PATHOLOGY vs Physiology 1 Normal cell MEMBRANE Selective

PATHOLOGY vs Physiology 1
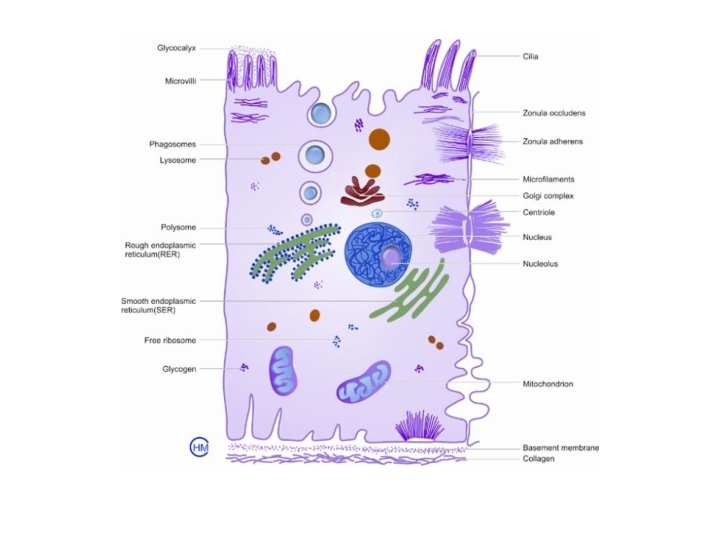

Normal cell • MEMBRANE • Selective pemeability – ions • Surface antigens & receptors • NUCLEUS – DNA – control • CYTOSKELETON 3

Organelles • • • Mitochondria Ribosomes Endoplasmic reticulum Golgi apparatus Lysosomes 4

CELL INJURY 5

Homeostasis, steady state, can be altered. • Limited ways to respond to injury. • 6

STRESS? 7

Cells can and must adapt to stimulus or stress In response to stress, cells may: – Adapt – Be reversibly injured – Die (irreversibly injured) 8

Other responses to stress Intracellular accumulations Pathologic calcification Cellular aging 9


CELL INJURY • Sequence of events that occur in a cell if the limits of adaptive response to a stimulus are exceeded 11

Causes of Cell Injury • Hypoxia and ischemia • “Chemical” agents • “Physical” agents • Infections • Immunological reactions • Genetic defects • Nutritional defects • Aging 12

Oxygen deficiency common and important – Hypoxia reduces aerobic oxidative respiration – Results from l) cardio respiratory failure, 2) loss of blood supply, 3) reduced transport of O 2 in blood (i. e. anemia, or CO toxicity), 4) blockage of cell enzymes (cyanide) Compare with ischemia: loss of blood supply. 13

HYPOXIC INJURY Myocardial infarction Cerebral infarction Renal atrophy

Chemicals and drugs n Chemical poisons - cyanide, arsenic, mercury n Strong acids, alkalis n Environmental pollutants n Oxygen at high concentrations n Hypertonic glucose, salt n Alcohol, narcotic drugs

Chemicals, drugs, toxins multitude of mechanisms - block or stimulate cell membrane receptors, - alter specific enzyme systems, - produce toxic free radicals, - alter cell permeability, - damage chromosomes, - modify metabolic pathways, - damage structural components of cells. 16

Physical agents • • • Trauma, extremes of heat and cold, radiation, electrical energy Pressure changes 17

Infectious agents MICROBIOLOGY – Viruses – Bacteria – Fungi – parasites 18

Immune dysfunction – Immunodeficiency - failure to respond due to congenital or acquired defects – Autoimmunity -- Immune response directed against host antigens – Hypersensitivity -- inappropriate or exaggerated response 19
 – Vitamin &")
Nutritional deficiency and imbalances – Protein-calorie deficiencies – Protein-calorie excess (obesity) – Vitamin & mineral imbalances 20

Workload imbalance – Overworked or under worked cells 21

GENETIC DERANGEMENTS Cancer Down's Syndrome Ehlers-Danlos

Free radicals • Free radicals are chemical species with a single unpaired electron in an outer orbital • Free radicals are chemically unstable and therefore readily react with other molecules, resulting in chemical damage • Free radicals initiate autocatalytic reactions; molecules that react with free radicals are in turn converted to free radicals 23

Reactive oxygen species: • Superoxide anion • Hydroxyl radical • Hydrogen peroxide 24

