Palliation With Endoluminal Stents Todd H Baron M

Palliation With Endoluminal Stents Todd H. Baron, M. D. , F. A. C. P. Professor of Medicine Gastroenterology & Hepatology Mayo Clinic College of Medicine
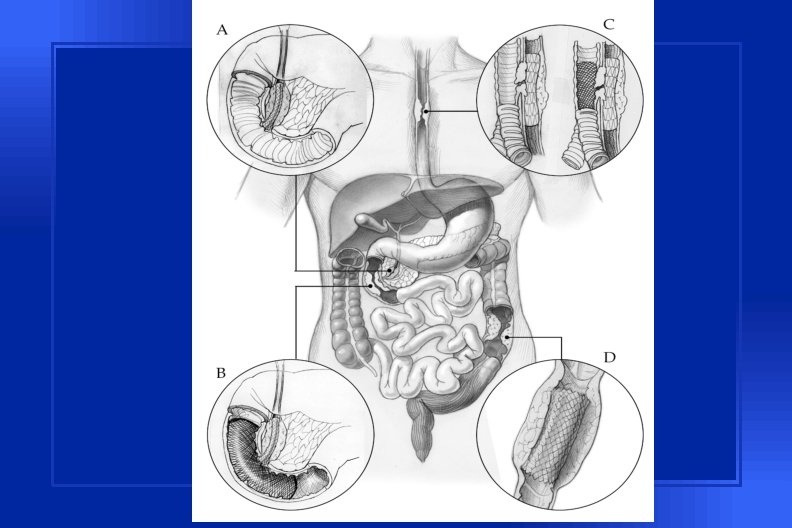

