Paradoxical Reaction in TB Done by Mazen Badawi

Paradoxical Reaction in TB Done by : Mazen Badawi Supervised by : Prof. Tariq Madani

Case l 18 yr old Saudi female presented with intermittent right flank swelling for 1 month. This swelling is progressively increasing in size and it would appear on standing and disappear when lying down.

Case l There were no associated abdominal pain or gastrointestinal or urinary symptoms. Patient denied any history of fever, weight loss or backache.

Case l She was diagnosed 5 months earlier with multifocal skeletal TB in hyoid, right mastoid and right occipital bones as well as the first 2 cervical vertebrae.

Case l She presented at that time with fever, weight loss, hearing loss, purulent discharge from her right ear and swelling over the right side of the neck overlying the hyoid bone

Case l Investigations: u A biopsy from the hyoid bone revealed caseating granuloma. No AFB or MTBPCR done u CT of the head showed lytic lesions in the mentioned bones

Case l Patient was started on 4 anti TB medications for 2 months and to continue on 2 medication for 4 months l Compliance was assured with regular follow ups l Patient had good improvement in symptoms in 4 months and then started to have right flank swelling

Case l On examination: the patient was afebrile, looked healthy. Abdominal examination showed non tender and soft fluctuant mass in the right flank which is prominent in standing position with no overlying skin changes. Examination of the spine was normal, and the rest of the physical examination was unremarkable.

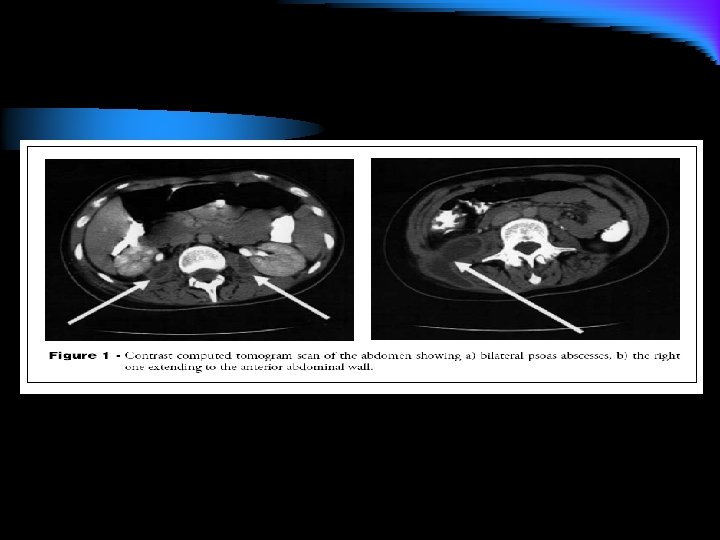
Case l Investigations: u CBC, ESR, LFT, renal functions were within normal u CXR was within normal u PPD >10 mm induration u CT Abdomen showed bilateral psoas abscess, the right one is bigger and extending to the abdomen and pelvis

Case l CT- guided aspiration of the right psoas abscess was done. Gram stain was negative. AFB stain and MTB-PCR was positive. l Pyrazinamide, ethambutol, moxifloxacin and amikacin was added for possible resistance

DD

l DD : Non tuberculous infection u Bacterial superinfection u New lesions of resistant TB u Progression of pre-existing and clinically silent psoas abscess due to drug resistance, incompliance or malabsorption u Drug fever , drug reaction, reduced drug levels due to drug- drug interaction u Different disease etiology, eg: lymphoma u Paradoxical reaction to anti TB drugs u

DD l Paradoxical reaction: Worsening of tuberculosis during appropriate anti TB therapy l Treatment failure: u Mycobacterial cultures +ve after 3 months or u AFB stain +ve after 5 months of appropriate treatment

In this case: l All bacterial, fungal and mycobacterial cultures turned out to be negative!!

l So, the additional drugs were discontinued , and the diagnosis of psoas abscess related to paradoxical reaction with anti TB was made l Patient continued on 2 drugs to complete total of 9 months. She was improving.
 or immune reconstitution inflammatory syndrome (IRIS, in HIV-coinfected pt.")
Definition l Paradoxical reaction (PR) or immune reconstitution inflammatory syndrome (IRIS, in HIV-coinfected pt. ) is defined as clinical, or radiological, or both, deterioration of preexisting tuberculous lesions, or the appearance of new lesions during the course of appropriate anti TB therapy in a patient who initially improves.

History : It is not new! l The first paradoxical drug reactions based on a possible immune response were reported by Robert Koch in 1890 when he attempted to treat tuberculous patients with injections of large amounts of killed tubercle bacilli (old tuberculin). This resulted in high fevers, ulcerating lesions, and increased morbidity and mortality.

