Pathogenesis of bone destruction Dr Salem Manasra Inflammation

Pathogenesis of bone destruction Dr. Salem Manasra

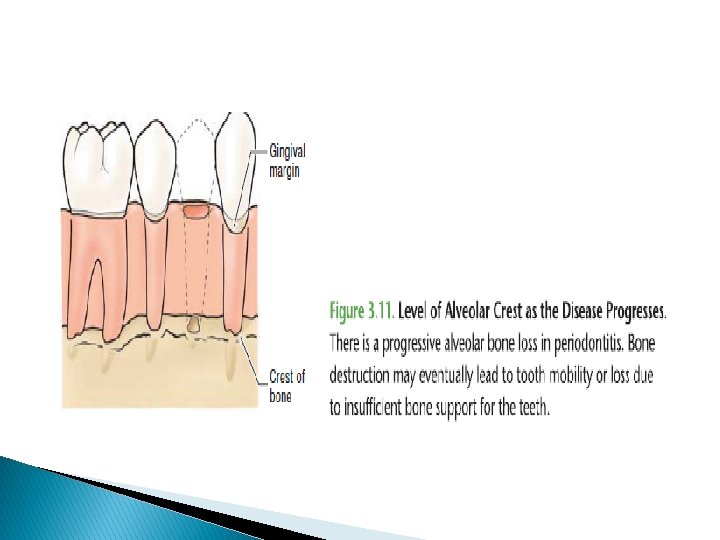
Inflammation : it’s the body reaction to injury. Alveolar bone loss : it’s the resorpion of alveolar bone as a result of periodontitis.

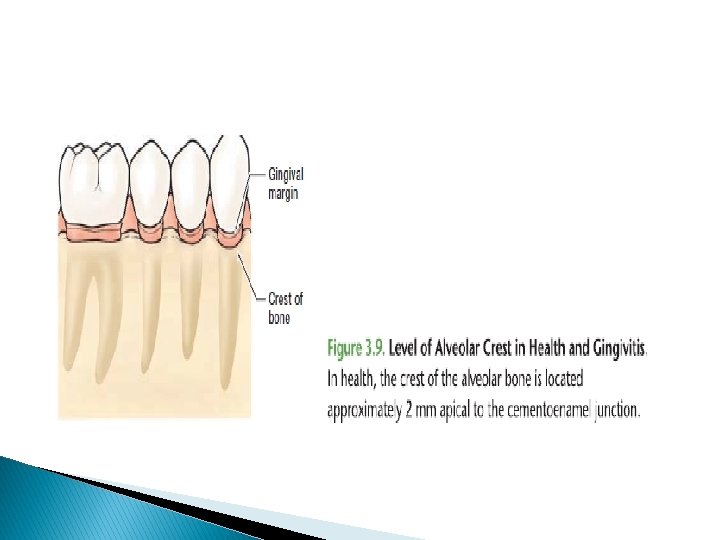
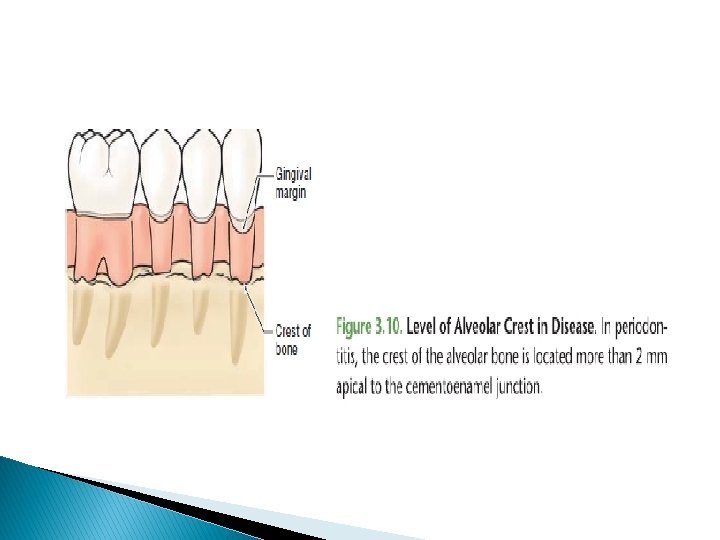
Changes in alveolar bone height in disease : Bone height in Health & Gengivitis , the crest of alveolar bone is located 2 mm apical ( below) the CEJ of the teeth. a. b. Bone height in periodotitis , more than > 2 mm.

