Pancreatic cancer Pathology l Exocrine l Solid Infiltrating



: 7(+), 19(+), 20(-) l CEA l CA 19")









 Right-side (N=564) Left-side (N=52)")












, CK 7(+) l Squamous cell, small")











- Slides: 41
Pancreatic cancer
Pathology l Exocrine l Solid Infiltrating ductal adenocarcioma: most l Variant of ductal adenocarcinoma l l Signet-ring cell, medullary, adenosquamous, anaplastic Acinar cell carcinoma l Pancreatoblastoma l l Cystic l Endocrine
Pathology l Exocrine Solid l Cystic l Mucinous cystic neoplasm l Intraductal papillary mucinous neoplasm l Serous cystic neoplasm l Solid pseudopapillary neoplasm l l Endocrine
Immunohistochemistry l Infiltrating ductal adenocarcinoma Cytokeratin(CK): 7(+), 19(+), 20(-) l CEA l CA 19 -9 l Mucins l
Risk factors of pancreatic cancer l Advanced age l Low socioeconomic status l Cigarette l Diabetes mellitus l Chronic pancreatitis l High-fat and cholesterol diet l Carcinogens exposure l PCBs, DDT, NNK, benzidine
Clinical presentation l Abdominal pain l Jaundice, obstructive l Right-side dominant l Weight loss, anorexia l New-onset DM l Acute pancreatitis l Especially no risk factors, stones or alcohols
Clinical presentation l Physical signs Jaundice: skin and sclera l Hepatomegaly l Palpable gall bladder l Lymphadenopathy l Left supraclavicle: Virchow’s node l Periumbilical: Sister Mary Joseph’s node l Peri-rectal region: Blumer’s shelf l
Diagnosis l Image studies CT or MRI: image of choice, equivalent l ERCP: direct imaging of p-duct, replaced by CT/MRI l EUS: more accurate for tumor itself l l l EUS-FNA PET: to be investigated l Histopathologic diagnosis
Diagnosis l Image studies l Histopathologic diagnosis Direct operation: curative or palliative l Percutaneous l l l More complication: hemorrhage, pancreatitis, fistula, abscess, tract seeding EUS-FNA
Staging l. T T 1: limited to pancreas, <2 cm l T 2: limited to pancreas, >2 cm l T 3: extend beyond pancreas, not involve celiac axis or SMA l T 4: involve celiac axis or SMA(unresectable) l l. N l N 1: regional LN(+)
Staging l IA: T 1 N 0 M 0 l IB: T 2 N 0 M 0 l IIA: T 3 N 0 M 0 l IIB: T 1 N 1 M 0, T 2 N 1 M 0, T 3 N 1 M 0 l III: T 4, any N, M 0 l IV: M 1
Treatment – surgical resection l Pancreatic l head and neck Pancreaticoduodenectomy +/- distal gastrectomy: Whipple’s operation l Mortality: 2 -3% l l Sepsis, hemorrhage , CV event Morbidity: 40 -50% l Leakage, abscess, delayed gastric emptying, hemorrhage l Pancreatic tail
Treatment – surgical resection l Pancreatic head and neck l Pancreatic tail l No obstructive jaundice in early state l l Tend to be larger, usually metastasis at dx Distal pancreatectomy