You Need To Know l Incidence: 6 -30 % of patients receiving anti TB drugs l Previously believed to be only in patients who are co- infected with HIV l In HIV infected patients its found to be more with those receiving HAART , it can reach 30% l Might cause larger reaction to PPD skin test

You Need To Know l Usually it is mild, transient and self-limited, might start anytime within anti TB course : few days to many months and usually last 10 -40 days, some studies suggest diagnosis to be made only after 30 days of initiation of treatment. l In HIV+TB+ PR may show from 10 -180 days with mean of 60 days since HAART l Patients tend to gain weight. Some studies showed weight loss. l Usually complicates treatment TB lymphadenitis, cerebral & dissimenated TB

You Need To Know l Care should be taken in miliary PTB, expanding tuberculomas in brain, enalrging mediastinal LN, severe sepsis, uncontrolled high fever. l In HIV – paradoxical response can be seen following Rx of lepromatous leprosy, or following corticosteriod withdrawal, recovery of cytopenia after chemo, withdrawal immunosupp. In transplant recepient infected with Crypt. N. and engrafment of Stem C. T. l In HIV + there could be other co-infections that show paradoxical reaction: MAC, Cryptococosis, CMV, Pneum. Jiroviichi, Herpes Z. , HCV, HBV
: Some studies relates timing")
You Need To Know l Risk Factors ( HIV +): Some studies relates timing of HAART initiation with concomitant treatment of opportunistic infections u Other studies, concerned about CD 4 count <100 cells/micro. L at time of initiation, and use of powerful protease inhibitors and HIV RNA decline of more than 2. 5 logs. In pre-existing TB it might happen with CD 4<200 u l HIV - : patients receiving infliximab (eg for IBD)

Pathogenesis 1. Enhanced inflammatory response as a result of increased MTB antigen exposure from rapidly dying MTB to sensitized lymphocytes following anti TB therapy and immune reconstitution (esp. HIV patients on HAART) which lead to increase in IL-5 & TNF-a 2. strengthening of the host’s delayed hypersensitivity response 3. decrease in suppressor mechanisms and apoptosis of lymphocyte

Pathogenesis l In HIV + , the half life of HIV is 1 -4 days. HAART may give 90% reduction in viral load within 1 -2 weeks. This decline persists 8 -12 wk & then stabilizes. The increase in immune cells occurs in inverse proportion to the fall.

Clinical Manifestations l Depends on HIV status, and site of infection: ¾ of HIV+ TB+ will have fever u PTB: fever, malaise, ? wt loss, worsening resp. symptoms, trans. Worsening CXR : new opacities, LN enlargment, ARDS u Extra PTB: lymphadenitis, Pl. effusion, tuberculoma expansion u In some HIV+ there are reported cases of cutaneous lesions, peritonitis, epydidimitis, bowel perforation or granulomatous nephritis. u

Diagnostic tests it is a diagnosis of exclusion! u +ve AFB stain , MTB PCR are NOT diagnostic (may be due to dead bacilli) u PPD and caseating granulomatous inflammation on biopsy are NOT diagnostic as they may reflect enhanced inflammatory reaction to the antigen from dying bacilli and not active infection u May cause increase in CRP u Hawkey(3) associates high baseline monocyte count with increased PR incidence u

Treatment l no optimal treatment! Mild to moderate: symptomatic treatment u Severe & Life threatening : ? short course of steriods and monitoring the patient, suggested to be taken orally for 6 wk, however no controlled trial was done u Surgical intervention? u Anti TB & Anti retroviral should not be stopped (HAART may be stopped only if life threatened) u

Study: Paradoxical reactions during tuberculosis treatment in patients with and without HIV coinfection

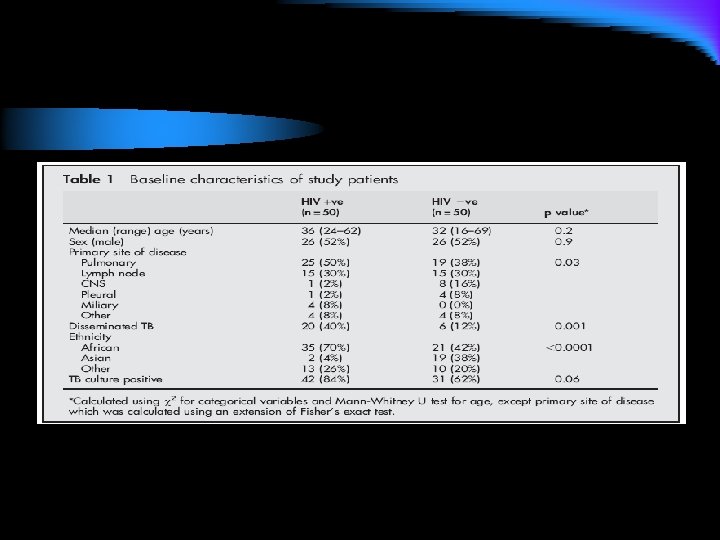
Background l It has been suggested that deterioration of TB during appropriate treatment, termed a paradoxical reaction PR, is more common and severe in HIV positive individuals on HAART. A group of TB patients who are HIV +ve were the cases and another group of TB patients who are HIV –ve were the control in a retrospective study.

