Parenteral preparations Presented by Dr Fatma M Mady

Parenteral preparations Presented by Dr. Fatma M Mady

Formulations intended for use by injection under or through one or more layers of the skin or mucous membrane From the Greek word “pare-enteren” means “to avoid the intestines” These drugs administered directly into tissues, tissue spaces or compartments by injection or infusion.

Why Parenterals? To achieve a biological effect that is not possible for oral administration: e. g. Insulin, certain penicillins To deliver the drug when the oral route is not available: e. g. coma, seizures, uncooperative patients, intensive care, Psychatric To minimize or avoid systemic toxicity: e. g. methotrexate (leukemic patients) To achieve local effect: e. g. local anaesthetics (dentist), local antiinflammatory (joints)

To allow rapid correction of fluid and electrolyte imbalances, and to supply short or long term nutritional needs: e. g. severe dehydration or electrolyte depletion To achieve immediate effect in emergencies (life threatening): e. g. direct intraventricular route To ensure delivery of accurate concentration of the drug: e. g. i. v route To guarantee dosage and drug compliance: e. g. i. m. long acting penicillins (prophylaxis of rheumatic heart disease) Ø How we can achieve slow onset and prolonged drug action obtained by: Modifying the formulation. (ex. Suspension, nanoparticles…etc) Using a route of injection other than I. V.
 Incorrect drug")
Why not parenterals? The frequent pain and discomfort of injections (invasive route) Incorrect drug or dose is often harder or impossible to counteract (i. v. route) Risk of tissue toxicity from local irritation. Restriction to use in hospitals or with specialized personnel Require asepsis (absence of microorganisms) at administration.
 • Subcutaneous (S. C) • Intramuscular (I.")
Routes of Administration • Intravenous (I. V) • Subcutaneous (S. C) • Intramuscular (I. M) • Intra dermal (I. D) • Other parenteral routes.
")
Intravenous (I. V)

1. Intravenous Route ØIntravenous medication is injected directly into vein to Obtain rapid and predictable onset Avoid irritation of other tissues. ØOnly drugs in aqueous or hydro-alcoholic solutions can be given by the I. V route. ØThe most commonly used veins for I. V. administration are proximal veins that are located in the forearm. ØIntravenous injections range from 1 - 100 ml.
 Suitable for irritant drugs due to rapid dilution and")
Intravenous route (I. V. ) Suitable for irritant drugs due to rapid dilution and insensitivity of the venous wall. Correction is very difficult or impossible. Avoid too rapid drug administration because of the irritation and/or drug toxicity at the target organ (drug shock) ( 1 ml per 20 sec) Aqueous, o/w emulsions (droplet size control) w/o & suspensions must not be given. Volume: 0. 5 – 1000 ml bolus dose: up to 10 ml slow controlled rate: 10 -50 ml i. v. infusion: 50 -1000 ml

Venoclysis Ø Is a technique of using intravenous infusion of large volumes of fluids (100 -1000 ml) Ø It utilizes products known as large volume parenterals (LVPs). Ø LVPs are used to: a. Supply electrolytes and nutrients. b. Restore blood volume. c. Prevent tissue dehydration. d. Dilute toxic materials already present in the body fluids. Ø e. g. Sodium Chloride USP (0. 9%) Dextrose(5%) , Ringer.
 is the commonly-used term for a solution of 0. 91%")
Saline normal saline (NS) is the commonly-used term for a solution of 0. 91% w/v of Na. Cl this solution is referred to as physiological saline or isotonic saline NS is used frequently in intravenous drips (IVs) for patients who cannot take fluids orally and have developed or are in danger of developing dehydration or hypovolemia.

Lactated Ringer's solution is a compound that is isotonic with blood and intended for intravenous administration. Generally, the sodium, chloride, potassium and lactate come from Na. Cl (sodium chloride), Na. C 3 H 5 O 3 (sodium lactate), Ca. Cl 2 (calcium chloride), and KCl (potassium chloride). Lactated Ringer's Solution is used because the byproducts of lactate metabolism in the liver counteract acidosis, which is a chemical imbalance that occurs with acute fluid loss or renal failure.

Lactated Ringer's Solution is often used for fluid resuscitation after a blood loss due to trauma, surgery, or a burn injury. Previously, it was used to induce urine output in patients with renal failure. Lactated Ringer's Injection, USP is indicated as a source of water and electrolytes or as an alkalinizing agent. Lactated Ringer's Injection, USP produces a metabolic alkalinizing effect. Lactate ions are metabolized ultimately to carbon dioxide and water, which requires the consumption of hydrogen cations.

