Pancreas divisum Chronic calcifying pancreatitis Case report Akos








")











 9 yrs")




")
")









- Slides: 43
Pancreas divisum + Chronic calcifying pancreatitis Case report Akos Pap National Institute of Oncology 2010
Interactive questions Success-rate of endotherapy in CP: 1. 2. 3. 4. 20 -30 % 40%0 % 60 -70 % 80< %
Interactive questions Success- rate of surgical decompression in CP: 1. 2. 3. 4. 20 -30 % 40 -50 % 60 -70 % 80< %
Interactive questions Which is first? 1. Surgery 2. Endotherapy 3. Either
Interactive questions Complication- rate of endotherapy: 1. <10 % 2. 10 -20 % 3. 30 -40 %
Interactive questions Complication- rate of surgery: 1. <10 % 2. 10 -20 % 3. 30 -40 %
Case report I. • 61 year old male-heavy alcohol consumption + smoking for 26 -38 years • 1975 cholecystectomy • 1976 acute pancreatitis with fluid collection - surgical cysto-duodenostomy • 1979 acute pancreatitis – choledochoduodenostomy • 1992 Sept. epigastric pain
Case report II. • 1992 Dec. Lundh test: no exocrine insufficiency, glucose loading: 4. 4 -7. 7 -7. 5 -8. 1 -10. 1 mmol/l • US + CT: obstructive pancreatitis with 5 mm diameter dorsal pancreatic duct, enlarged parenchyma, no calcification. • ERCP: duodenal compression with enlarged pancreatic head, swollen parapapillary duodenal mucosa, unsuccessful cannulation of the papilla, normal biliary outflow through the large choledocho-duodenostomy
Case report III. • 1993. Ápr. ALP: 380 U/l, GGT: 278 U/l (chronic cholangitis) • US: Chronic obstructive pancreatitis • ERCP: no pancreatic duct opacification, suprapapillary stricture of common bile duct with large choledocho-duodenostomy – biliary papillotomy + stenting with a 8 F teflon drain • At 6 months endoscopic stent removal • No severe relapse during 10 years
Case report IV. • 2004 Aug. acute relapsing pancreatitis • CT: parapapillary inflammation + calcification, moderate proximal pancreatic duct dilatation • Non-insulin dependent diabetes mellitus. ALP: 447 U/l, GGT: 178 U/l • Unsuccessful ERCP in another institution
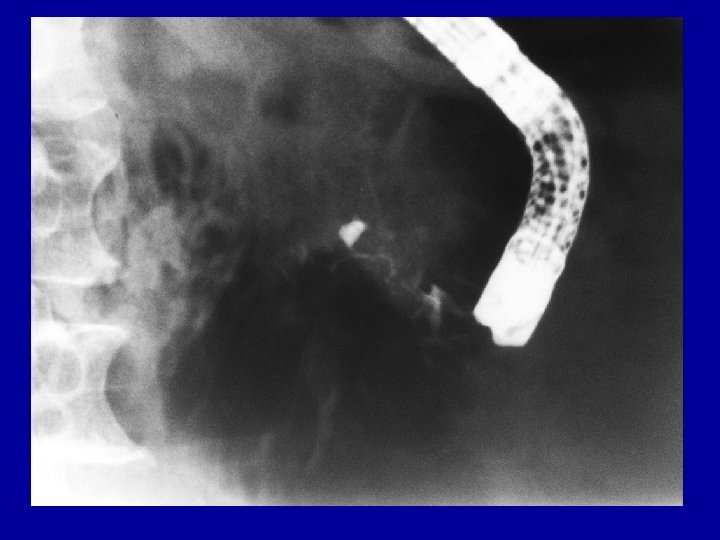
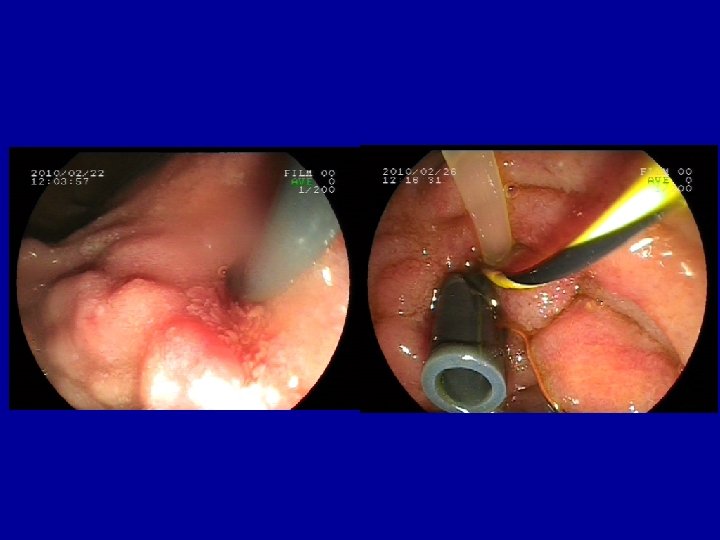