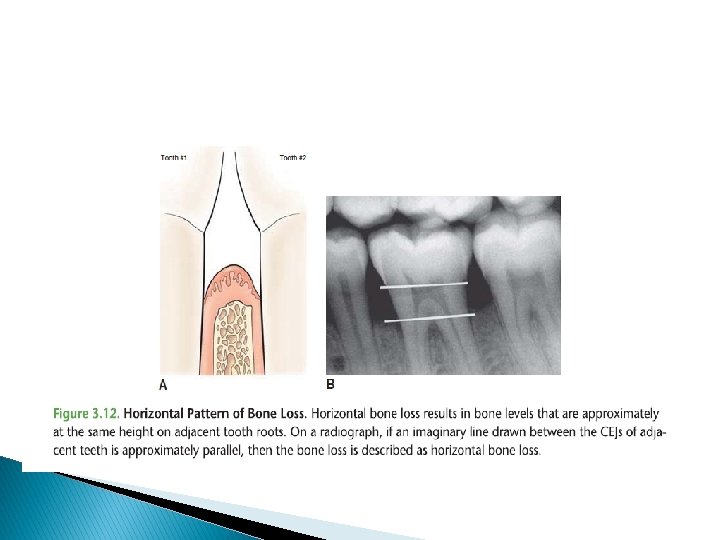
Types of bone loss : Horizontal bone loss : Is the most common of bone loss. This type of loss results in Even reduction of bone. 1.

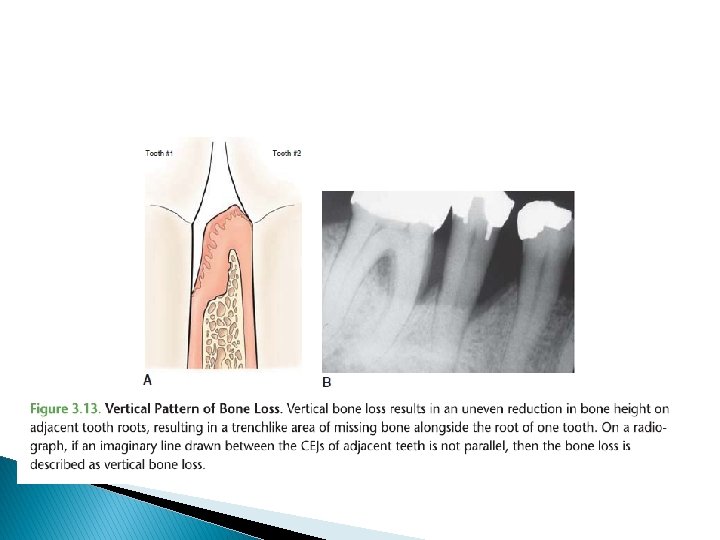
2. Vertical bone loss: Is less common of bone loss. This type of bone loss is Uneven reduction in the bone. 3. Combination of horizontal & vertical bone loss.

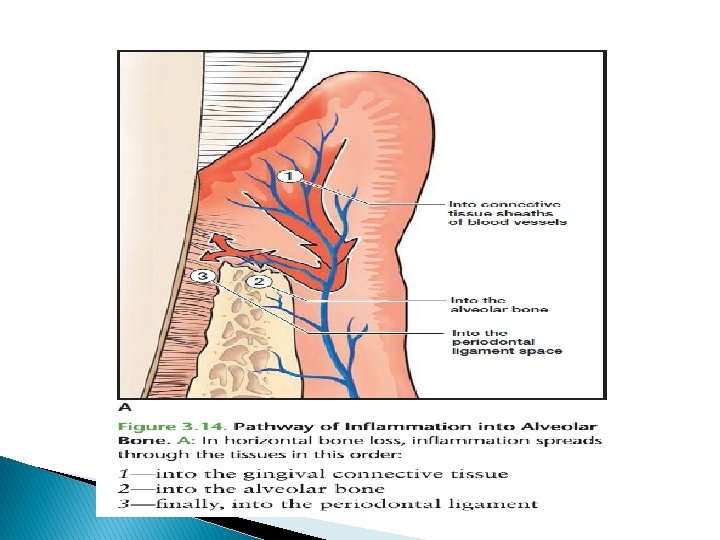
Pathways of inflammation into alveolar bone In Horizontal bone loss : 1 - inflammation spreads into the tissues within the gingival C. T along the C. T sheath surrounding blood vessels. 2 - into alveolar bone. 3 - into PDL space.

