Patellofemoral Stabilization Q angle RIMT University Department of
 RIMT University Department of Physiotherapy Prepared by: Dr. Navkaran Singh")
Patellofemoral Stabilization (Q- angle) RIMT University Department of Physiotherapy Prepared by: Dr. Navkaran Singh

Asymmetry of Patellofemoral Stabilization • The orientation of the quadriceps resultant pull with respect to the pull of the patellar tendon provides information about the net force on the patella in the frontal plane. • The NET EFFECT of the pull of the quadriceps and the patellar ligament can be assessed clinically using a measurement called the Q-angle (quadriceps angle).

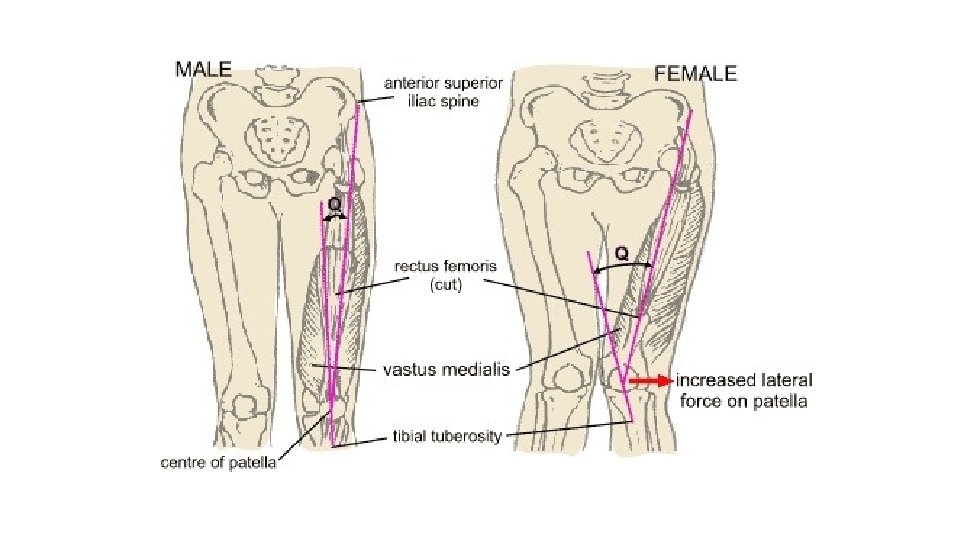
• The Q-angle is the angle formed between a line connecting the ASIS to the midpoint of the patella and a line connecting the tibial tuberosity and the midpoint of the patella. • A Q-angle of 10 degree to 15 degree measured with the knee either in full extension or slightly flexed is considered normal. • Any alteration in alignment that increases the Q-angle is thought to increase the lateral force on the patella.

Consequences of or in Q angle • This can be harmful because an increase in this lateral force may increase the compression of the lateral patella on the lateral lip of the femoral sulcus. • In the presence of a large enough lateral force, the patella may actually sublux or dislocate over the femoral sulcus when the quadriceps muscle is activated on an extended knee.

Why Q angle is measured in extension ? 1. The Q-angle is usually measured with the knee at or near full extension because lateral forces on the patella may be more of a problem in these circumstances. 2. With the knee flexed, the patella is set within the intercondylar notch, and even a very large lateral force on the patella is unlikely to result in dislocation. 3. Furthermore, the Q- angle will reduce with knee flexion as the tibia rotates medially in relation to the femur.

Men vs Women • It has been postulated that women have a slightly greater Q-angle than do men because of the presence of a wider pelvis, increased femoral anteversion, and a relative knee valgus angle. • However, other authors have disputed this, and the presence of a gender difference in the Q-angle is still a matter of debate. • Although an excessively large Q-angle of 20 degree or more is usually an indicator of some structural malalignment, an apparently normal Q -angle will not necessarily ensure the absence of problems.