Human Albumin It is a sterile nonpyrogenic preparation of serum albumin. The solution contains 5 or 25 of albumin, corresponding to 100 or 500 ml of normal human plasma, respectively. Do not contain antimicrobial agent. It serves as an emergency agent for restoration of blood volume in case of shock or hemorrhage. If it is administered in hypertonic concentration it will abstract water from interstitial and intracellular fluids and increase blood volume by an amount more than administered. In isotonic concentration it will expand blood volume only by an amount equal to the volume (1 gm of albumin holds about 18 ml water) Burns, cirrhosis, nephritis…
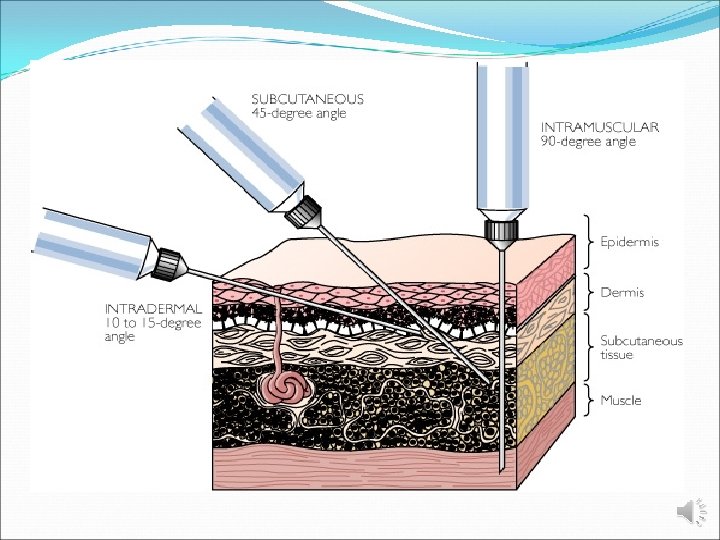

2. Intramuscular Route • It is the second route in rapidity of onset of systemic action after the I. V. route. • Injections are made into the striated muscle fibers that lie beneath the subcutaneous layer. Ø The sites of injections are: • Gluteal muscle (buttocks). up to 5 ml • Deltiod muscle (upper arm). 2 ml • Vastus laterals muscle (lateral thigh). up to 5 ml

2. Intramuscular Route Ø The major clinical problem is muscle or neural damage. Ø There are numerous dosage forms available for this route which includes: a. Solutions. b. Oil in water (o/w). c. Water in oil (w/o). d. Colloidal suspensions. f. Reconstitutable powders. Typically form a “depot” in the muscle mass from which the drug is slowly absorbed
. Most portions of")
3. Subcutaneous Route Lying immediately under the skin (below the dermis). Most portions of the arms and legs in addition to the abdomen. Volume: up to 2. 0 ml Normally aqueous or suspensions are given. Injection site may be massaged after injection to facilitate drug absorption Absorption (rate and extent) < i. m. < i. v. For daily administration (e. g. insulin) should be continuously changed or rotated. ØIncludes variety of drugs : 1. Vaccines 2. Insulin 3. Scopolamine 4. Epinephrine

4. Intradermal Route Ø It involves injection of the drug into the skin layer. (below the epidermis). Ø Given for diagnostic purposes or immunization. e. g. Allergy test materials. Ø Injected volumes are given at 0. 05 ml per dose. Volume: up to 0. 2 ml (0. 1 ml most common). Absorption is prolonged with slow onset. Suitable for testing allergens in diagnostic tests.