Right-side versus Left-side pancreatic resection: John Hopkins Experience (1984 -1999) Right-side (N=564) Left-side (N=52) P value Tumor diameter 3. 1 cm 4. 7 cm <0. 01 Margin(+) 30% 20% NS LN(+) 73% 59% 0. 03 Post-op mortality 2. 3% 1. 9% NS Overall complication 31% 25% NS Post-op hospital stay 11 d 7 d NS Median survival 18 m 12 m NS
For recurrence l Disease l nature Locally recurrence and distant mets l Neoadjuvant/adjuvant l treatment Chemoradiation 5 FU, MMC, Cisplatin, Paclitaxel, Gemcitabine l Relative radioresistant l Mostly single arm l No definite evidence of survival benefit l
Unresectable disease l Palliative surgery l RT or CCRT Radio-resistance l 5 FU, Gemcitabine l Really benefit? l l Palliative chemotherapy
Palliative surgery l Obstructive jaundice l Duodenal obstruction Hepaticojejunostomy l Choledochoduodenostomy l Cholecystojejunostomy l l Pain l relief Neurolysis
Systemic chemotherapy l Problems Highly resistant to chemotherapy l Usually poor performance l l Pain, N/V, cachexia, weakness Impaired liver function l Usually lack of measurable lesions l l Variation in phase II studies
Chemotherapy – historical l 5 -FU l is cornerstone Combination with Adramycin, mitomycin: FAM l Cyc, MTX, Vincristine, Mitomycin l Epirubicin, cisplatin, carboplatin, Ara-C High response rate in phase II : 40% Not confirmed in phase III l l Combination not better than 5 FU alone
Gemcitabine l Well-tolerated agent l Phase III study, Gemzar vs. 5 -FU Response rate: 5. 4% vs. 0% l Survival: 5. 65 m vs. 4. 41 m (p=0. 0025) l Clinical benefit: 23. 8% vs. 4. 8 l l l Pain, performance status, weight gain Toxicity similar with 5 -FU l Gemcitabine superior to 5 -FU
Gemcitabine-based combination
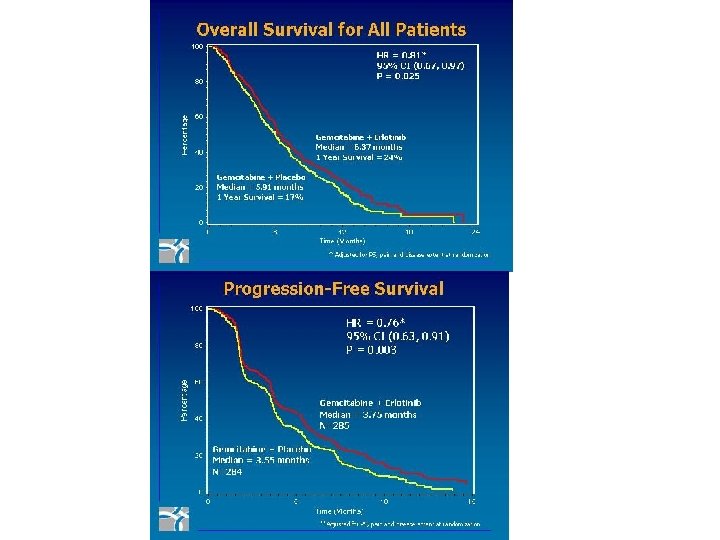
Gemzar+Tarceva vs. Gemzar ASCO annual meeting 2005, abstr no. 1
Biliary tract cancer
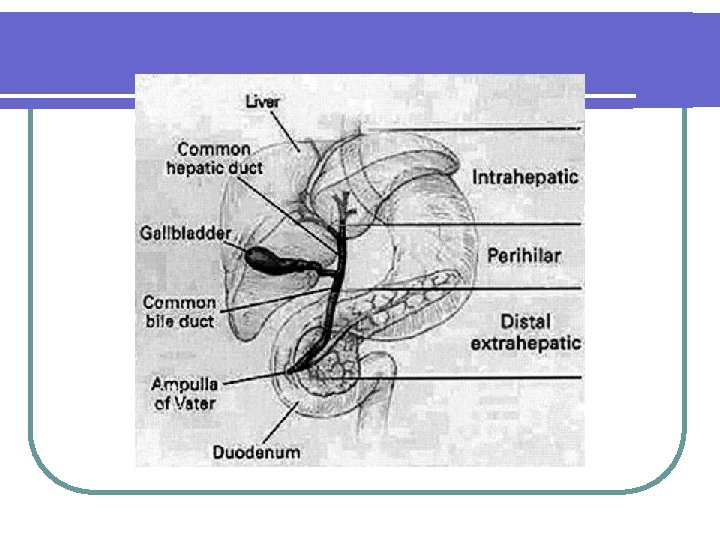
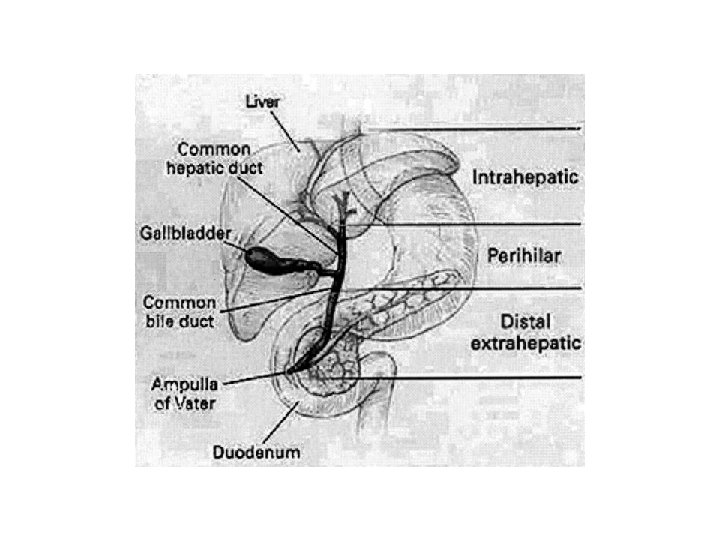
Classification l Cholangiocarcinoma l All tumors arise from bile duct epithelium l Mostly adenocarcinoma Intrahepatic (6%) l Hilum (67%): Klaskin’s tumor l Distal extrahepatic (27%) l Gall bladder l
Epidemiology l Old age: median 65 year-old l Slightly more in men l Uncommon cancer l Uncertain nature course and treatment
Risk factors l Chronic inflammation Primary sclerosing cholangitis : autoimmune l Choledochal cyst : congenital l Parasite l Stone : maybe l Repeat inflammation, stricture l Young age-onset l l Carcinogens
Pathology l Adenocarcinoma: 95%, most l CK 20(-), CK 7(+) l Squamous cell, small cell, sarcoma, lymphoma l CK 20(-), CK 7(+) l l Cholangio. Ca, pancreatic Ca, lung adeno. Ca CK 20(+), CK 7(-) l Colon cancer
Growth pattern l Nodular type Intrahepatic l Differential diagnosis of hepatic tumor l l HCC, cholangio. Ca, metastatic tumor l Sclerosing type Hilum and distal l Growth along the bile duct, difficult to diagnosis l