Free radicals initiated by: EXOGENOUS SOURCES: • Radiant energy: UV, X ray 25

Free radicals initiated by: • • • ENDOGENOUS SOURCES: Inflammation: e. g. neutrophil killing Chemicals/drugs &their metabolism Redox reactions of normal metabolism Transition metals: especially iron & copper, which donate or accept free electrons • Nitric oxide (just say NO!) 26

CELL INJURY BY FREE RADICALS • Lipid peroxidation of membranes • Oxidative modification of proteins • DNA Lesions 27

Protection from ROS Antioxidants block or scavenge • Vits. A, E, C • Binding of catalyzing iron & copper to transport proteins (e. g. transferrin, ceruloplasmin, lactoferrin, ferritin) • Enzymes: • Catalase (in peroxisomes) decomposes hydrogen peroxide • Superoxide dismutase converts superoxide to water and oxygen • Glutathione peroxidase catalyzes free radical breakdown 28

DISEASES CONGENITAL – genetic, non genetic ACQUIRED – • Infective • Inflammatory – injury & disordered repair • Immune • Metabolic • Hemodynamic • Cell growth 29

Others • Iatrogenic • Opportunistic • Hospital acquired infections 30

PATHOGENESIS 31

The cellular response depends on: • Type of lesion • Duration and severity • Type of cell • Physiologic state of the cell • Capacity of the cell for adaptation 32

Type, duration & severity of the injurious agent small dose of chemical toxin or short duration of ischemia cause reversible cell injury, while large dose of the same chemical agent or persistent ischemia causes cell death.

Type, status & adaptability of the target cell n nutritional and metabolic status, & adaptation of cell to a hostile environment determine the extent of cell injury skeletal muscles can withstand hypoxic injury for a longer time while cardiac muscles often suffer irreversible cell injury after 30 -60 min of persistent ischemia.

Important susceptible cell components • Generation of ATP by aerobic respiration. • Integrity of the cell membrane (ionic & osmotic homeostasis) • Protein synthesis • Cytoskeleton • Genetic integrity 35

Cellular and biochemical sites of damage in cell injury • ATP decrease • Mitochondrial damage • Loss of calcium homeostasis • Oxidative stress 36

cell injury ATP is essential for Membrane transport, Protein synthesis, Lipid synthesis Phospholipid metabolism

Consequences of ↓ intracellular ATP • Plasma membrane sodium pump failure • Calcium influx • Altered energy metabolism • Reduction in protein synthesis • Unfolded protein response 38

HYPOXIA - ISCHEMIA MODEL Blood Clot O 2 Impaired function of the plasma membrane ATP-dependent Na+ pump Oxidative ATP Phosphorylation Glycolysis Detachment of ribosomes

SEQUENTIAL CHANGES Failure of aerobic &switch to anaerobic respiration Rapid depletion of glycogen accumulation of lactic acid lowers the intracellular p. H Intracellular acidosis-clumping of nuclear chromatin

Normally in the ATP dependent Na+-K+ pump there is transport of Na+ out of the cell and diffusion of K+ into the cell lowered ATP Na+ is retained within the cell K+ is diffused out of the cell This results in increased intracellular water accumulation to maintain the iso-osmatic condition (hydropic swelling)

As a result of continued hypoxia Ribosomes are detached from the granular endoplasmic reticulum Polysomes are reduced to monosomes Thus reduced protein synthesis

Ca++ INDUCED CELL INJURY Ca++ Cytoplasmic ionic Ca++ ATPase ATP Phospholipase Phospholipids Protease Protein Endonuclease DNA Disruption Damage

Mitochondrial Damage by: • Cytosolic Calcium influx • Oxidative stress • Phospholipase - breakdown of phospholipids - and sphingomyelin pathways 44

Mitochondrial damage results in • Mitochondrial permeability transition of inner mitochondrial membrane • Reversible but can become permanent and be death blow • Leakage of cytochrome c and initiation of apoptosis 45

Membrane permeability defects result in • Mitochondrial dysfunction • Loss of membrane phospholipids • Cytoskeletal abnormalities • ROS (reactive oxygen species) • Lipid breakdown products 46

Lysosomal membrane injury: Enzyme leakage and activation in cytoplasm →cell digestion, loss of glycogen, loss of RNA & DNA and eventually necrosis 47

Cell Injury and Cell Death • Point of no return: not precise • Two consistent characteristics of irreversibility 1. Inability to restore mitochondrial function 2. Severe cell membrane damage • Leak of lysosomal contents leading to cytoplasmic & nuclear degradation • Massive leak of intracellular substances and influx of calcium 48

CELLDEATH • NECROSIS • APOPTOSIS 49

50
- Slides: 50