Case report V. • 2004. Okt. ERCP: suprapapillary stricture of common bile duct with normal outflow at the choledocho-duodenostomy, P. divisum • Patulous secondary papilla with suprapapillary stenosis of the dorsal duct • Secondary papillotomy with needle-knife, dilation + 8 F pancreatic stent with jejunal feeding tube. • 2004 Nov. dilation + 10 F pancreatic stent into the dorsal duct (double stenting 8 F + 10 F)
Case report VI. • 2005 Ápr. Elective endoscopic removal of pancreatic stents • 2008 Ápr. US: no ductal dilatation mild parapapillary calcification • ALP: 394 U/l, GGT: 117 U/l, glucose: 10, 6 mmol/l, CRP: 5 mg/l • 2009 Nov. ALP: 367 U/l, GGT: 110 U/l, glucose: 9, 2 mmol/l, CRP: 5 mg/l • No relapse of chronic pancreatitis (Degenerative eye problem).
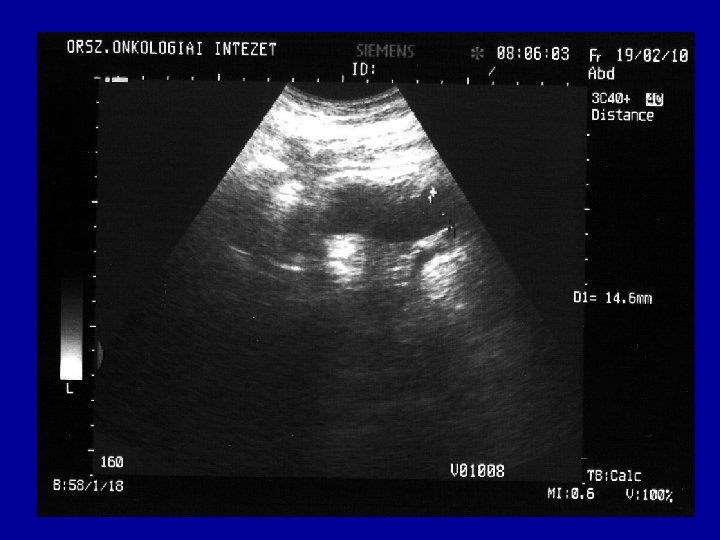
Case report VII. • 2010 Jan. Moderate pain, chronic cholangitis • ALP: 542 U/l, GGT: 205 U/l, glucose: 9, 3 mmol/l, CRP: 66 mg/l • US: Progressive parapapillary calcification, dorsal pancreatic duct 14 -18 mm with some parenchymal inflammation in the head of pancreas • Fatty liver with portal inflammation
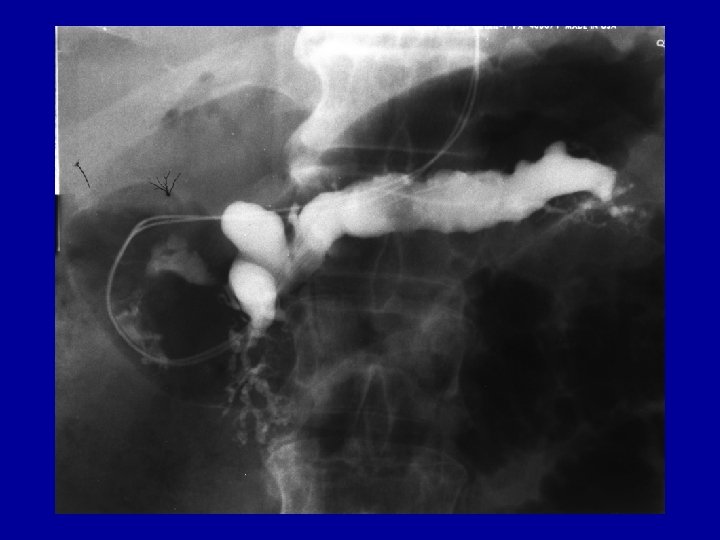
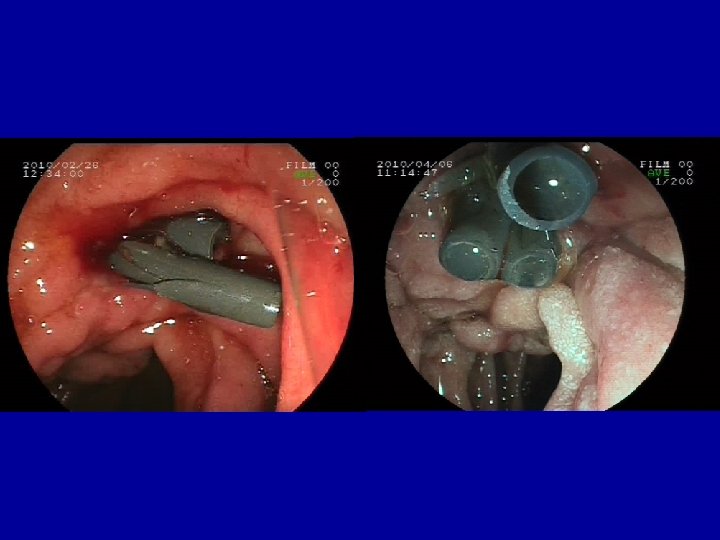
Case report VIII. • 2010 Febr. ERCP: Pancreas divisum with unequivocal changes in the ventral ducts. • Patulous secondary papilla with suprapapillary restenosis and distal dilatation of dorsal duct, • Dilation, 10 F pancreatic stent + 5 F nasopancreatic catheter with citrate lavage for 3 days followed by another 10 F stent placement into the dorsal duct
Case report IX. • 2010 Apr. another 10 F pancreatic stent to calibrate stenosis equilibrating prestenotic dilatation (10 mm=3 x 10 F), • no pain at dilation and further on. • Planned removal after 6 month
Temporaly loss of endotherapy against surgical treatment q Prospective, randomized, open label Dutch study, 2 -years follow-up q Longitudinal Wirsungo-jejunostomy, in 75% partial or total pain relief q ESWL + multiple balloon dilations with stenting (3 monthly for 27 weeks) painless in 32% q Better quallity of life after surgery (also at the 6 th week) q No significant differences in complications, hospital stay, changes in pancreatic function (carbonhydrate metabolism and elastase) , exocrine function (p=0, 05) Cahen DL, Gouma DJ, Nio Y, Rauws EA, Boermeester MA, Busch OR, Stoker J, Laméris JS, Dijkgraaf MG, Huibregtse K, Bruno MJ. Endoscopic versus surgical drainage of the pancreatic duct in chronic pancreatitis. N Engl J Med. 2007; 356: 676 -8
