Pancreatitis Pancrease In human beings the pancreas is

Pancreatitis

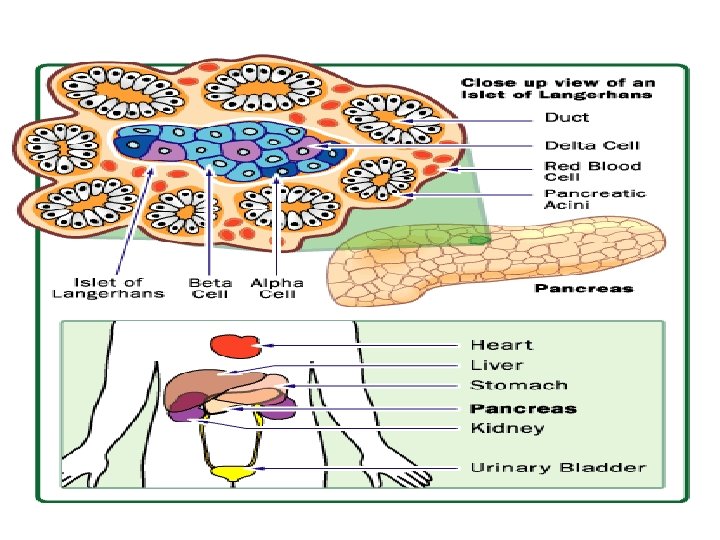
Pancrease In human beings, the pancreas is a 6 -10 inch elongated organ weighing 65 to 160 grams and lying in the abdominal cavity. It lies posterior to the stomach, anterior to the kidneys, and empties into the duodenum portion of the small intestine. The human pancreas can be divided into five regions: (1) the head, which touches the duodenum, (2) the body, which lies at the level of second lumbar vertebrae of the spine, (3) the tail, which extends towards the spleen, (4) the uncinate process, and (5) the pancreatic notch, which is formed at the bend of the head and body. The pancreatic duct or duct of Wirsung runs the length of the pancreas and empties into the duodenum at the ampulla of Vater. The common bile duct usually joins the pancreatic duct at or near this point.

Functions…. It makes pancreatic juices & hormones. The pancreatic juices are enzymes that helps in digestion of food in small intestine (duodenum). Pancrease is a compound gland coz it Composed of both exocrine & endocrine tissues.

Blood supply of pancrease Arterial supply…. The pancreas is supplied arterially by the pancreaticoduodenal arteries: the superior mesenteric artery feeds the inferior pancreaticoduodenal arteries the gastroduodenal artery feeds the superior pancreaticoduodenal artery. Venous drainage…. Venous drainage is via the pancreaticoduodenal, veins which end up in the portal vein. The splenic vein passes posterior to the pancreas but is said to not drain the pancreas itself. The portal vein is formed by the union of the superior mesenteric vein and splenic vein posterior to the neck of the pancreas. In about 40 percent of people, the inferior mesenteric vein also joins with the splenic vein behind the pancreas; in most people it simply joins with the superior mesenteric vein instead.

Pancreatitis It is inflammation of pancreas. Pancreas secrete enzymes which help in digestion of food ie trypsin, chymotrypsin, amylase, lipase, estrase etc. Normally, digestive enzymes do not become active untill they reach the small intestine where they begin digesting food. But, if these enzymes become active inside the pancreas, they start digesting pancreas it self & primarily due to intracellular activation of trypsinogen to trypsin by numerous stimuli assiciated with acinar cell injury.

Acute pancreatitis An acute condition presenting with abdominal pain & is usually associated with raised pancreatic enzyme levels in blood & urine as a result of in flammatory disease of pancreas. Incidence…… Varies from 21 -50 cases/lakh population. Diseese may occur at any age with peak in young men &older women. About one third of patient die in early phase of attack coz of multiple organ failure. While deaths occuring after 1 st week of onset are due to infective complications. 80% of patient have mild attack of pancreatitis & mortality is 1% while who have severe attack mortality varies 20 -50%.

