Paracetamol Poisoning Dr Ben Mc Kenzie Emergency Physician

Paracetamol Poisoning Dr Ben Mc. Kenzie Emergency Physician

Case Example � 13 year old girl � Drinking with friends to see who could take the most panadol and aspirin. � Took maybe 60 tablets, 12 aspirin � 2 days ago � Presents with RUQ pain and vomiting

Yes this is a real case! Increasing pill parties in USA. .

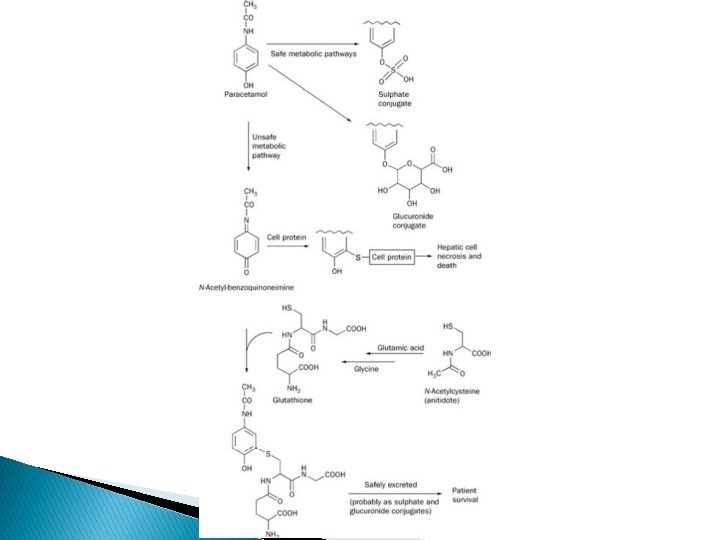
Normal Metabolism � 90% conjugated and excreted in urine ◦ Conjugated with sulfate ◦ Conjugated with glucuronide � 2% excreted unchanged in urine � Rest metabolised by cytochrome P 450 mixed function oxidase system (CYP 2 E 1, CYP 1 A 2, CYP 3 A 4) ◦ Forms N-acetyl-p-benzoquinoneimine (NAPQI) ◦ NAPQI is TOXIC!! But luckily is conjugated with Glutathione in the liver under in therapeutic doses of paracetamol.

Toxicity � Once sulfation and gluronidation pathways are saturated metabolism is shunted down the CYP 450 pathway of oxidation. � One glutathione is depleted then NAPQI accumulates. � NAPQI starts binding hepatic cells proteins and cell death.

Toxicity more likely � When there is overdose � If induction of CYT P 450 enzymes ◦ Carbamazepine and phenytoin use induce CYP 2 E 1 ◦ Malnourished – less glutathione stores. ◦ Alcoholics with repeated paracetamol insults �Induced CYP 450 enzymes �Malnourished, fasting �Not increased risk with single overdose

Toxicity less likely � In children under 5 ◦ More conjugation and more glutathione stores

Risk Assessment – Single Ingestion � <150 mg/kg in adults or 7 -10 g toxicity unlikely � <200 mg/kg in children toxicity unlikely �> 350 mg/kg Most patients develop hepatoxicity

Risk Assessment – Single Ingestion � Rumack-Matthew Nomogram was the original plotted graph of untreated patients paraectamol concentration against time. 60% above the line developed hepatoxicity. � This has been modified with subsequent evidence taken into account. � Lowered by 25% to allow for inaccuracies in assessment.

Paracetamol Nomogram

Risk Assessment – Single Ingestion � Blood taken at 4 hours post ingestion or immediately if the patient presents after 4 hours. � Blood taken prior to 4 hours is a waste of time and money!