• Large Q-angles are thought to create excessive lateral forces on the patella that may predispose the patella to pathologic changes. IMPORTANT: • One problem with using the Q-angle as a measure of the lateral pull on the patella is that the line between the ASIS and the midpatella is only an estimate of the line of pull of the quadriceps and does not necessarily reflect the actual line of pull in the patient being examined.

1. If a substantial imbalance exists between the vastus medialis and vastus lateralis muscles in a patient, the Q-angle may lead to an incorrect estimate of the lateral force on the patella because the actual pull of the quadriceps muscle is no longer along the estimated line. 2. Furthermore, a patella that sits in an abnormal lateral position in the femoral sulcus because of imbalanced forces will yield a smaller Q-angle because the patella lies more in line with the ASIS and tibial tuberosity.

There are several abnormalities that can yield increased lateral forces. • There is a potential for imbalance between the vastus lateralis and vastus medialis muscles, although, as identified earlier, this imbalance cannot be measured in vivo. • The presence of a tight IT band could also limit the mobility of the patella and restrict its ability to shift medially during flexion, contributing to increased stress under the lateral facet of the patella. • When the IT band moves posteriorly with knee flexion, it exerts an even greater lateral pull on the patella, which results in a progressive lateral tilting as knee flexion increases. • The increased lateral tilt could further load the lateral facet, increasing joint stress. • The frontal plane deviation of GENU VALGUM increases the obliquity of the femur and, concomitantly, the obliquity of the pull of the quadriceps.
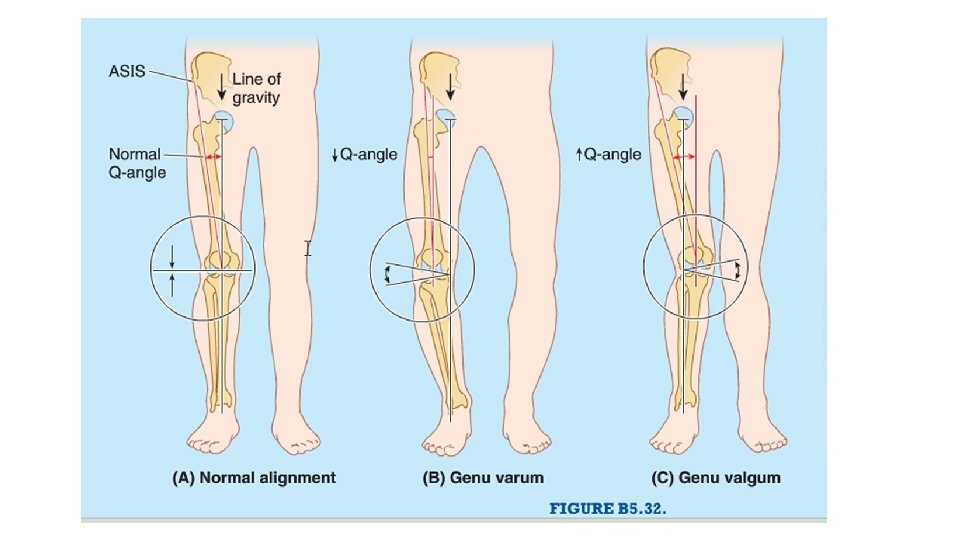