Weak points of the study q The etical committee interrupted the study at the 19 th endoscopic and 20 th surgical treatment q 3 of the 4 patients previously failed by endoscopy, also failed by surgery but included only in the endoscopic group q Jacques Deviere: „the results are manipulated” • (2 pseudocysts not mentioned among the 16 ESWL cases) q Old technique (stent exchange at every 3 rd month + balloon dilation, 27 weeks short-term treatment)
Successful endotherapy series q 89% painless after ESWL + stent implantation Weber A, Schneider J, Neu B, Meining A, Born P, Schmid RM, Prinz C. Endoscopic stent therapy for patients with chronic pancreatitis: results from a prospective follow-up study. Pancreas. 2007; 34: 287 -94. q 23 -months„on demand” stent replacement q. After 5 -years follow-up 52 -62% absence of pain Delhaye M, Devière J. Letter to the Editor Endoscopic versus Surgical Treatment for Chronic Pancreatitis Correspondence N Eng J Med 2007; 356: 2101 -2104
Comparison of surgical and endoscopic therapy q Pancreatic duct obstruction and pain q Endotherapy vs. surgery (resection (80%), drainage (20%)) q 140 eligible pts, only 72 agreed to be randomized q Endotherapy: sphincterotomy+stenting (52 %), stone removal (23 %) q Initial success rates: similar q 5 -year follow-up q Complete absence of pain (37 % vs. 14 %) Partial relief (49 % vs. 51 %) (randomized subgroup: 34 % vs. 15 % , 52 % vs. 46 %) q Increase in body weight: 20 - 25 % in the surgical group q New-onset diabetes (34 - 43 %), Dite P, Ruzicka M, Zboril V, Novotny I. : A prospective, randomized trial comparing endoscopic and surgical therapy for chronic pancreatitis. Endoscopy. 2003; 35: 553 -8
Endoscopic stenting for CP q 8 centers follow-up after 2 - 12 years (mean 4. 9 years) 1018 of 1211 patients (84%) q structured questionnaires; no pain or only weak pain q strictures (47%), stones (18%), strictures plus stones (32%) q 60% endotherapy completed, 16% still receiving endoscopic treatment q 24% had undergone surgery q long-term success of endotherapy 86% only 65% in intention-to-treat analysis q no significant differences between groups q pancreatic function not positively affected Rosch T, et al. : Endoscopic treatment of chronic pancreatitis: a multicenter study of 1000 patients with long-term follow-up. Endoscopy. 2002; 34: 765 -71.