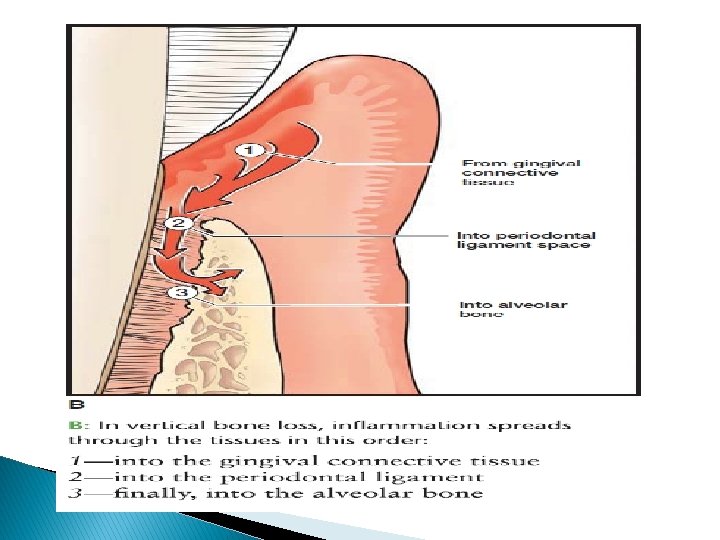
In Vertical bone loss : 1 - within gingival C. T. 2 - directly into PDL. 3 - into alveolar bone.

Bone defects in periodontal disease : we have three shapes of bone defects : a) Infra bony defects. b) Osseous craters. c) Bone loss in furcation area.
 Infra bony defects Result when bone resorption occurs in an uneven , oblique")
a) Infra bony defects Result when bone resorption occurs in an uneven , oblique direction. The bone resorption primarily affects on one tooth.
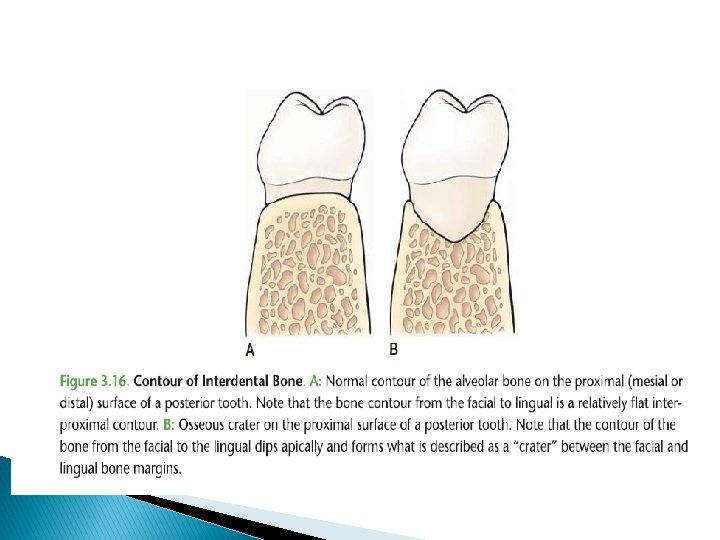
 Osseous craters : Is a bowel – shaped defect in the interdental alveolar")
b) Osseous craters : Is a bowel – shaped defect in the interdental alveolar bone. Bone loss nearly equal on the roots of two adjacent teeth.
 Bone loss in furcation area : Occurs in multi rooted tooth , resulting")
c) Bone loss in furcation area : Occurs in multi rooted tooth , resulting in a loss of alveolar bone between the roots of the teeth.

