Partners in Health Rwanda There a total of







 Medication Costs Annual Per Patient Marginal Per Capita Program")













- Slides: 30
Partners in Health Rwanda
�There a total of 27 rural health districts �They include more than 80% of the population �Current annual per capita health care spending by public sector is around $4 ($40 million total) �Additional $15 per capita donated by PEPFAR ($150 million total) �Target for annual per capita health care spending is $27
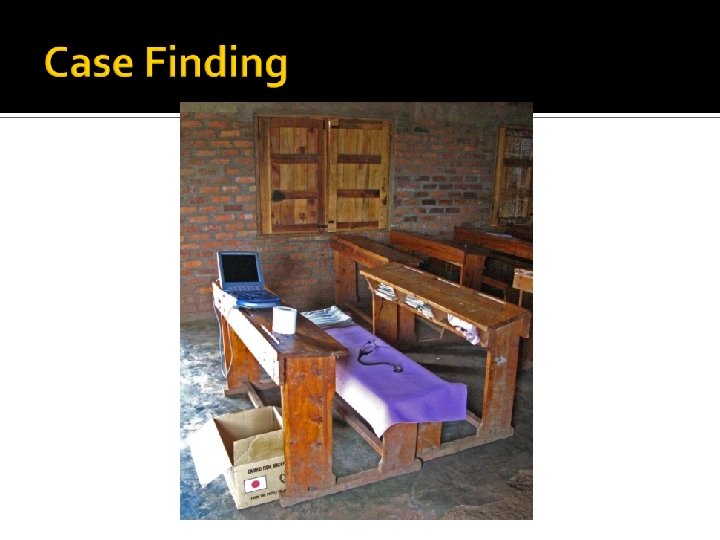
Burera Southern Kayonza Kirehe ● ● ● Health center Kigali District hospital + health center 1 hour good road + 30 minutes slow track
Haiti Rwanda S. Africa China France BP BMI CHOL Ezzati et al. PLo. S Medicine. 2005
Indicator Rural Urban Farmer 92 % 44 % % in lowest wealth quintile 24 % 6. 1% Dirt-floor housing 93 % 52 % % of women with BMI > 25 kg/m 2 10 % 19 % % of women with BMI < 18. 5 kg/m 2 20 % Cannot read at all 32 % 15 % No education 25 % 14 % No trained assistance during delivery 65 % 34 % Access to health care limited by facility distance (women’s self-report) 42 % 28 % Infant mortality (per 1000 live births) 108 69
N % of Heart Failure Admissions Authors Country City or Region D’Arbela et al. 1966 Uganda Kampala 15, 176 3. 5% Turner 1962 Tanzania Mombasa 3, 052 6% Baldachin 1962 Zimbabwe Bulawayo 12, 105 3% Nigeria Jos and Katsina 2, 700 7% Beet 1956
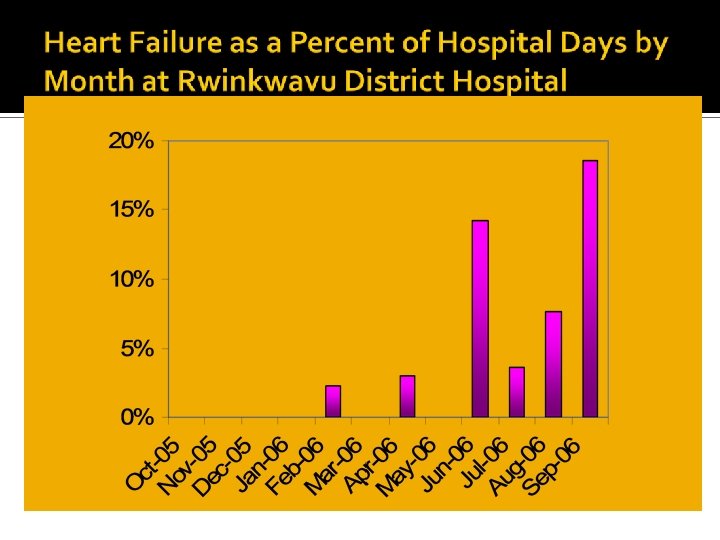
