Pathology of Kidney Dr Sachin Kale MD Associate








 • TUBULAR INJURY (NEPHROTOXIC)")
 – Mild OLIGURIA – Mild AZOTEMIA • MAINTENANCE")






: 1 -4 weeks following streptococcal infection by nephritogenic strains")







,")















- Slides: 43
Pathology of Kidney Dr. Sachin Kale, MD. Associate Professor, Dept of Pathology.
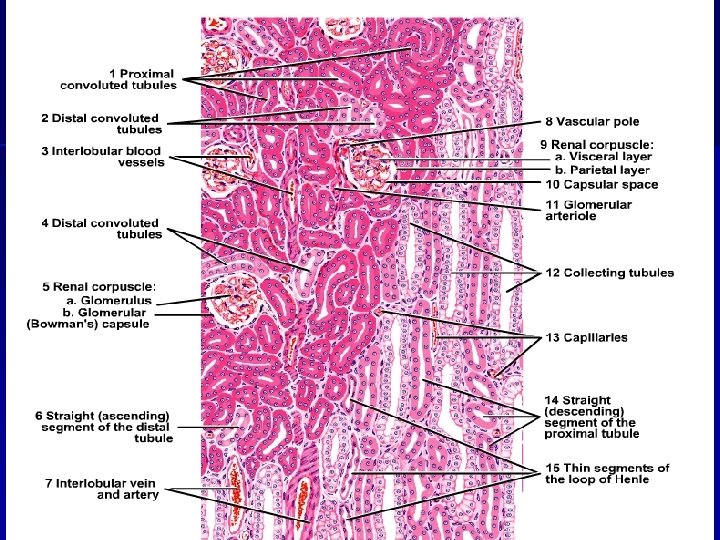
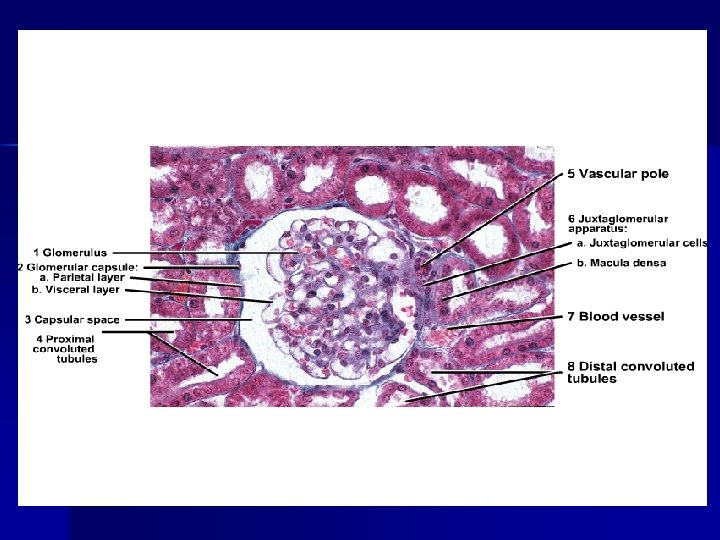
Anatomy of Kidney Note the positions of Glomerulus PCT, DCT, CT Cortex, Medulla, Pelvis.
Glomerular diseases: n Primary – Acute diffuse post streptococcal – RPGN – Membranous GN – FSGS – MPGN – Lipoid nephrosis or minimal change – Ig. A nephropathy n Secondary – SLE, Diabetes, Amyloidosis, Goodpasture’s syndrome, PAN, WG, HSP, Hypertension etc.
