Pathology of atherosclerosis a concept building and case

Pathology of atherosclerosis - a concept building and case based approach Dr ajit nambiar
 and “sclerosis” ATHEROSCLEROSIS")
Understand two words “athero” (greek) and “sclerosis” ATHEROSCLEROSIS

Today’s journey Normal blood vessel Modifiable Non Modifiable Risk factors Years But every day you contribute to that build up A blood vessel with fat deposited in it’s wall

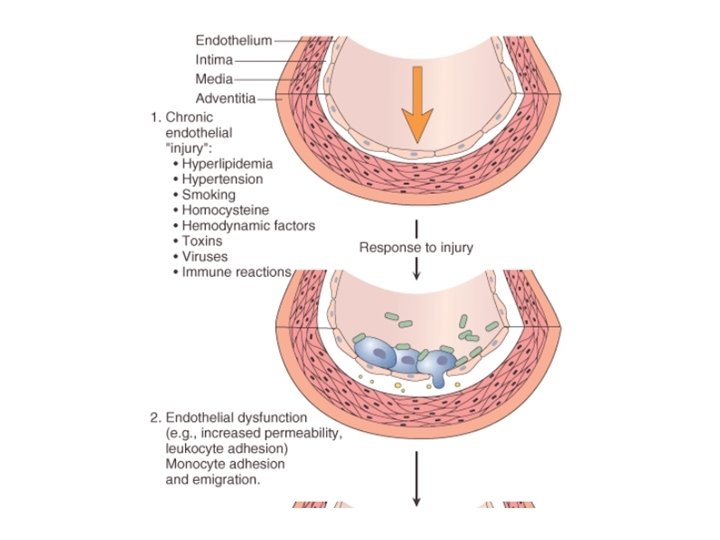
atherosclerosis is a chronic inflammatory and healing response RESPONSE TO INJURY HYPOTHESIS

Basic Concept 1 • injury inflammation Acute chronic Loss necrosis repair regeneration

Basic Concept 2 Cell injury inflammation chronic Chemical mediator CYTOKINES interleukins FUNCTIONS v. Activate endothelium v. Endothelial dysfunction v. Stimulate growth factors release v. Proliferation of fibroblasts and muscle cells

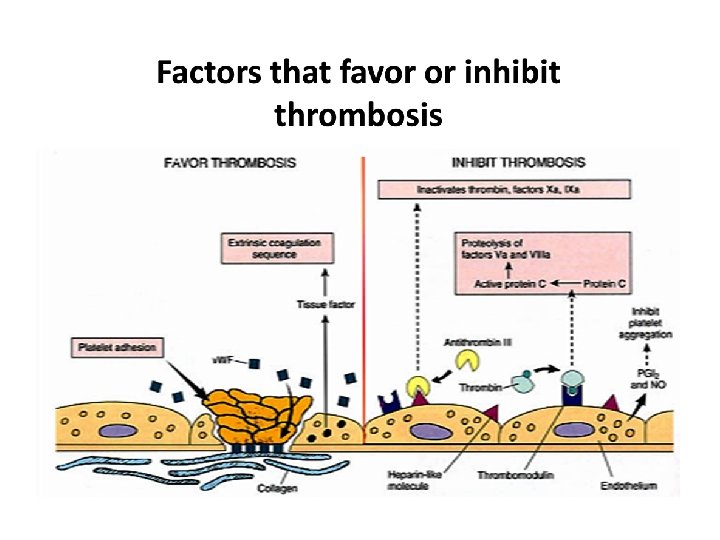
Basic Concept 3 Virchow’s triad
 chemokines")
Concept 4 Endothelial function and dysfunction Growth factors: FGF Inflammation: Cytokines(IL 1) chemokines

Cholesterol concept

Risk factors for atherosclerosis MODIFIABLE • • • Diabetes Hypertension Smoking Type A personality Obesity Metabolic syndrome NON- MODIFIABLE Age : elderly Sex : males , females after menopause Familial : hypercholesterolemia • Genetic: LDL receptor mutation • •

Major Risk Factors for Atherosclerosis NONMODIFIABLE Ø Increasing age Ø gender Ø Family history Ø Genetic abnormalities • rise with each decade • Males> females, • After menopause : the incidence of atherosclerosis increases • Familial hypercholesterolemia • Lipoprotein lipase deficiency (autosomal recessive) • Enzymes , LDL receptor (protein mutations)

MODIFIABLE Ø Hypertension Ø Cigarette smoking Ø Diabetes Ø Hyperlipidemia • cause endothelial cell injury • (1) increased glycosylation of collagen, which increases LDL binding to collagen in atheromatous lesions; and (2) the fact that glycosylated highdensity lipoprotein (HDL) is more easily degraded than is normal HDL. • Diet, cholesterol levels, LDL, HDL

HT DM smoking Endothelium injury/ dysfunction Increase permeability endothelium Loss of endothelium thrombosis Injury Inflammation chronic recruit Lymphocytes macrophages Release cytokines Growth factors: PDGF, FGF, TGF Lipid can enter intima Oxidized LDL is toxic to endothelium cholesterol Foam cells Lipid core Proliferation of smooth muscle fibrous tissue ATHEROSCLEROSIS