• In contrast, individuals with genu varum exhibit less obliquity of the femur and therefore should have a diminished lateral quadriceps pull. • The transverse plane deviation of medial femoral torsion (or femoral anteversion) generally results in the femoral condyles being turned in (medially rotated), carrying the patella medially with the femoral condyles and increasing the Q-angle by increasing the obliquity of the pull of the quadriceps on the patella. • Medial femoral torsion is often associated with lateral tibial torsion in the older child or adult, or it may exist independently.
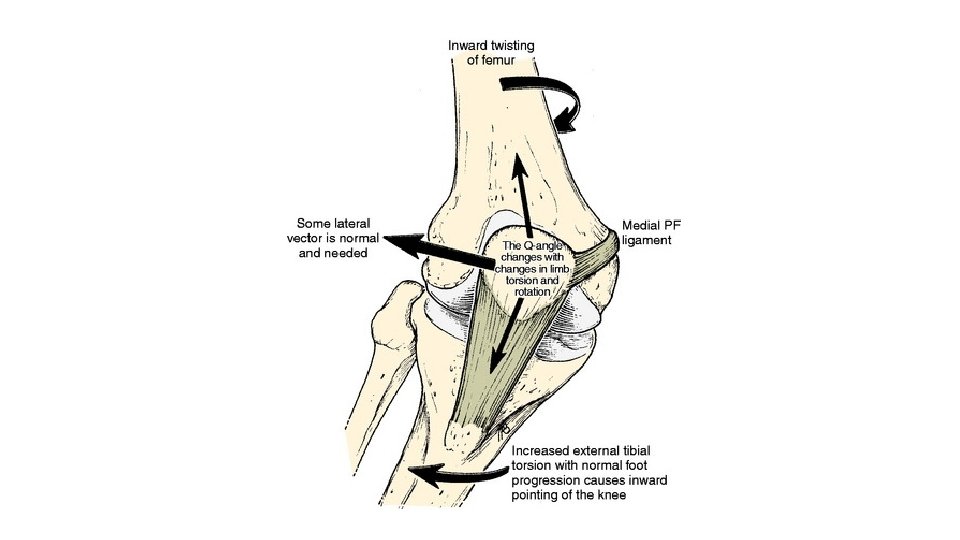

• In lateral tibial torsion, the tibial tuberosity lies more lateral to the patella, increasing the Q-angle by increasing the obliquity of the patellar tendon. • When medial femoral torsion and lateral tibial torsion coexist, the Q -angle will increase substantially, resulting in a substantial lateral force on the patella.

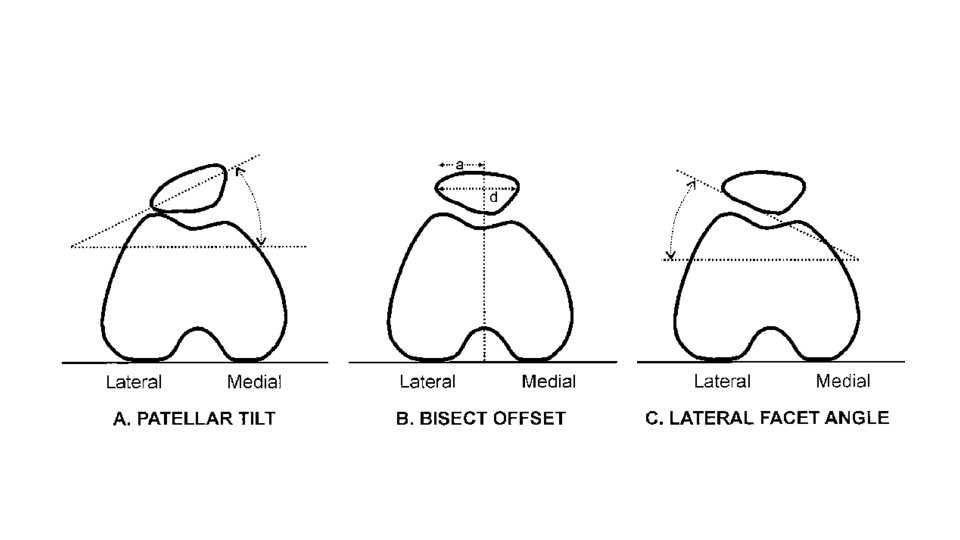
Forces other than the alignment and balance of the quadriceps muscle components may influence patellar positioning. 1. Either laxity of the medial retinaculum or excessive tension in or adaptive shortening of the lateral retinaculum may contribute to a laterally tilted patella in the femoral sulcus. 2. In addition, a tight IT band may exert an excessive lateral pull on the patella through the lateral patellofemoral ligament. 81 3. Such deficits in the passive stabilizers, as well as weak- ness in the medial active stabilizers, result in increased lateral compressive forces. 4. It is currently unknown whether such changes in the passive structures are primary or are secondary to abnormalities in the dynamic stabilizers.

Thank you
- Slides: 17