Clinical Syndromes: n Nephritic syndrome. – Oliguria, Haematuria, Proteinuria, Oedema, Azotemmia, Hypertension. n Nephrotic syndrome. – >3. 5 gm proteinuria, Hypoalbuminemia hyperlipidemia, Lipiduria n RPGN. – Nephritis, loss of Kidney function - within weeks n Chronic renal failure. – Azotemia/uremia progressing over months and years q Asymptomatic Hematuria or proteinuria
CHRONIC RENAL FAILURE Fluid and Electrolytes: Dehydration, Edema, Hyperkalemia, Metabolic acidosis Calcium Phosphate and Bone: Hyperphosphatemia, Hypocalcemia, Secondary hyperparathyroidism, Renal osteodystrophy Hematologic: Anemia, Bleeding diathesis Cardiopulmonary: Hypertension, Congestive heart failure, Pulmonary edema, Uremic pericarditis Gastrointestinal: Nausea and vomiting, Bleeding, Esophagitis, gastritis, colitis Neuromuscular: Myopathy, Peripheral neuropathy, Encephalopathy Dermatologic: Sallow (greenish-yellow) color, Pruritus, Dermatitis
ACUTE TUBULAR NECROSIS • • Destruction of renal TUBULAR epithelium Loss of renal function 50% of ACUTE renal failure Two types: ISCHEMIC NEPHROTOXIC -AMINOGLYCOSIDES -AMPHOTERICIN B -CONTRAST AGENTS
NORMAL
ATN
ATN PATHOGENESIS • BLOOD FLOW DISTURBANCES (ISCHEMIC) • TUBULAR INJURY (NEPHROTOXIC)
CLINICAL COURSE • INITIATION (36 hours) – Mild OLIGURIA – Mild AZOTEMIA • MAINTENANCE – More OLIGURIA – More AZOTEMIA – DIALYSIS NEEDED • RECOVERY – HYPOKALEMIA main problem – BUN, CREATININE return to normal
Immune Mechanisms of Glomerular injury: n Antibody mediated: In-Situ immune complex deposition n Circulating immune complex deposition. n n n – Tissue antigens - Goodpasture anti GBM Ag – Planted antigens - infections, toxins, drugs. – – Endogenous - DNA as in SLE Exogenous – infections – HBs. Ag, Syphilis, Streptococcal, Falciparum, Cell mediated Immune injury Activation of alternate complement pathway
Immune Glomerulonephritis: 1. 2. 3. 4. 5. 6. Antigen or Antibody - Immune reaction Activation of complements, Neutrophils… destruction of glomerular structure Inflammation, exudation swelling. ↓ blood flow, GFR, Oliguria, Proteinuria, Hematuria, Hypertension.
Neutrophil Activity Proteases – GBM degradation n Reactive oxygen metabolites – cell damage n Arachidonic acid metabolites – Reduction in GFR n
Other Mediators Cytotoxic antibodies n Macrophages n Platelets n Resident glomerular cells n Fibrin related products n
Nephritic Syndromes : n Diffuse Proliferative GN – Post Streptococcal. n Rapidly Progressive GN (or Crescentic) – Post Streptococcal, Goodpasture’s, n Focal Glomerulonephritis – Primary: Bergers disease (Ig. A Nephritis) – Secondary Ig. A nephritis, Henoch Schonlein purpura, SBE, Coeliac Disease etc.
Diffuse Proliferative GN: Post streptococcal* common – n Primary infection - Pharynx, skin, ear etc. . n Kidney damage – 1 -4 weeks after infection. n Malaise, fever, nausea, edema*, ↑ASO, ↓C 3 n Resolution in 6 -8 weeks. n
Post Streptococcal GN (Prol. GN): 1 -4 weeks following streptococcal infection by nephritogenic strains (time for Ab formation) n Immune mediated n Granular deposits of Ig. G, Ig. M & C 3 in GBM, (subepithelial location common) n Humps in GBM on EM or IF Microscopy n
• Normal • Inflammation • Proliferation • Swelling. • Narrow capillary • ↓GFR-Renin-BP • Post Strepto GN
Diffuse Proliferative GN: n n Enlarged hypercellular glomeruli. Hyperplasia of epithelium & endothelium. Cell Swelling. Inflammatory cells. Collapsed capillaries. Obstruction to blood flow.