Definition of atherosclerosis • What Is getting deposited? • Where is it getting deposited? ? • Which vessels? ? • What Is atheros? ? ? • Why Is it thick? ? ? Or what Is sclerosis!!!
 Ø Coronary arteries, popliteal arteries,")
Atherosclerosis : Common sites Ø Lower abdominal aorta (Commonest) Ø Coronary arteries, popliteal arteries, internal carotid arteries Ø circle of Willis (cerebral vessels) Ø mesenteric and renal arteries, mainly at their origin (branching from aorta) Ø Vessels usually spared : upper extremities

Case studies Presentaion salient features Case 1 Case 2 Name age Ahmed 44 yr old Faisal 57 yr old presents He comes with history of chest pain. He feels his frequency and severity of pain is on an increase. He complains of severe chest pain and breathlessness with sweating Past history He complained of pain on exertion after doing heavy exercise since last 7 years. He is a known HT. He complained of pain on exertion after doing heavy exercise since last 12 years. He is a known HT, DM. Investigation His cholesterol levels are mildly elevated. Troponin and CK-MB normal Cholesterol moderately elevated. Troponin and CK-MB elavated

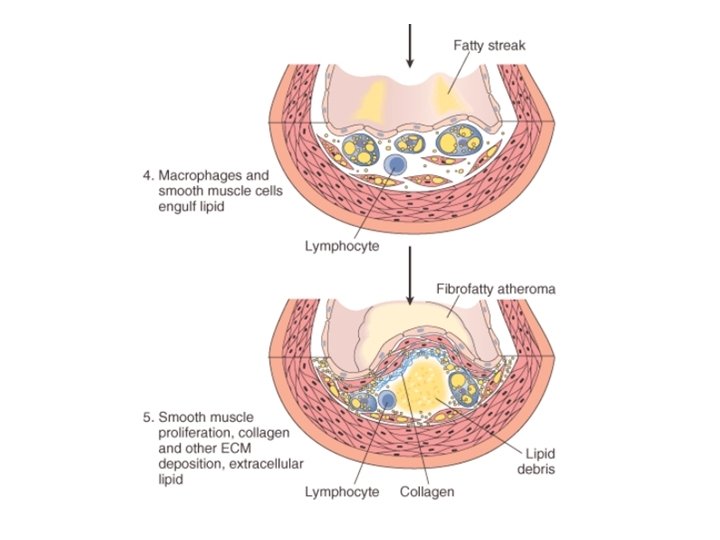
Atherosclerosis : Morphology • Stages of Atherosclerosis : 1. Fatty streaks and dots 2. Fibrous plaque / Fibrofatty plaque (Atheromatous plaque) 3. Complicated atheromatous plaque

Fatty streak
 A fibrous cap dense collagen and scattered smooth")
Atheromatous plaque 3 zones • (1) A fibrous cap dense collagen and scattered smooth muscle cells and macrophages; • (2) the lipid zone foam cells (lipid-laden macrophages and smooth muscle cells) and extracellular lipid and debris; • (3) the basal zone, composed of proliferated smooth muscle cells and connective tissue. Different plaques contain varying amounts of these three layers; some are mainly fibrous, and others are predominantly fatty.

Atherosclerosis : Morphology This microscopic cross section of the aorta shows a large overlying atheroma on the top with some ulceration on left. Needle-shaped cholesterol crystals are commonly present in the lipid zone

Atherosclerosis : pathogenesis of clinical complications The natural history, morphologic features, main pathogenic events, and clinical complications of atherosclerosis.

Complications in Atherosclerotic plaques BREAKAGE BLOCKAGE • Rupture and hemorrhage • Hemorrhage into a plaque (sudden blockage of lumen) • Aneurysm formation and potential rupture • Dissection (tear) in vessel wall and rupture • Ulceration (erosion) of the intima • Thrombosis Partially or completely occlude Lumen • Embolism (thrombus breaks dislodges in distant vessel away from origin) • calcification
 plaques q Vulnerable plaques : contain large areas of foam cells and extracellular")
Vulnerable(dangerous) plaques q Vulnerable plaques : contain large areas of foam cells and extracellular lipid, thin fibrous cap, contain few smooth muscle cells or have clusters of inflammatory cells, hence are more likely to rupture Vulnerable plaques (prone to rupture) have thin fibrous caps, large lipid cores, and increased inflammation Stable plaques - densely collagenous and thickened fibrous caps with minimal inflammation & little lipid core

CONSEQUENCES OF ATHEROSCLEROTIC DISEASE q. The major targets of atherosclerosis v. Heart (Myocardial infarction : Heart attack) v. Brain (cerebral infarction : stroke) v. Kidneys ischemia infarction vmesenteric occlusion and bowel ischemia, v. Lower extremities (peripheral vascular disease : gangrene of the legs) v. Aorta (aortic aneurysms)

Complications story of case 1 and case 2

Case diagnosis Case 1 • Angina pectoris • Angiogram shows 70% block in the left main anterior descending • A fibrous plaque • The progression of the plaque explains his worsening situation Case 2 • Myocardial infarction • ECG and cardiac enzymes are supportive • Complicated plaque • Vulnerable plaque • Complete block explains his myocardial infarction

Take home messages • Understand who are at risk and why? ? • How does a atheromatous plaque form (response to injury- chronic inflammation) • Where(locations) and what (constituent) of atheroma • Complications in atherosclerosis • Applying to clinical scenarios

Source Robbins Basic Pathology chapter 9 and page 336 - 344 THANK U FRIENDS
- Slides: 31