Method l A study was undertaken to determine the frequency of PR and its associated features in a population of HIV+TB+ patients and a similar sized group of HIV-TB+ individuals

Methods Patients diagnosed with TB between February 1997 and February 2002 were identified from the Royal Free Hospital TB database which records all patients diagnosed with TB in our urban teaching hospital. Treatment was initiated either as an inpatient or an outpatient depending on symptom severity. All patients in the clinic received self-administered treatment. Clinical information was validated against patient case notes. Diagnoses were accepted if the patient had: l l l 1. 2. 3. l a positive culture for Mycobacterium tuberculosis; had been culture negative but AFB smear and/or nucleicacid amplification assay positive (TB Strand Displacement Amplification assay, Becton-Dickinson, NJ, USA) with clinicoradiological features and response to treatment consistent with TB; histological findings consistent with TB and response to treatment consistent with TB. Patients were excluded if they were followed up for less than 6 months or never started TB treatment.

METHODS l The comparator population was selected by identifying consecutive TB l l patients who satisfied the definition of diagnosis, did not meet the exclusion criteria, and had a documented negative HIV antibody test. PR was defined as a worsening of clinical or radiological findings following the initiation of appropriate antituberculous treatment in the absence of evidence of disease relapse or the presence of another diagnosis. Dissemination was defined as clinically or radiologically apparent disease at more than one site, with or without laboratory confirmation. Dual antiretroviral therapy was defined as the use of two nucleoside reverse-transcriptase inhibitors (NRTIs). HAART involved the use of two NRTIs with either a protease inhibitor (PI) or a non-nucleoside reverse-transcriptase inhibitor (NNRTI). Statistical analysis was performed using Fisher’s exact test, x 2 test, Mann-Whitney U test, and Kaplan-Meier methods.

Results Total pt 114 HIV + TB+ 64 Excluded 14 HIV-TB+ 50 HIV+ TB+ 50 4 died 4 no mathcing criteria 3 no records 3 f/u outside PR 5 PR 14

9 didn’t receive HAART 28 received HAART after TB Dx 2 pt. developed PR before anti TB Reason is severe or prolonged symptoms

l ESR, CRP, LDH , Hb, Albumin measured in all patients HIV+TB+ before and after PR developed. No significant change between those who developed PR and those who didn’t.
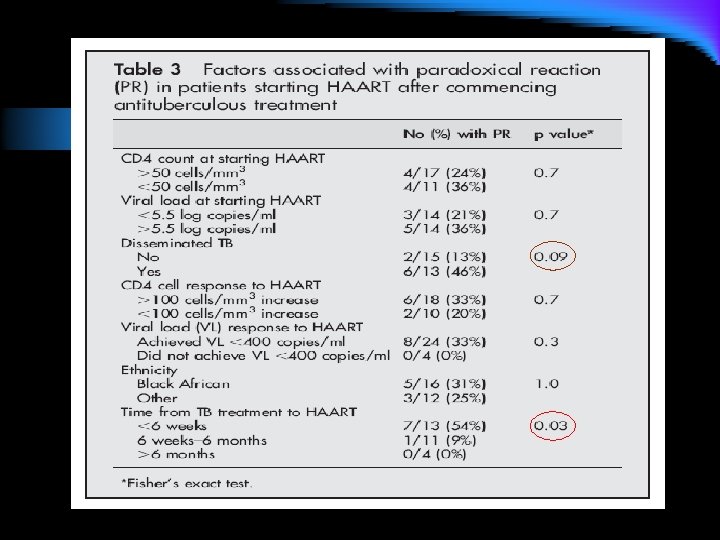

Analysis of data of the 28 HIV+TB+ patients who received HAART only after TB dx l 8 of the 28 patients (29%) had PR. l Their median CD 4 count at TB diagnosis was 58 cells/ml (range 30– 143) and the viral load was 5. 5 log copies/ml (range 5. 2– 5. 9). l No association was found between PR and baseline CD 4 count or CD 4 response on HAART in this study l In this group PR was significantly associated with starting HAART within 6 weeks of TB diagnosis (p=0. 03). l PR was more common in those with disseminated disease (6/13 with dissemination v 2/15 without dissemination; p=0. 09) and viral load suppression to , 400 copies/ml within 6 months (p=0. 3). However, none of these reached statistical significance.

