PANKREAS DR RUTH SHIFA PANCREAS ENDOCRINE EXOCRINE Most













, continuous, twisting Q")








- Slides: 23
PANKREAS DR. RUTH SHIFA
PANCREAS • ENDOCRINE • EXOCRINE • Most imp disease. Diabetes mellitus • tumors • Pancreatitis • Carcinomas
• Functions of pancreas • Endocrine portion constitute what portion? ? ? • B cells secrete : ? • Endocrine cells are called: ? • How many I of L cells are present: ?
• Pancreatic acini exocrine acinar cells. • synthesis and packaging of digestive enzymes for secretion into a central lumen.
acute chronic Inflammation of the Pancreas
Clinical Situation Pt. X • a 32 year, • divorced, • business executive brought to the emergency department C/O- abdominal & back pain and vomiting x 2 days. 6
O/E - trying to sit up, continuously movement on the bed. is alert ; able to answer questions, but refuses to let anyone touch his abdomen or his back. He rates his pain at 10/10
His skin is hot, dry and flushed with turgor and he complains of extreme thirst. VS: BP 100/60, T-100°F, P-120, R- 28 shallow, O 2 sats-90%
• Laboratory tests § Serum amylase- hallmark test § Serum lipase – also elevated § Blood glucose § Serum calcium- Decreased § Triglycerides Acute Pancreatitis
CAUSES • GET SMASHED
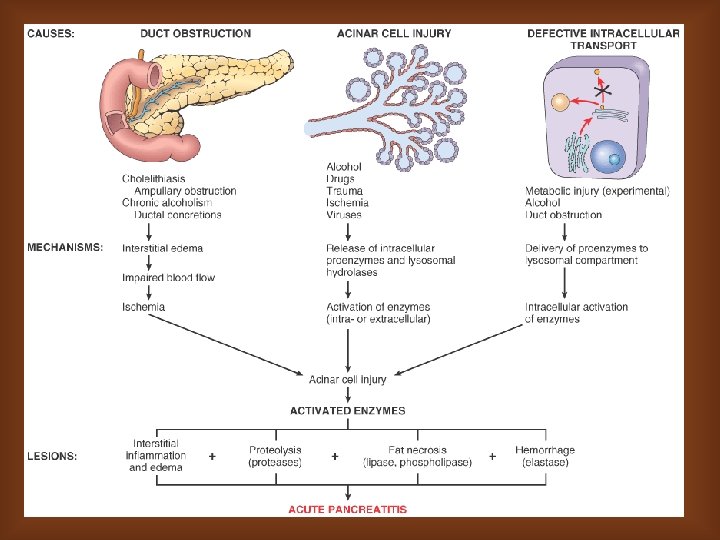
Acute Pancreatitis Etiology and Pathophysiology Pancreatic Ducts become obstructed Hypersecretion of the exocrine enzymes of pancreas These enzymes enter the bile duct, where they are activated and with bile back up into the pancreatic duct Pancreatitis
Progression of Disease • Autodigestion Acute Inflammation of Pancreas Necrosis of Pancreas Digestion of vascular walls Thrombus and Hemorrhage Death
Acute Severe Pancreatitis Pathophysiology Injury or disruption of pancreatic ducts leakage of active pancreatic enzymes autodigestion Breakdown of cell membranes edema vascular damage, hemorrhage, necrosis inflammatory mediators Shock, MODS, …. . 13
None stated – comes on when recumbent P Deep, piercing (knife-like), continuous, twisting Q R LUQ or mid-epigastrium radiating to back Patient may flex spine to get relief Aggravated by eating & alcohol Unrelieved by vomiting Aggravated by supine position or walking Relieved by sitting up & leaning forward S Severe “ 10”/10 T Sudden onset CLINICAL FEATURES 14
Morphology-Gross & M/E. • Mild inflammation and edema to severe extensive necrosis and hemorrhage. • Edema • Fat necrosis • An acute inflammatory reaction • Proteolytic destruction of pancreatic parenchyma • Destruction of blood vessels with interstitial hemorrhage.
Diagnostic Tests & Procedures • • • Abdominal and chest films CT scan Ultrasound Aspiration biopsy Peritoneal lavage • Endoscopic Retrograde Cholangio-pancreatography (ERCP) 17
Chronic pancreatitis
COMPLICATIONS
PANCREATIC NEOPLASMS
Serous cystadenoma
Adenocarcinoma
• Questions 1. Pancreatitis-acute/chronic 2. Adenocarcinoma 3. Pathophysiology of pancreatitis