Pathogenesis The anatomical changes of acute pancreatitis reflect two fundamental events: 1 -Autodigestion of pancreatic substance by in appropriately activated pancreatic enzymes(Normally, pancrease are protected from autodigestion by synthesis of pancreatic enzymes in acinar cell in proenzyme form & by confinement of yhese proenzymes to membrane-bound compartments(zymogen granules)within acinar cell before secretion. In acute pancreatitis these proenzymes become active coz of low p. H & increase in intracellular ca or coz of cathepsin B. these active enzymes cause disintegration of acinar cells & fatty tissue in & around the pancreas, damaging the elastic fibers of blood vessels & leading to vascular damage) 2 -Acinar cell injury response mediated by proinflamatory cytokines: (Damaged acinar cells release potent cytokines that attract neutroplhils & macrophages. These inflammatory cells release more cytokines such as necrisis factor, interleukin 1, nitric oxide & platelet activating factors into pancreatic tissue & circulation, thereby amplifying the local & systemic inflammatory response syndrome(SIRS)& this leads to multiple organ damage syndrome(MODS).
 & alcohol abuse(28%). The remaining are Congenital……")
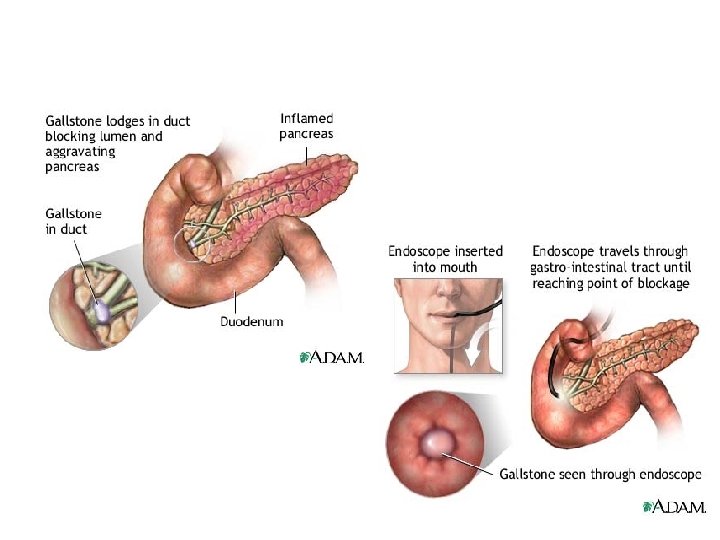
Aetiology Major causes are biliary calculi(50 -70%) & alcohol abuse(28%). The remaining are Congenital…… Pancreas divusum Metabilic……. Hyperlipoproteinuria, Hypercalamia, Drugs(thiazide diuretics), genetics Mechanical…. Traumatic injury, Perioperative injury Vascular…… Shock, atheroembolism, Polyarthritis nodusa Infection…. . Mumps, Coxsakie virus, Mycoplasma pneumoniae Idiopathic…. .

Clinical features • • • Severe upper abdominal pain, with radiation through to the back, is the hallmark of pancreatitis. Nausea and vomiting (emesis) are prominent symptoms. Shock(not only coz of hemorrhage but coz of release of vasodilating agents ie prostaglandin, bradykinin). Findings on the physical exam will vary according to the severity of the pancreatitis, and whether or not it is associated with significant internal bleeding. The blood pressure may be high (when pain is prominent) or low (if internal bleeding or dehydration has occurred). Typically, both the heart and respiratory rates are elevated. Abdominal tenderness is usually found but may be less severe than expected given the patient's degree of abdominal pain. Bowel sounds may be reduced as a reflection of the reflex bowel paralysis (i. e. ileus) that may accompany abdominal catastrophe. Turner sign & Cullen sign