IF- Diffuse Proliferative GN
Pathogenesis of Diffuse PGN: Streptococcal infection – Antibody attack GBM - inflammation & proliferation. n Glomerular capillary obstruction: n – J. G. A stimulation – Renin – high blood pressure – Reduced filtration – raised blood urea – Fluid retention – Oedema n Damage to GBM: – Unselective proteinuria (form Pr. casts in tubule) – Haematuria (form RBC casts in tubule)
Progression of DPGN: Poststreptococ cal DPGN Rapidly Progressive GN Complete Healing CGN Cardiac Failure or Uremia; death in acute phase
RPGN Clinicopathologic syndrome n Glomerular damage n Rapid progressive decline in renal function n Histology: accumulation of cells in Bowman’s space in the form of “Crescents” n
RPGN: Classification & Pathogenesis Postinfectious n GN associated with systemic diseases n Idiopathic RPGN n Glomerular injury is immunologically mediated. n Goodpasture’s syndrome – classic anti. GBM nephritis n
RPGN classification Post-infectious RPGN n Systemic diseases – n – SLE, Goodpasture’s, Vasculitis (PAN), Wegener’s granulomatosus, HSP, Essential cryoglobulinemia n Idiopathic RPGN
RPGN cont. . Idiopathic : ½ the cases, n Linear, Granular or minimal to none immune deposits n Gross: Enlarged pale kidneys Large white kidney n Petechial hemorrhages in cortex n M/E: Glomeruli: focal necrosis, endothelial proliferation n
RPGN… Formation of crescents: n Proliferation of parietal cells, migration of monocytes and macrophages into Bowman’s space n Crescents obliterate Bowman’s space, compression capillary tuft n Crescents undergo sclerosis n
RPGN: Clinical features Goodpasture’s Syndrome: recurrent hemoptasis & renal manifestations n Hematuria, Red cell casts, Moderate proteinuria, n Variable HT and edema n Oliguria n
Which of the following presents with hematuria, proteinuria and hypertension Nephrotic syndrome n Nephritic Syndrome n UTI n Renal Tubular Acidosis n
All of the following are seen in renal failure except Hypercalcemia n Hyperkalemia n Bone lesions n Metobolic Acidosis n
Anemia in renal failure is generally Microcytic hypochromic n Normocytic normochromic n Dimorphic n megaloblastic n
Which of the following is not a primary GN Minimal Change disease n Membranous GN n Diabetes mellitus n RPGN n
Which of the following is not part of nephrotic syndrome Lipiduria n Hypertension n Proteinuria n Edema n
True about Post-strepto GN Occurs 1 – 4 months after infection n Occurs 1 – 4 days after infection n Occurs 1 – 4 weeks after infection n Non of the above n
False about RPGN. . Formation of crescents n Small contracted kidneys n Hematuria n Oliguria n
Spot the diagnosis RPGN
Spot the diagnosis ATN
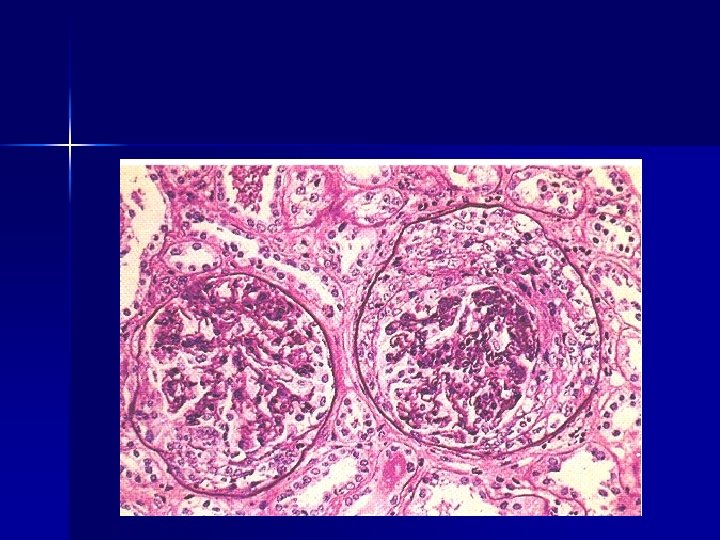
Spot the diagnosis Post streptoco ccal GN
Thought for the day… n Ours is a world where people don't know what they want and are willing to go through hell to get it.
Thanks… n http: //sachinkale 1. tripod. com