Risk Assessment – Single Ingestion � Panadol Osteo…. Sustained release ◦ Use the same nomogram despite it not being validated for these preparations ◦ No evidence to suggest toxicity is different

Risk Assessment – Chronic ingestion � Some patients take supratherapeutic doses over a number of days. ◦ Dental pain ◦ Codeine abuse ◦ Illness (these patients are often dehydrated, malnourished and higher risk. Risk Assessment Guide � 10 grams (child 200 mg/kg) in 24 hours � 6 grams (child 150 mg/kg) per day for 48 days

Paracetamol as a coingestion � You do not need to do routine paracetamol levels if a patient is cooperative and able to give a history (Best. Bets) � However if doubt about reliability or unconscious then it is a cheap and easy test to do.

Natural History � Hepatotoxicity takes 18 – 36 hours to develop. � All patients have an ALT/AST rise by 36 hours � Prior to hepatotoxity most patients develop nausea, vomiting, feel unwell. But maybe asymptomatic. � Liver toxicity – RUQ pain, nausea, unwell, jaundice. � ALT/AST peak day 3 and LFTS are repeated in a serial fashion to map the fall. � Development of liver failure depends on the amount of hepatic injury

Liver failure � Hepatitis � Coagulopathy � Shock � Renal Failure � Lactic Acidosis � Hypoglycaemia � Cerebral oedema - hyperammonaemia � Death from multi-organ failure

Decontamination � Charcoal if present within 1 hour � Only if they are conscious and compliant � Remember there is an antidote

N-Acetylcysteine � Thought to provide cysteine to enhance glutathione synthesis. � Not contraindicated if a patient is allergic to sulphonamides/”sulfas” � 10 -20% may develop flushing or anaphyactoid reaction and almost all people tolerate it when it is restarted/slowed rate. � All patients who receive NAC within 8 hours do well.

N-Acetylcysteine � ALL PATIENTS WHO RECEIVE NAC WITHIN 8 HOURS DO WELL Regime In Australia � 150 mg/kg IV infusion, over 15 to 60 minutes � 50 mg/kg IV infusion, over 4 hours � 100 mg/kg IV infusion, over 16 hours.

N-Acetylcysteine � People over the nomogram line � People who you risk assess as potential toxicity and result will take longer than 8 hours post ingestion to obtain. � Patients with abnormal LFTs � Supratherapeutic ingestions with high risk/abnormal LFTs – base on dose ingested

N-Acetylcysteine For how long? - If the patient receives N-Acetylcysteine within 8 hours they maybe discharged after the 20 hour infusion is complete. - Continue the infusion until paracetamol levels are undetectable if hepatic damage occurs (in consultation with clinical toxicologist)

Case – 13 Year old girl � Na 137 K 3. 5 CL 98 HCO 3 30 Urea 2. 6 Cr 46 � Alb 49 AST 7234 ALT 5896 GGT 18 ALP 224 � Bili 16 � Paracetamol <30 � BSL 6. 4 � Lactate 1. 6 � INR 1. 7 Management

Case – The 13 year old girl � On presentation AST 7234 ALT 5896 � 18 hours later: AST 1642 ALT 3392 INR 1. 4 � 26 hours later: AST 895 INR 1. 3 � 34 hours later: AST 28 INR 1. 1 Lucky!

Severe Hepatic Failure � Refer � Liver to liver unit ICU recovery phase commences day 3 � Transplant/Death

Every Day toxicology � Patient comes in and has taken 20 tablets of olanzepine/respiridone/quetiapine/largactil � What is your plan?

Toxicology Framework � Risk Assessment � Decontamination � Enhance Elimination � Antidotes � Supportive care

Supportive care � Is the treatment you initiate to support a patients physiology.

Oxygenation

Airway Support � Usually GCS of 8 is indication for intubation unless short acting agent involved. � Prevent aspiration.

Cardiovascular Support � BP low because less awake and less endogenous catecholamines � Direct pharmacological effects � Dehydration � Part of multiorgan failure

Cardiovascular Support

Temperature Support

Bladder Support � Many patients can’t urinate and its an amazing ICU physiological monitor. � Will also stop patients being agitated when their bladder is full!

Renal Support

Others � Pressure Care � Blood sugar � Monitoring
- Slides: 36