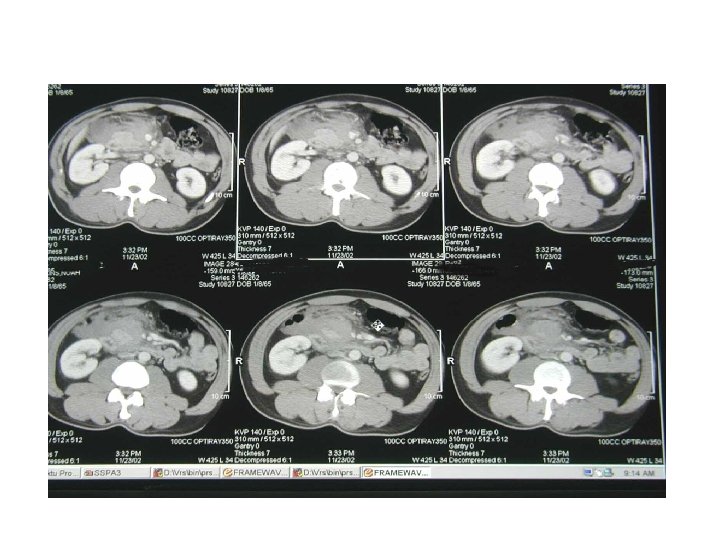
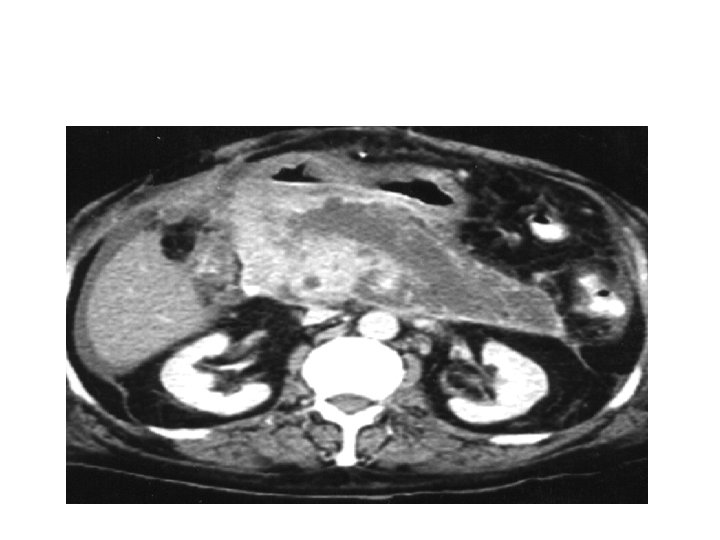
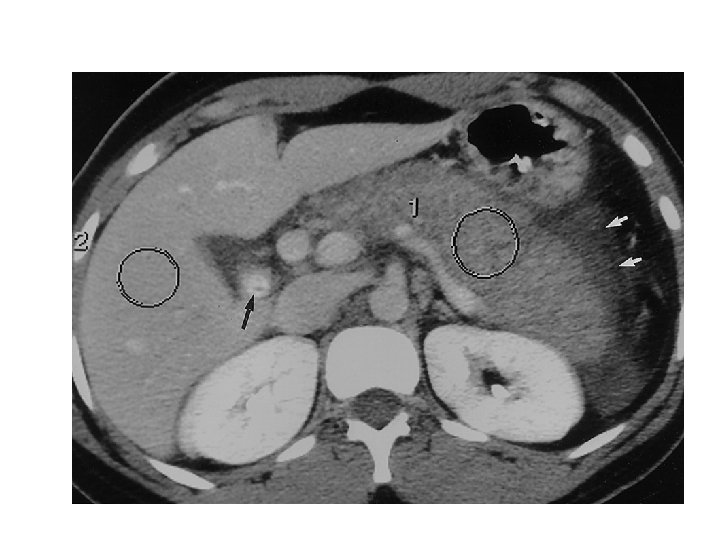
Investigations • Serum amylase has low sensitivity and specificity • 20% cases of pancreatitis have normal serum amylase (particularly alcoholic aetiology) • Serum lipase are more sensitive APACHE II score Multivariate scoring system Measure objective parameter - vital signs and biochemical analysis Can be used throughout course of illness USG(swollen pancreas may be detected, valuable in detection of peritoneal fluid, gallstone, dilation of common bile)

Contrast-enhanced CT scoring system Grade A B C Criteria Norma. L glandular collection Focal or diffuse enlargement, Small intra-pancreatic fluid Any of the above. Peripancreatic inflammatory changes. Less than 25% gland necrosis D Any of the above. Single extrapancreatic fluid collection 25 -50% gland necrosis E Any of the above. Extensive extrapancreatic fluid collection. Pancreatic abscess. More than 50% gland necrosis

• • • Ranson's criteria On admission – Age > 55 yrs – WCC > 16, 000 – LDH > 600 U/l – AST >120 U/l – Glucose > 10 mmol/l Within 48 hours – Haematocrit fall >10% – Urea rise >0. 9 mmol/l – Calcium < 2 mmol – p. O 2 < 60 mm. Hg – Base deficit > 4 – Fluid sequestration > 6 L Can not be applied fully for 48 hours Also poor predictor later in the disease To predict the severity, three or more factors should be present. . Glasgow criteria On Admission Age >55 yrs WBC Count >15 x 109/L Blood Glucose >200 mg/d. L (No Diabetic History) Serum Urea >16 mmol/L ( No response to IV fluids) Arterial Oxygen Saturation <76 mm. Hg Within 48 hours Serum Calcium <2 mmol/L Serum Albumin <34 g/L LDH >219 units/L AST/ALT >96 units/L

Management • Early treatment • Aims of treatment are to : – To halt progression of local disease – Prevent remote organ failure • Requires full supportive therapy – often on ITU or HDU • Urinary catheter, CVP line and possibly arterial line • Regular assessment of Ca, blood sugar, LFTs • Patients require: – Fluid resuscitation with both colloid and crystalloid – Correction of hypoxia with an increased inspired oxygen or ventilation – Adequate analgesia - opiate or epidural • Increasing evidence that antibiotic prophylaxis useful in severe pancreatitis • If gallstone is aetiology then ERCP(endocsopic retrograde cholangiopancreatography)is indicated. • If no improvement in 48 hrs then do urgent edoscopic intervention.