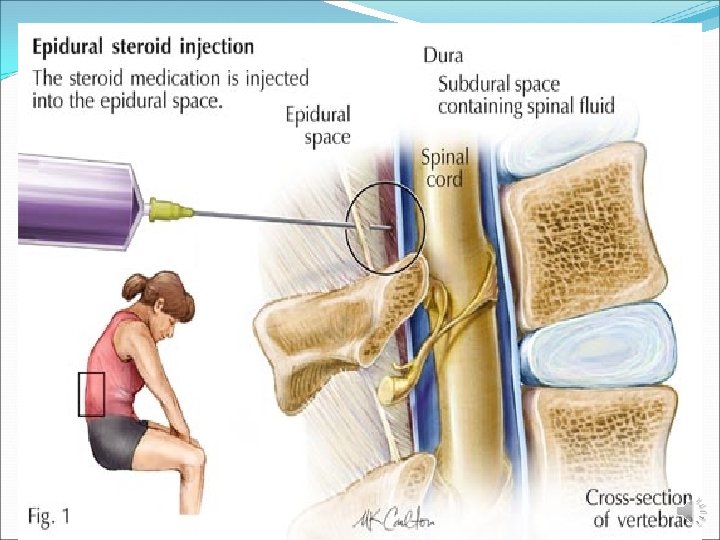
5. Other Parenteral Routes Intra-arterial route 1 -Injecting a drug directly into an artery 2 -Used to administer radioopaque contract media for reviewing an organ such as the heart or kidney or perfuse an antineoplastic agent at highest possible concentration to target organ. Intrathecal route 1 -Used to administer a drug directly into the cerebrospinal fluid. 2 -It is not the same route as spinal anesthesia where the drug is injected within the dural membrane surrounding the spinal cord, or in extradural or epidural anesthesia where the drug is deposited outside the dural membrane.

Routes of parenteral administration more specialized routes Intracardiac Injected directly into the cardiac muscle or a ventricle Used in emergency treatment Intra-articular Injected into the synovial fluid in a joint cavity. Ophthalmic injection Injected into different areas of the eye.
 Ready for injections 1 -Solutions 2 - Suspensions 3 -Emulsions")
Classification of Parenterals I) Ready for injections 1 -Solutions 2 - Suspensions 3 -Emulsions II) Ready to be combined with a vehicle 1 - Dry soluble products III) Ready for dilution 1 - Liquid concentrate 2 - Dry insoluble products

1. Solutions: Simplest and most convenient. Suitable for all routes of administration. Isotonic and has a p. H of 7. 4, buffers are used. Are usually aqueous but may be also found as mixtures of ether with glycols, alcohol, or other non-aqueous solvents. Most solutions have a viscosity and surface tension similar to water.

Oily Injections Oily solutions intended primarily for i. m. Vehicles: vary from vegetable oils to simple esters e. g. ethyl oleate

2. Suspensions: Are dispersed, multi-phased, heterogeneous system of insoluble solid particles intended principally for I. M and S. C injections. Must not cake during shipping and storage and should be easy to suspend and inject throughout its shelf life. Must not be administered directly to the bloodstream because of the danger of insoluble particles blocking the capillaries.

Ø Insoluble medicaments or adsorbed onto an insoluble matrix to modify the release. Particle size and size distribution must be carefully controlled to pass readily from the needle, Not Suitable for i. v. , intra-arterial or ophthalmic injections. e. g. methylprednisolone acetate BP, Insulin acetate BP

Suspensions Oily suspensions Far less common To provide an effective slow release or depot. For deep i. m. route e. g. penicillin G procaine with aluminium stearate suspension USP
. Oil-in-water sustained release depot preparations")
3 -Emulsions Water-oil emulsions of allergenic extracts (given subcutaneously). Oil-in-water sustained release depot preparations (given intramuscularly). Oil-in-water nutrient emulsions (given intravenously). e. g. Dexamethasone palmitate, Diazepam w/o allergenic extracts (s. c. )
 e. g. iron dextran")
Types of Parenterals Colloidal solutions Sterilized in autoclave (not filteration) e. g. iron dextran BP and iron sorbitol BP. Mixed solvent systems • When it is necessary to formulate a true solution. • e. g. of cosolvents Ethanol, propylene glycol and glycerol. • Restriction of the selection of cosolvent and its conc. is essential. • e. g. Digoxin injection BP (ethanol, propylene glycol and water) Concentrated solutions • Diluted or added to i. v. infusion. • toxic if given concentrated, e. g. potassium chloride (cardiotoxic)

4 -Dry Powders: Parenteral drug products are usually prepared as dry powder because it is unstable in solution. A disadvantage of this parenteral form is the need to reconstitute the product with the correct diluent prior to use. Dry powders may be intended to be reconstituted as a solution or as a suspension.
![Dry powders Reconstituted as solution suspension e. g: Thiopental Sodium for Injection [USP]. e.](http://slidetodoc.com/presentation_image_h2/929aad9a240cbe6147eac21c59fc6b39/image-32.jpg "Dry powders Reconstituted as solution suspension e. g: Thiopental Sodium for Injection [USP]. e.")
Dry powders Reconstituted as solution suspension e. g: Thiopental Sodium for Injection [USP]. e. g: Sterile Ampicillin for Suspension [USP].
- Slides: 32