Periodontal pockets Attachment loss in periodontal pockets: It’s the destruction of the fibers & bone that support the teeth. Tissue destruction spreads not only ia an apical ( vertical ) directions, but also in lateral direction. A pocket on different root surfaces of the same tooth can have different depth.

Disease site : Is an area of tissue destruction. It may involve only single surface or several surfaces of the tooth. Inactive disease site : disease site is stable , with attachment level of JE remaining the same over time. Active site : that shows continued apical migration of JE over time.

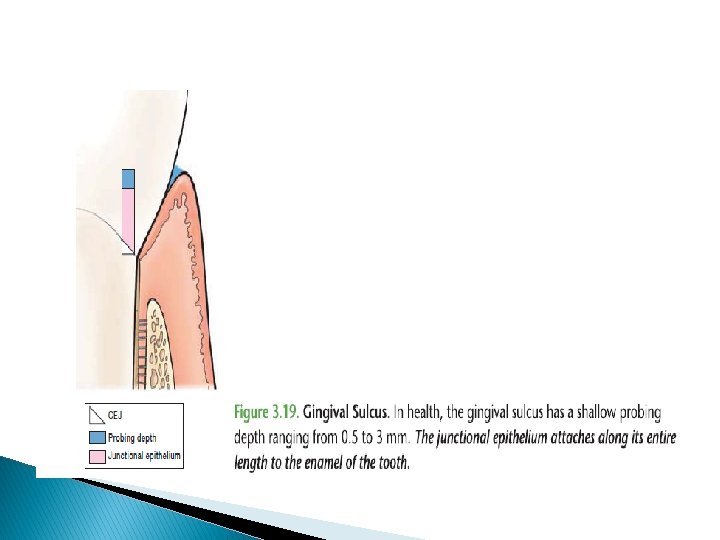
Pocket formation Gingival sulcus : In health , he sulcus is between 0. 5 – 3 mm in depth. The JE is coronal to CEJ & attach a long its length to the enamel of the tooth.

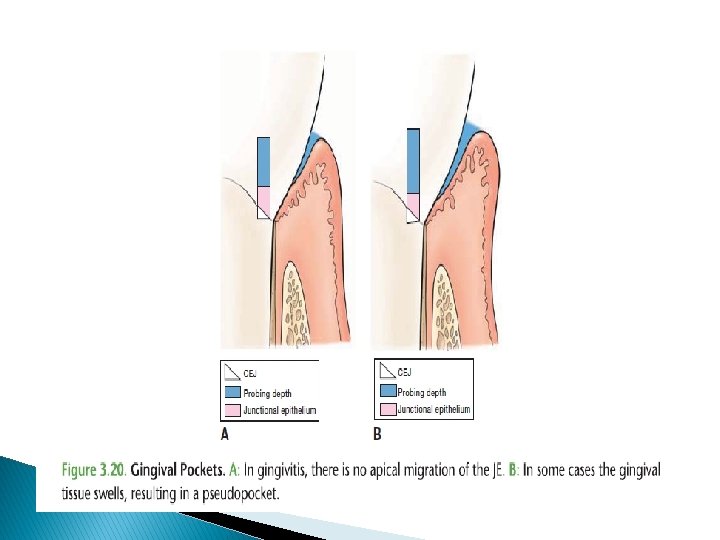
1. Gingival pockets Gingival pocket is a deepening of the gingival sulcus as a result of swelling or enlargement of the gingival tissue.

Characterized by : 1 - False pocket or ‘ psudopocket ‘ , because there is No destruction of PDL fibers or alveolar bone in a gingival pocket. 2 - No apical migration of JE in a gingival pocket , the JE remain coronal to CEJ. In gengivitis , the coronal portion of JE detaches from the tooth resulting in a slight increase in probing depths.
 Detachment of coronal portion of")
3 - increased probing depths. It occur because a) Detachment of coronal portion of CEJ from the tooth. b) Increased tissue size due to swelling of tissue & increase the collagen fibers in C. T.
- Slides: 27