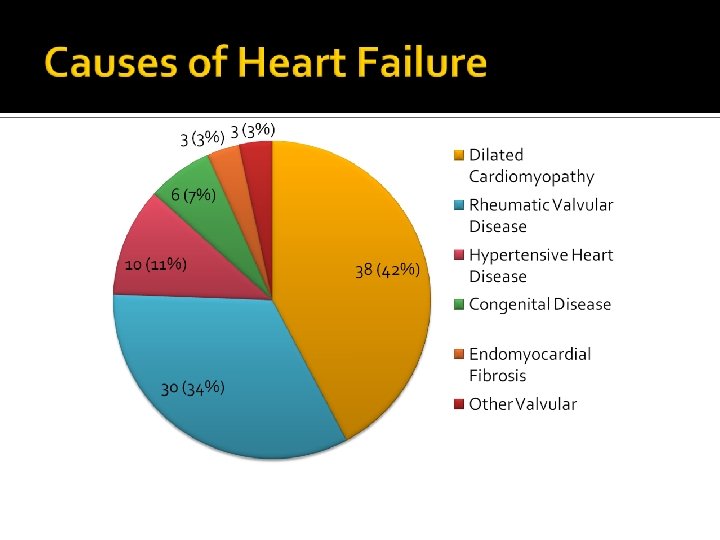
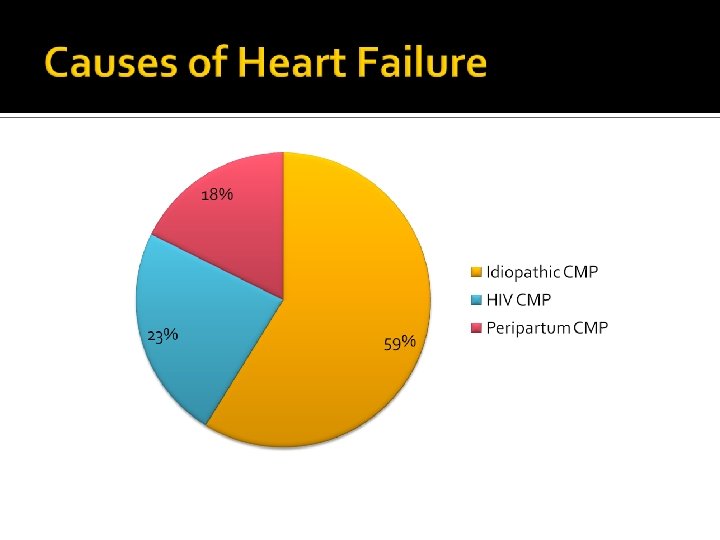
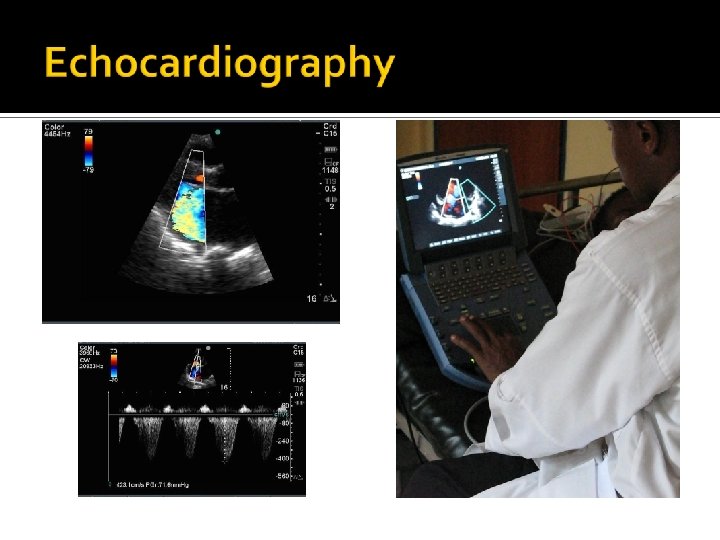
� 90 patients with heart failure identified from October 2006 to October 2007 �All have structural heart disease confirmed by echocardiography �Median age: 36 years
Disease Cardiomyopathy (0. 2% prevalence) Medication Costs Annual Per Patient Marginal Per Capita Program Cost $55 Advanced RHD (0. 1% prevalence) Malignant HTN (0. 3 % prevalence) Operative Costs Per Patient $0. 19 $5, 000 – 10, 000 $25 Total *Based on estimates of disease prevalence and intensity of case finding $0. 76 $0. 53 $1. 48*
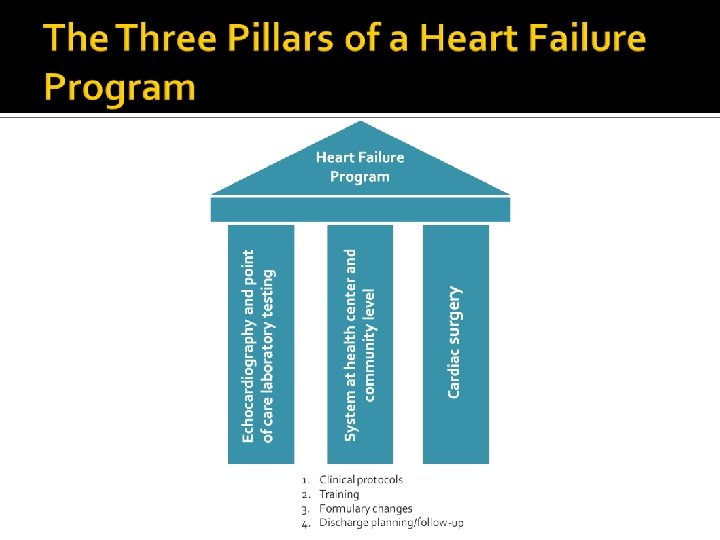
Physicians Nurses Physicians Community health workers Nurses and physicians Echocardiography Point of care laboratory testing Clinical protocols
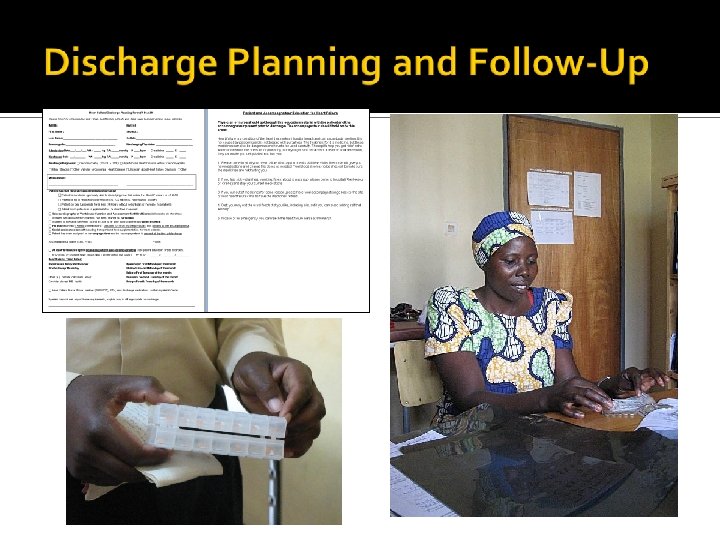
�I-STAT machine for monitoring of Renal function Electrolytes INR in case of anticoagulation
Clinical Protocols
Clinical Protocols
Medication Initial Estimate Final Estimate Captopril 37. 5 mg tid $22 $16 Lisinopril 20 mg qd $241 $12 Atenolol 50 mg qd $2 $2 $1261 $26 $1 $1 $805 $4 Carvedilol 25 mg bid HCTZ 12. 5 mg Amlodipine 10 mg qd www. imres. nl
Faris et al. Cochrane Collaboration. 2006 Mc. Murray and Pfeffer. Lancet. 2005
Stage IV hypertension almost eradicated
Prophylaxis 55 patients with Rheumatic MR treated with monthly IM benzathine PCN Tompkins et al. Circulation. 1972
Prophylaxis
�Walter Sisulu Heart Center, Johannesburg, South Africa �Emergency, Salam Heart Center, Khartoum �Operation Open Heart at King Faisal Hospital in Kigali �Brigham and Women’s Hospital at King Faisal Hospital
� How to scale-up a heart failure program at a national level? 1. 2. 3. 4. 5. 6. 7. Procurement of echocardiography equipment at district hospital level Procurement of point of care laboratory testing at district hospitals and health center level Formulary changes at district hospital and health center level Development and implementation of country-specific clinical protocols for district hospitals and rural health centers Development of training material and a training curriculum for physicians, nurses, and community health workers Development of a training model requiring 1 to 1 clinical mentorship and leading to official certification Partnership with Ministry of Health, National Medical School, and other stakeholders (i. e. Rwandan Heart Association)
� Why only heart failure? There is the need for a program targeting all chronic diseases of poverty 1. Edematous conditions 2. 3. 4. 5. 6. Insulin-dependent diabetes Severe hypertension Asthma and other chronic lung diseases Epilepsy Malarial hyper-reactive splenomegaly a) b) c) Heart failure Cirrhosis/portal hypertension Chronic renal disease We are currently working on the development of a chronic care team (2 physicians and 3 nurses)