DISCUSSION l Our results, based on a population of patients with a range of clinical disease, suggest that PR during treatment for TB is common in both HIV infected and uninfected individuals. The observed frequency of 28% in our HIV positive patients is lower than some groups have reported since the introduction of HAART, while our rate of 10% in HIV negative patients is higher than the rate of 2% reported by Narita et al in their HIVnegative comparison group. 5 We believe these differencesmay be due to patient selection. We have investigated a typical mixed inpatient and outpatient study population with a range of TB presentations. All patients received daily selfadministered treatment and, although not formally assessed in this study, adherence to treatment in our cohort is generally excellent. l The main differences between our HIV positive and HIV negative groups were with respect to ethnicity and the presence of disseminated TB. The former reflects the demographic characteristics in our practice as a whole. We observed PR in all ethnic groups with no difference in frequency according to race, although the sample size for this analysis was small. However, there have been no reports of ethnic differences in the occurrence of PR and we do not believe that ethnicity explains the increased frequency in the HIV positive group.

l We and others have shown a strong association between the use of HAART and PR. 10 The underlying mechanism for this is unclear. Our data suggest that PR is independent of both baseline CD 4 count and HAART mediated recovery of CD 4 cells as measured in peripheral blood. However, these may not accurately reflect local immune responses in, for example, the lung which are probably more relevant. 11 This might explain the reported slow recovery of M tuberculosis specific T cell responses in blood from patients starting HAART. 12 13 There is a suggestion that a rapid reduction in HIV plasma viral load may be associated with PR, as found by Navas et al. 10 l In practice, the association between early initiation of HAART and PR creates a dilemma for the clinician treating TB/HIV co-infection. Against this must be balanced the risk of further opportunistic infections if HAART is delayed. A large study of co-infected patients showed that four of 188 had a further AIDS defining illness (ADI) within the first 2 months of TB treatment. 14 Those at particular risk of further

l Although our study could not investigate the reasons which lead physicians to decide when to prescribe HAART after TB treatment and hence we cannot rule out confounding factors, our data suggest that delaying HAART to avoid PR may be advisable in the presence of disseminated TB but not necessary in those with low CD 4 counts alone. A flaw in this strategy may be the difficulty in accurately assessing the TB burden in manypatients with advanced immunosuppression. l In HIV negative patients admitted for treatment of TB, restoration of skin test responses to PPD after 2 weeks of antituberculosis treatment have been reported. 15 This has been ascribed to reversal of immunosuppression due to TB itself. However, improved nutritional status and alcohol cessation, which might be most marked in those admitted for treatment, have been shown to affect cell mediated immunity 16 and thus may also play an important part.

l l Disseminated TB—which is seen more frequently in HIV infected TB patients 17—was associated with PR, although this did not reach statistical significance. This may not only reflect the importance of immune status, as discussed above, but also suggests that overall mycobacterial load can influence the development of PR. Campbell and Dyson 3 proposed that rapid killing of bacilli by effective antituberculous treatment can cause the release of large amounts of tuberculoprotein and other cell wall products. The ability of such materials to elicit a severe and potentially fatal inflammatory response was described first by Koch himself. 18 It is logical to assume that the overall inflammatory response to M tuberculosis reflects both the number and function of appropriate immune cells and the amount of antigen that they encounter. The severity and frequency of PR would therefore be expected to increase if disseminated or extensive single organ disease was present. We have shown that PR is a common phenomenon during TB treatment in a combined inpatient and outpatient population, regardless of HIV antibody status. However, it is seen more frequently in co-infected patients receiving HAART. The reasons for this remain unclear, although the timing of HAART initiation in relation to TB diagnosis appears to be important, as does the presence of disseminated disease. Our study is limited by its retrospective nature and relatively small size. Results that do not achieve statistical significance at the 5% level may become significant with a larger sample. We believe that this warrants further prospective, clinical, and laboratory investigation

Summary l l l l PR is a serious, easily missed phenomenon Diagnosed by exclusion Higher association with HIV+ Suggestion of starting HAART after approx. 1 - 2 months of OI treatment (TB, HBV…)if AIDS is severe give 2 week gap Don’t stop Anti TB Don’t stop Anti retrovirals unless life was threatened Steriods may help in individual cases Larger sample studies are needed especially regarding management

l Questions?

REFERECES 1 - Fayez H, Imad M, TB paradoxical reaction, clinical note. Saudi J M 2007 2 - Narita M, Ashkin D, Hollender ES, et al. Paradoxical worsening of tuberculosis following anti-retroviral therapy in patients with AIDS. Am J Respir Crit Care Med 1998; 158: 157– 61. 3 -Hawkey C, Yap T, Pereira J, et al. Characterization and management of paradoxical upgrading reactions in HIV-uninfected patients with lymph node tuberculosis. Clin Infect Dis 2005; 40: 1368– 71.

Thank you!
- Slides: 46