Complications • • • • Local…. . Necrosis +/- infection Pancreatic fluid collections Colonic necrosis Gastrointestinal haemorrhage Splenic rupture Systemic…… Hypovolaemia and shock Coagulopathy Respiratory failure Renal Failure Hyperglycaemia Hypocalcaemia • SIRS • MODS

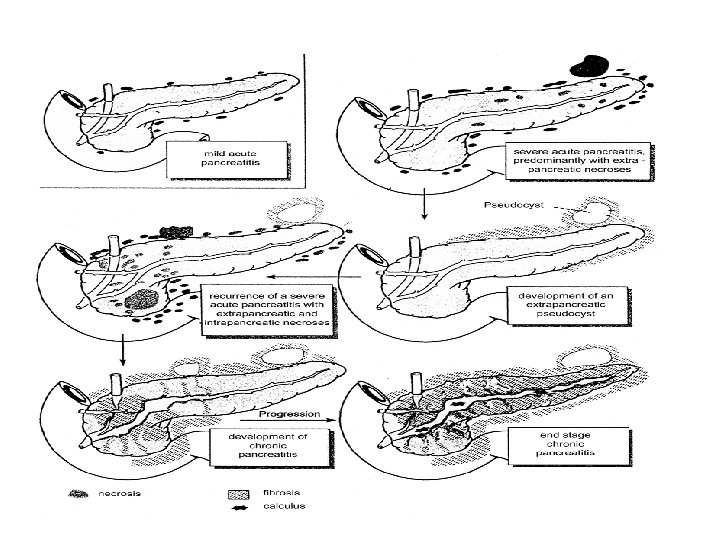
Acute hemorrhagic pancreatitis • It is most severe form of acute pancreatitis. • Gross appearance ischaracterized by blue-black hemarrhage with gray-white necrotic softening, sprinkled with foci of yellow white chalky fat necrosis. Foci of fat necrosis may be found in omentum & mesentery of bowel. In most cases peritoneal cavity contains a serous, turbid, brown tinged fluid in which glibules of fat can be identified. • This fluid may become secondarily infected to produce supporative peritonitis.

Choronic pancreatitis • It is characterized by recurring or persistent abdominal pain with continued loss of pancreatic parechyma & replacement by fibrous tissues with or without steatorrhea or diabet. es mellitus. Incidence…… In Europian, North Amirican studies range from 2 -10 cses/lakh population/year. Male>Female…. . 4: 1 MEAN AGE OF ONSET IS 40 YEARS. Aetiology…… Gallstone, High alcohol consumption Trauma, Idiopathic Heriditery pancreatitis(abnormal catatonic trypsinogen due to abnormality in long arm of chromosom 7 in which histadine replace arginine &trypsinogen to trypsin intracellularly)

Pathogenesis 1 -Hyper secretion of protein from acinar cell in absence of increased fluid scretion permits the presipitation of protein which admix with cellur debries that forms ductal plug which cause obstruction. 2 -Normally. GFTR(cystic fibrosis transmembrane conductance regulator)gene mediates secretion of bicarbonate rich alkaline pancreatic juice. If mutation occur in this gene then redeuce intaluminal fluid & bicarbonate level& lowers the normal p. H. These conditions reduces the solubility of secretd pritein& this give thickened & viscous secretions that tend to obtruct the ducts. Clinical features…. . Repeated attacks of severe abdominal pain or recurrent attack of mild pain or persistant abdominal pain & bach pain. If disease is on head of pancreas then pain is on epigastrium & right subcostal region. If disease is on left side patient have pain in left subcostal region & back pain, radiate to shoulders specially to left shoulder) Nausea, vomiting, wt, loss Diarrhea, Oily stool

Investigations 1 -Pancreatic function test 2 -MRI, CT 3 -MR cholangiogram, MR pancreatogram 4 -ERCP or percutaneous pancreatography Treatment…. . Diet low in fat. No alcohol, tabacco, smoking, morphine Pancreatic enzyme supplimentation Antioxidents to mop up oxygen free redical has been tried. Surgery…. . Most patient have mass in head of pancreas so resection of head of pancreas by pancreatoduodenectomy or beger procedure. If duct is markedly dilated, a longitudinal pancreatojejunostomy or frey procedure. Rarely, disease at tail of pancreas then do distal pancreatomy.


Prognosis • 80% of patients have mild pancreatitis with good recovery • Mild disease accounts for less than 5% of the mortality form pancreatitis • Mortality from pancreatitis due to: – Early multiple organ failure – Late infected pancreatic necrosis – Haemorrhage – Associated co-morbidity Development of Pancreatic cancer is a risk in those who have pancreatitis more than 20 years.
- Slides: 26