Clinical manifestation l Painless jaundice Early in hilum/distal type l Late in intrahepatic type l l Abnormal ALP/GGT l Weight loss, nausea/vomit l Palpable liver l Intrahepatic type l Biliary l tract infection Due to obstruction
Clinical manifestation l Tumor l markers Elevated serum CEA and CA 19 -9
Diagnostic evaluation l CT l scan, ultrasound For painless jaundice, to exclude stone l ERCP (Endoscopic Retrograde Cholangio. Pancreatography) Biliary tree evaluation l Intervention: stenting, brushing cytology l l MRI/MRCP l Non-invasive entire biliary tree evaluate
Extrahepatic Cholangiocarcinoma T 1 confined to the bile duct T 2 invades beyond the wall of the bile duct T 3 invades the liver, gallbladder, pancreas, and/or unilateral branches of the portal vein or hepatic artery T 4 Invades any of the following: main portal vein or its branches bilaterally, common hepatic artery, or other adjacent structures, such as the colon, stomach, duodenum, or abdominal wall N 1 Regional lymph node metastasis M 1 Distant metastasis Stage IA T 1 N 0 M 0 Stage IB T 2 N 0 M 0 Stage IIA T 3 N 0 M 0 Stage IIB T 1–T 3 N 1 M 0 Stage III T 4 Any N M 0 Stage IV Any T Any N M 1
Intrahepatic Cholangiocarcinoma T 1 Solitary tumor without vascular invasion T 2 Solitary tumor with vascular invasion or multiple tumors none >5 cm T 3 Multiple tumors >5 cm or tumor involving a major branch of the portal or hepatic veins T 4 Tumor(s) with direct invasion of adjacent organs other than the gallbladder or with perforation of visceral peritoneum N 1 Nodal metastases to the hepatoduodenal ligament M 1 Any distant metastases Stage I T 1 N 0 M 0 Stage II T 2 N 0 M 0 Stage IIIA T 3 N 0 M 0 Stage IIIB T 4 N 0 M 0 Stage IIIC Any T N 1 M 0 Stage IV Any T Any N M 1
Treatment l Surgery: mainstay Biliary tree evaluation for resectability l Intrahepatic: hepatic resection l Extrahepatic: may require pancreaticoduodenectomy, morbidity l l Prognosis: not clear, due to rarity
Multimodality treatment l Pre-op l neoadjuvant tx RT, C/T, CRT no benefit l Post-op l adjuvant tx RT, C/T, CRT no benefit A trial suggest adjuvant C/T may benefit GB ca l Adjuvant CCRT for locally advance dz? l
Locally advanced disease l CCRT, can be considered 5 FU/LV l Good performance l Liver toxicity, GI toxicity l l Palliative chemotherapy
Palliative chemotherapy l Pooled analysis, extra- and intra-hepatic l 5 FU/LV remained mainstay Infusion, bolus l RR: 20%-30% l Survival 6 -7 m l l Combination: Traditional: cisplatin, mitomycin l Newer agents: gemcitabine, taxane l
Palliative procedure l Biliary stenting, PTCD l Complication of biliary stenting Communicate bile duct and intestine l Bile is sterile l Resultant repeat infection (BTI) l