Parasomnia Night Terrors Kelsey Carrio Megan Preovolos Christian



 Nightmare Night Terror Scary dream")




 n Acute")










 n Pre-cursor of serotonin n n Serotonin may")
 Four children, 8 -12 yrs")


- Slides: 27
Parasomnia: Night Terrors Kelsey Carrio, Megan Preovolos Christian Wilbur, Marjan Amiridavani COGS 175 June 1, 2007
Outline Intro to Night Terrors—Kelsey n REM/ n-REM—MJ n Causes—Christian n Treatments—Megan n Conclusions n
Parasomnias n Parasomnias are disruptive sleep-related disorders that can occur during arousals from REM sleep or partial arousals from Non-REM sleep. Parasomnias include nightmares, night terrors, sleepwalking, confusional arousals and many others.
Nightmare or Night Terror? (American Academy of Pediatrics, 1998) Nightmare Night Terror Scary dream awakens child. Child awakes only partially, if at all. Occurs in last hours of the night. Occurs one to four hours after child falls asleep. Child cries and is afraid. Child sits up, thrashes, and may struggle with caregiver. Child may scream, cry or talk aloud. Eyes may be staring ahead, with heart racing. Child is aware of caregiver. Child is not very aware of caregiver. Child may have trouble going back to sleep. Child often goes back to sleep without fully awakening. Child often remembers dream and may want to talk about it. Child has no memory of a dream, or of waking up, screaming, or thrashing.
Night terrors n n n A person experiencing a night terror or sleep terror abruptly awakes from sleep in a terrified state. The person may appear to be awake, but is confused and unable to communicate. They do not respond to voices and are difficult to fully awaken. Night terrors last anywhere from a few seconds up to 30 minutes, after which time the person usually lies down and appears to fall back asleep. People who have sleep terrors usually don't remember the events the next morning.
People experiencing sleep terrors may pose dangers to themselves or others because of limb movements. n Night terrors are fairly common in children occurring in approximately 5% of them mostly between the ages of three to five. n
N-REM vs. REM n n n Non-REM Slow EEG Muscular activity Dreaming rare 80% of sleep time n n n REM (paradoxical) EEG similar to awake person No movement Dreaming common Hard to arouse easily 20% of sleep time
Onset of Night Terror - EEG n n Spontaneous attack during stage 3 of NREM sleep 2 s of diffuse hypersynchronous high voltage delta wave arousal Brief EEG delta discharge immediately preceding the clinical episode Increased heart rate (shown from EKG)
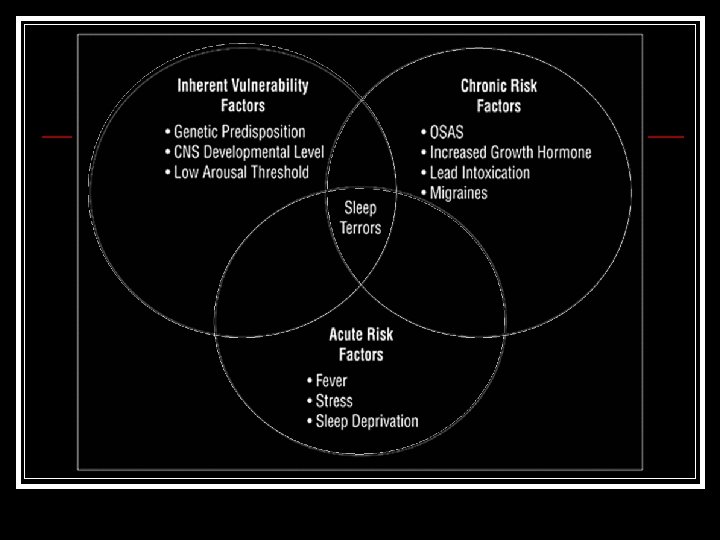
Causes of Night Terrors n Genetic Factors n Sleep Disordered Breathing (SDB) n Acute Triggers
Genetic Factors Guilleminault et. al. 2003 - 35% of children with both NT and SDB have at least 1 immediate relative with parasomnia. Kales et. al. 1980 - 96% had 1 or more relatives in the pedigree with NT or Sleepwalking. Owens et. al. 1999 - 60% risk if both parents were affected.
Sleep Disordered Breathing Guilleminault et al. 2003 - 51 of 84 children had BOTH NT and an additional sleep disorder. - If the SDB is treated, then the NT symptoms disappear. Owens et al. 1997 - Parasomnias are more common in children with Obstructive Sleep Apnea (OSA) than in a normative age-matched sample.
How SDB’s? n Sleep fragmentation due to sleepdisordered breathing may elicit an increase in slow-wave sleep as a recovery mechanism. This could be an increased risk factor for night terrors because they occur in stage 3/4 of sleep.
Acute Triggers Mild increases in psychosocial stress and relative sleep deprivation are known to trigger night terrors in affected individuals. These triggers most likely play a synergistic role in evoking the night terror, and are not the primary source when they
Treatments Education Behavioral Hypnosis Medication
Educate n Make sure parents understand n Transitory: Usually end on their own Regular sleep pattern n Safe environment n n n Remove sleep disturbances n n No bunk beds, safety gates, etc Night lights, sounds, etc Protect but don’t awaken
