveoli Alveolar surface area for gas exchange. Clinical Manifestations: 1. Tachypnea ( respiratory rate): to maintain good arterial B. gases & prevent hypoxia or cyanosis. 2. Barrel chest from prolonged expiration. 3. Lack of purulent sputum. 4. Long-term consequences (cor pulmonale) & respiratory failure.
Comparison of Symptoms for Chronic Bronchitis and Emphysema Chronic bronchitis Mild Dyspnea Productive cough Cyanosis common Respiratory infection Onset usually > 40 ys History of smoking Cor pulmonale common Emphysema Sever Dyspnea Dry or no cough Cyanosis rare Infrequent infections Onset usually > 50 ys History of smoking Cor pulmonale in terminal stages
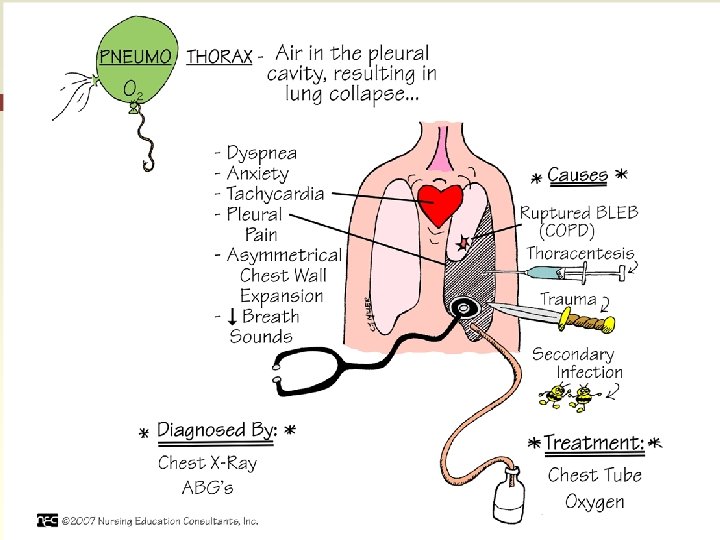
Restrictive Pulmonary Disorders Pneumothorax Entry of air into the pleural cavity in which the lungs reside Normal lung expansion need a negative Pr. within the pleural cavity with respect to atmospheric Pr. When air enters the pleural cavity the -ve Pr. is lost and the lungs collapse. Each lung sits in a separate pleural cavity So Pneumothorax of one plural cavity will not cause collapse of the other lung.
Restrictive Pulmonary Disorders Pneumothorax Types of pneumothorax: 1. Open (communicating type) Traumatic chest wound. Air enters the pleural cavity. Lung collapses 2. Closed or spontaneous pneumothorax Air “leaks” from the lungs into the pleural cavity. Due to lung cancer, rupture, pulmonary disease. Lung collapses
Restrictive Pulmonary Disorders Pneumothorax 3. Tension pneumothorax Ø One-way movement of air into but not out of the pleural cavity. Ø A hole or wound to the pleural cavity Ø Collaps of the lung. Ø A life-threatening condition because Pr. in the pleural cavity continues to & may result even in compression of large B. V. in the thorax.
Restrictive Pulmonary Disorders Pneumothorax Manifestations of pneumothorax: - Tachypnea, Dyspnea - Chest pain - Possible compression of thoracic B. V. & heart, especially with tension pneumothorax Treatment of pneumothorax: 1. Removal of air from the pleural cavity with a needle or chest tube 2. Repair of trauma & closure of opening into pleural cavity
Restrictive Pulmonary Disorders Pneumothorax Atelectasis: Lung expansion due to; - Blockage of the airways - Compression of the alveolar sacs. Types of atelectasis: 1. Absorption atelectasis Bronchial passages block by mucus, tumors or edema (mucous accumulated in ch. bronchitis, cystic fibrosis. 2. Compression atelectasis Due to lung compression by air, blood, fluids or a tumor
Restrictive Pulmonary Disorders Atelectasis Manifestations of atelectasis: - Dyspnea, cough. - Reduced gas exchange. - Shunting of B. to the inflated areas of the lungs. - The ventilation– perfusion coupling ability of the lungs will help ensure that blood is directed to areas of the lungs where gas exchange can still occur. Treatment of atelectasis: - Removal of airway blockage - Removal of air, blood, fluids, tumors, etc. that are compressing lung tissues
Restrictive Pulmonary Disorders Bronchiectasis Abnormal dilation of the bronchus or bronchi. Ø Due to prolonged injury or inflammation of respiratory airways & bronchioles. Ø So associated with chronic respiratory disease, infections, cystic fibrosis, tumor growth or exposure to respiratory toxins. Ø The major manifestations of bronchiectasis are impaired ventilation of the alveoli, chronic inflammation and possible fibrosis of the areas. (Increased dead space)
Adult respiratory distress syndrome (ARDS) ARDS is a syndrome associated with destruction of: Alveolar membranes. & their related capillaries. It may occur as a result of direct injury to the lungs or as a result of dramatic decreases in B. flow to the lung (“shock of lung, ” ).