Endoscopic stenting for CP q 93 CP patients with dominant sticture (ERCP) 9 yrs q Pain during 5. 6 yrs before treatment q Stent exchanges according symptoms during 16 mos q Pain relief: 74% (only partial: 1/3) q Lasting (5 yrs) pain relief 64% q 36/49 pts painless without stent (4 yrs) q 13/49 pts relapsed, 11/13 stented again q Complications: mild pancreatitis (4), abscess (2) Binmoeller et al Endoscopy 1995, 27: 638 q Problems: drain occlusion albumin, bacteria, calcium Smits et al Gastrointest Endosc 1997, 45: 52 q Ductal and/or parenchymal alterations ERCP + EUS 56%-68%, half remained Sherman et al Gastrointest Endosc 1996; 44 -276
What could be the reason of the low success-rate? q Low number of patients q 3 of the 4 patients who previously failed by endoscopy, then by surgery diminished response-rate of endotherapy but not that of surgery q Open labelled study: surgical treatment more definitive „the larger the scar, the smaller the pain” q After the endoscopy the surgical treatment still possible q Complications in the surgical group: 35% and 5% severe! q Editorial recommendation: First endoscopy, the second step could be a surgical treatment Elta G. H. Editorial Is There a Role for the Endoscopic Treatment of Pain from Chronic Pancreatitis? N Eng Med 2007; 356: 727 -729
Multiple stents for calibration of pancreatic strictures in chronic pancreatitis. Á Pap, M Burai, T Gyökeres Z. Gastroenterol 2006, 3: 130 -135 Multiple stenting of refractory pancreatic duct strictures in severe chronic pancreatitis: long-term results. Costamagna G, Bulajic M, Tringali A, Pandolfi M, Gabbrielli A, Spada C, Petruzziello L, Familiari P, Mutignani M. Endoscopy. 2006. 38: 254 -9.
Rational for multiple stenting • Patency increased by multiplying internal diameter of stents + space between outer surface and ductular wall • Free outlet of branch ducts assured by space between stents and the ductular wall • Definitive calibration of stenosis to 2/3 of the distal dilatation
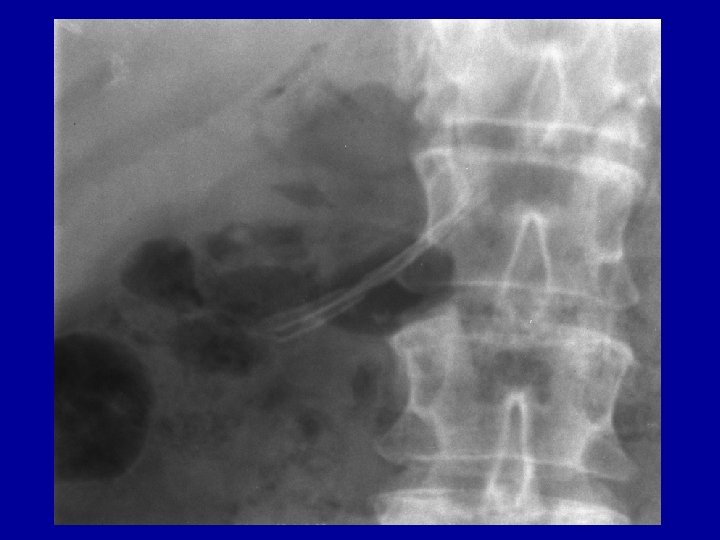
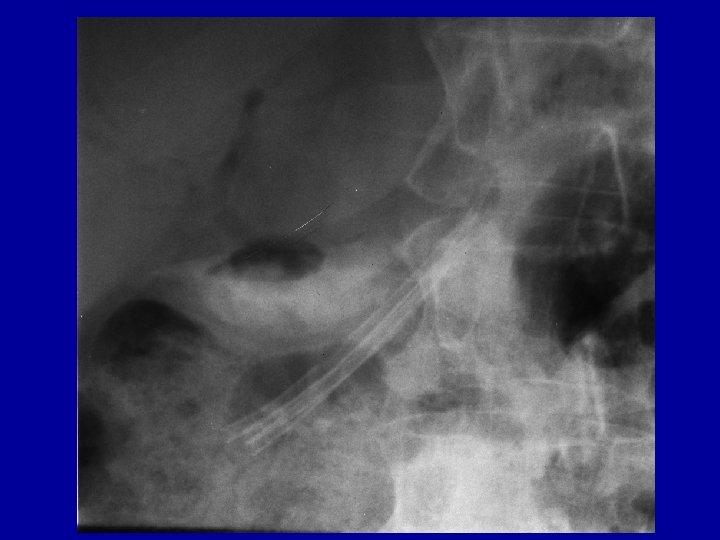
Multiple biliary and pancreatic stents with guidewire in the papilla
Results I. One stent group Multiple stent group n= 13 patients (16 cases) 12 patients (16 cases) age 56. 3 (50 -78) years 52. 7 (42 -58) years gender 1 female, 12 male 1 female, 11 male stenting time 3. 3. (1 -18) months 5. 5 (1 -18) months 31. 6 (8 -65. 5) months 41. 9 (5 -80) months nasopancreatic citrate lavage 7 10 ESWL 5 3+1 stone removal supplementary biliary stenting 2 5 painfull relapses due to alcohol and/or smoking 7 7 surgery 2 0 repeated stenting 1 5 death (unrelated) 2 2 follow-up