Behavioral Intervention “Waking Treatment” n n n Usually occur around same time each night Track timing of night terrors for a couple of nights Fully wake up 15 -30 mins before usually occur n n n Allow to sleep again after 5 minutes After week, stop waking. If terrors return, repeat waking for one more week 90% effective in study of 50 children (Oakey)
Hypnosis Stress reduction n In adults: n n Mild night terrors: self-hypnosis n n Deep breathing, concentrate on relaxing imagery Severe night terrors: n n Professional hypnotism Suggestions to reduce awareness of nocturnal sensory stimuli
Medication n Tricyclic Antidepressants n n n Ex: Imipramine, Trazodone Often used as temporary treatment in conjunction with hypnosis Benzodiazepines n n n Ex: Diazepam Suppress slow-wave (stage 3/4) sleep Disadvantages n n n Addictive Growth hormone secreted in slow wave sleep Also studies stating DOESN’T work (Cooper)
Melatonin Therapy Neurohormone produced by pineal gland n Therapy for sleep-phase onset delay n Take controlled release 30 mins before bedtime n Study: Abrupt disappearance of parasomnias in 12 year old boy (within 2 days) n -Smits et al.
L-5 -Hydroxytryptophan (Bruni et al, 2003) n Pre-cursor of serotonin n n Serotonin may cause production of sleep-producing factors Resolves conflict between slow-wave sleep and arousal 45 children: 34 given L-5 -HTP, 14 take placebo Episode recurrence after 6 months n n 2 in L-5 -HTP (6. 4%) 9 in placebo group (64. 3%)
Case Study Self-Hypnosis in Management (Kohen et al, 1992) Four children, 8 -12 yrs old n Treatment: 20 -60 mg of imipramine at bedtime followed by self-hypnosis n Strategy: n n n Demystify through education Establish prompt control through imipramine Train in self-regulation through self-hypnosis Discontinue medication but continue hypnosis
Conclusion n Unanswered questions n n n What causes the sudden occurrences to stop? Exact causes and remedies Alternate State of Consciousness? n n Is it even conscious? Are they aware?
References Bruni, et al. L-5 -Hydroxytryptophan treatment of sleep terrors in children. Eur J Pediatrics. 2004; 163: 402 -407 Cardoso, Silvia Ph. D and Sabbatini, Renato Ph. D “Night Terrors” www. cerebromente. org. br/. . . /terror 1_i. htm Copyright 1998 by State University of Campinas, Brazil Chiba, A. “Circadian Rhythms” 4 -19 -2007 http: //www. cogsci. ucsd. edu/~chiba/circadian_rhythms_07. pdf Di Gennaro, et al. “Night terrors associated with thalamic lesion” Clinical Neurophysiology, Volume 115, Issue 11, November 2004, Pages 2489 -2492 Durand , Mark and Jodi A. Mindell. Behavioral intervention for childhood sleep terrors. Behavior Therapy. 1999; 40(30): 705 -715. Guilleminault C, Palombini L, Pelayo R, Chervin R. Sleepwalking and Sleep Terrors in Prepubertal Children: What Triggers Them? PEDIATRICS Vol. 111 No. 1 January 2003, pp. e 17 -e 25. Haley, Carma. “Terror in the Night” http: //childrentoday. com © 1999 -2003 i. Parenting, LLC Kales A, Soldatos CR, Bixler EO, et al. Hereditary factors in sleepwalking and night terrors. Br J Psychiatry. 1980; 137: 111 -118. Kohen, et al. Sleep-terror disorder in children: the role of self-hypnosis in management. American J Clinic of Hypnosis. 1992 April; 34(4): 233 -244. Lask, B. A novel and non-toxic treatment for night terrors. BMJ 1988; 297(6648): 592. Matthews, B and M. Oakey. Triumph over terror. BR Med Journal. 1986; 292: 203. “Not Such ‘Sweet Dreams’” http: //www. talaris. org/spotlight_dream. htm Talaris Research Institute © 2005 Owens J, Millman R, Spirito A. Sleep Terrors in a Five Year-old Girl. Arch Pediatr Adolesc Med. 1999; 153: 309 -312. Owens J, Spirito A, Nobile C, Arrigan M. Incidence of parasomnias in children with obstructive sleep apnea. Sleep. 1997; 20: 1193 -1196. Rosen, et al. Sleep walking, confusional arousals and sleep terrors in the child. Principles and Practice of Sleep Medicine in the Child. Philadelphia, PA: Saunders. P 99 -106. “Sleep Disorders: Parasomnias” www. webmd. com/sleep-disorders/guide/parasomnias © 2005 -2007 Web. MD, Inc