Possible Causes of ARDS ü Septicemia, uremia ü Trauma ü Inhalation of toxic gases or agents ü Aspiration of gastric contents ü Widespread pneumonia ü Drug overdose ü Systemic shock
Manifestations of ARDS Dyspnea, tachypnea. Hypoxemia: CO 2 is significantly more water soluble than O 2. Still eliminated from the lungs via diffusion; So blood levels of O 2 are more affected by ARDS than CO 2. Hypocapnia may result. Infiltration of lung tissues with immune cells that release inflammatory mediators. Accumulation of fluids in alveoli & around alveolar spaces. Changes in blood p. H due to altered blood levels of CO 2. Pulmonary fibrosis. / Respiratory failure.
Treatment of ARDS O 2 therapy Anti-inflammatory drugs Diuretics to reduce edema Correction of acid–base balance
Respiratory distress syndrome of the newborn Etiology: In premature newborn: Lack of surfactant in the lungs. 1. Surfactant is produced by Type II cells of the alveoli It is formed of phospholipids & proteins. It covers the surfaces of the alveoli to reduce the surface tension & prevents the alveoli from collapse. It also moistens alveolar surfaces to gas exchange. Clinical manifestations become evident immediately at birth and can be rapidly fatal if not treated.
Manifestations of respiratory distress syndrome in the newborn ü Rapid, shallow breathing ü Nasal flaring, grunting upon inspiration ü Lung collapse ü Lung inflammation & damage ü Hypoxemia
Treatment of respiratory distress syndrome in the newborn Delay or prevention of premature delivery of infant if possible. Treatment: - Synthetic surfactant. Exogenous surfactant will need to be supplied until the infant’s lungs have matured to the point where they are producing their own surfactant. - Mechanical ventilation. - Injection of cortisol in the mother prior to delivery may significantly reduce the incidence of respiratory distress syndrome in premature infants. Cortisol has also been shown to stimulate activity of Type II cells.
Respiratory Failure The lungs are unable to Oxygenate the B. sufficiently or remove CO 2 from it. Types: 1. Acute: - Neumothorax. - Opioid drug overdose 2. Chronic: - End result of chronic respiratory diseases
Manifestations of respiratory failure - Hypoxemia & Hypercapnia - Altered blood p. H - Cyanosis (not always present). - CNS symptoms: Slurred speech Confusion Impaired motor function - CVS symptoms: Initial tachycardia & C. O. Followed by bradycardia & C. O.
Respiratory Failure Causes of Respiratory Failure A. Acute - Pneumothorax - Drug overdose (opioids, sedatives) - Pleural effusion - Airway obstruction - Status asthmaticus - Inhalation of toxins or noxious gases. B. Chronic - Emphysema - Interstitial lung diseases - Cystic fibrosis - Pulmonary emboli - Diffuse pneumonia - Pulmonary edema - Spinal cord / brain injury - Congestive heart failure - N-M disorders
Respiratory Failure Treatment of respiratory failure: - Bronchodilators - Correction of blood p. H - Oxygen therapy - Mechanical ventilation
General symptoms of respiratory disease Hypoxia: O 2 in tissues. Hypoxemia: O 2 in arterial B. Hypercapnia : CO 2 in the blood Hypocapnia : CO 2 in the blood Dyspnea : Difficulty breathing Tachypnea : Cyanosis: rate of breathing Bluish discoloration of skin & mucous membranes due to oxygenation of B. Hemoptysis: Blood in the sputum