Biliary and pancreatic stents in the corresponding ducts Pancreatic lavage with citrate (1. 9%) at 1 -2 ml/min for 3 -5 days
Results II. q. No complication occurred at stenting, no new-onset diabetes developed. q. Relapse-free follow-up occurred for 31. 6 and 41. 6 months (range 8 -80) in one stent and multiple stents groups, respectively until now. Increasing the stent number prolonged the relapse free period in 2 pts. q Relapses (7 -7 cases) were provoked by alcohol, smoking and heavy meals and treated mainly by multiple stenting (6 cases) or operation (2 patients).
Multiple stenting of refractory pancreatic duct strictures in severe chronic pancreatitis: long-term results. Costamagna G, Bulajic M, Tringali A, Pandolfi M, Gabbrielli A, Spada C, Petruzziello L, Familiari P, Mutignani M. Endoscopy. 2006. 38: 254 -9. q 19 patients with severe chronic pancreatitis (16 men, three women; mean age 45 years) with a single pancreatic stent refractory dominant stricture q balloon dilation of the stricture; insertion of the maximum number of stents allowed by the stricture q removal of stents after 6 to 12 months q only one patient (5. 5 %) had persistent stricture after multiple stenting q mean follow-up : 38 months q asymptomatic 84 % , symptomatic stricture recurrence 10, 5% q no major complications
Conclusion q Multiple pancreatic stenting with progressive calibration of stenosis can dilate the stricture without rupture, ischemia and side brach obstruction caused by aggressive balloon dilation q The relapse- free period could be prolonged also without stent in place if alcohol consumption and smoking have been stopped definitely q A well controlled, randomised study should be necessary to demonstrate advantages of multiple pancreatic stenting in comparison to surgery.
Interactive questions Success-rate of endotherapy in CP: 1. 2. 3. 4. 20 -30 % 40%0 % 60 -70 % 80< %
Interactive questions Success- rate of surgical decompression in CP: 1. 2. 3. 4. 20 -30 % 40 -50 % 60 -70 % 80< %
Interactive questions Which is first? 1. Surgery 2. Endotherapy 3. Either
Interactive questions Complication- rate of endotherapy: 1. <10 % 2. 10 -20 % 3. 30 -40 %
Interactive questions Complication- rate of surgery: 1. <10 % 2. 10 -20 % 3. 30 -40 %