Enteral Stents

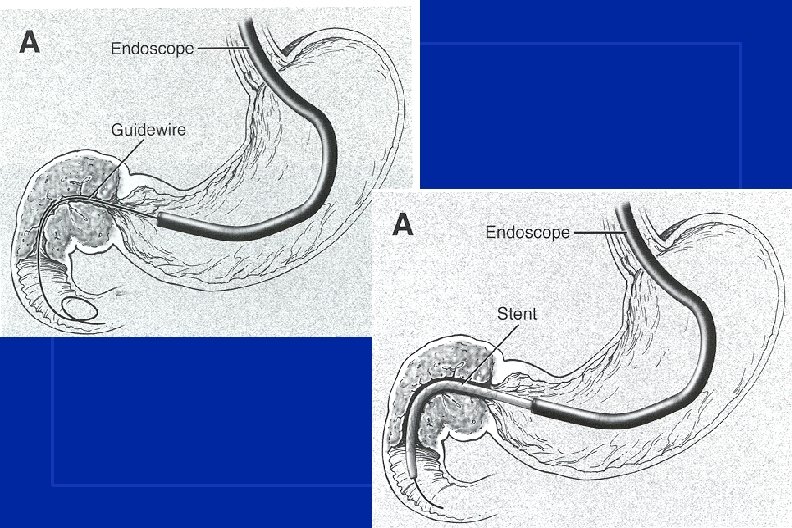
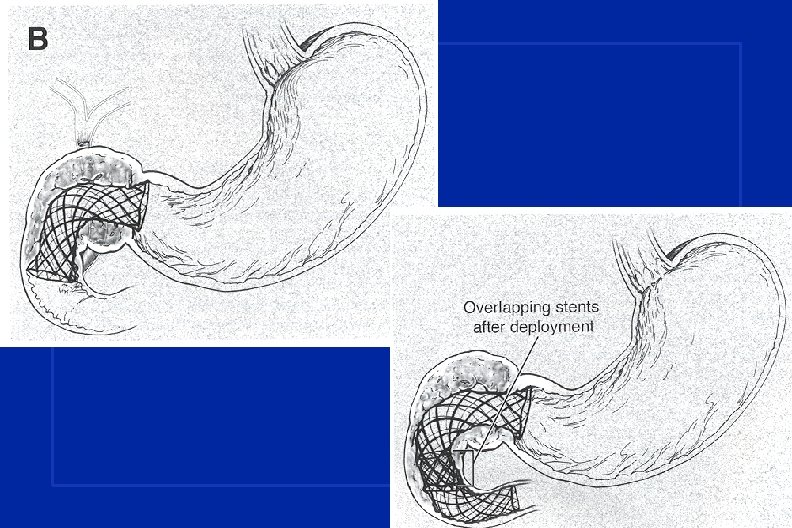
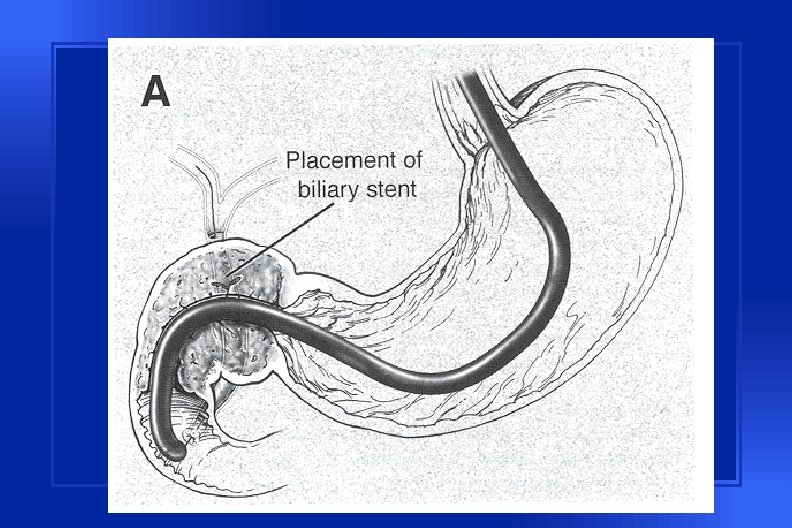
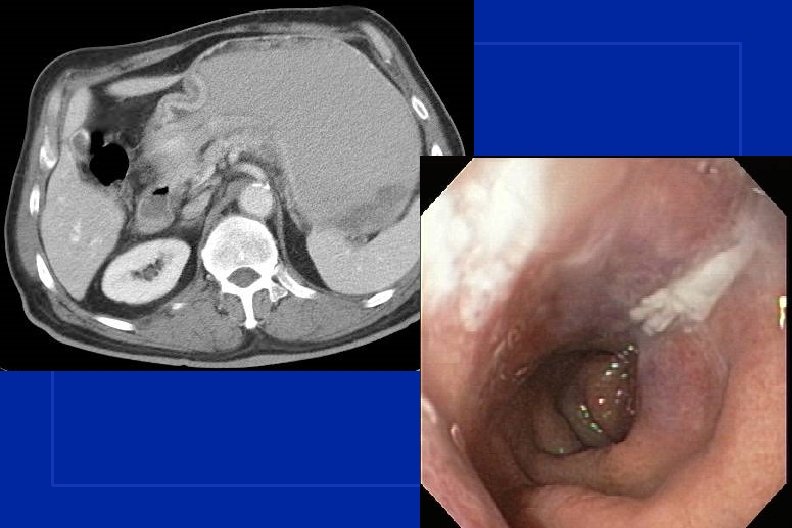
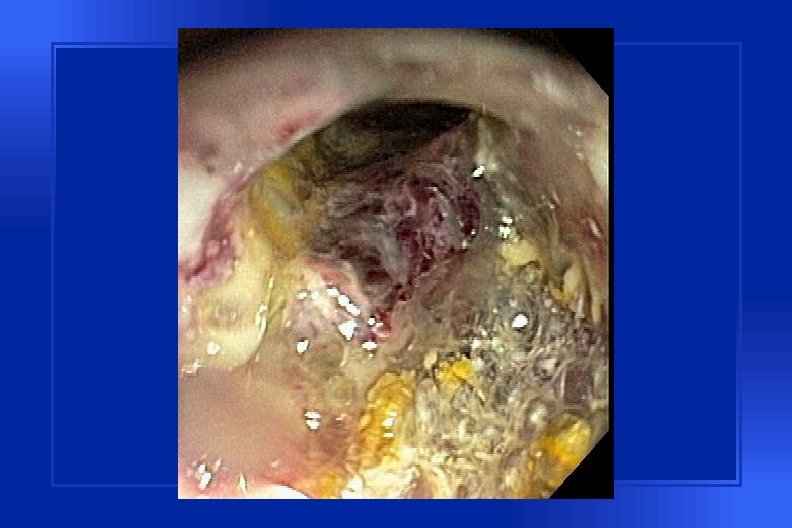
Malignant Gastric Outlet Obstruction

Clinical Situations • Unresectable CA pancreatic, GB, Cholangio • Metastatic disease • Local invasion - colon • Gastric CA • primary • Recurrent

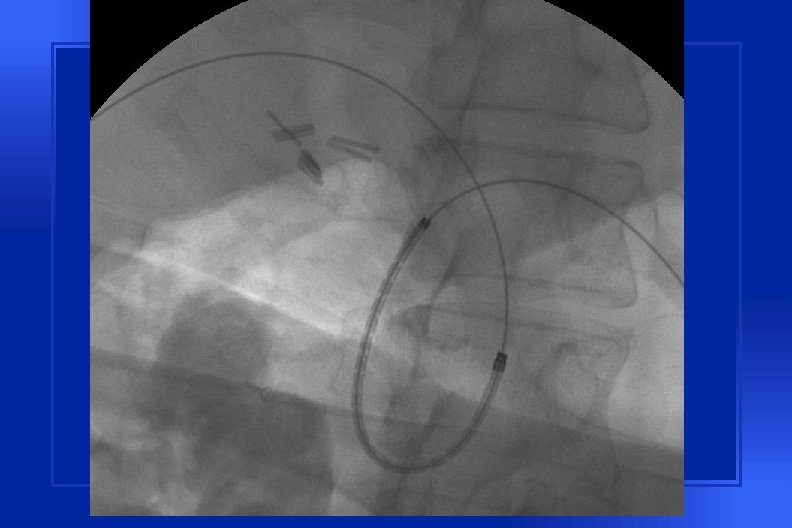
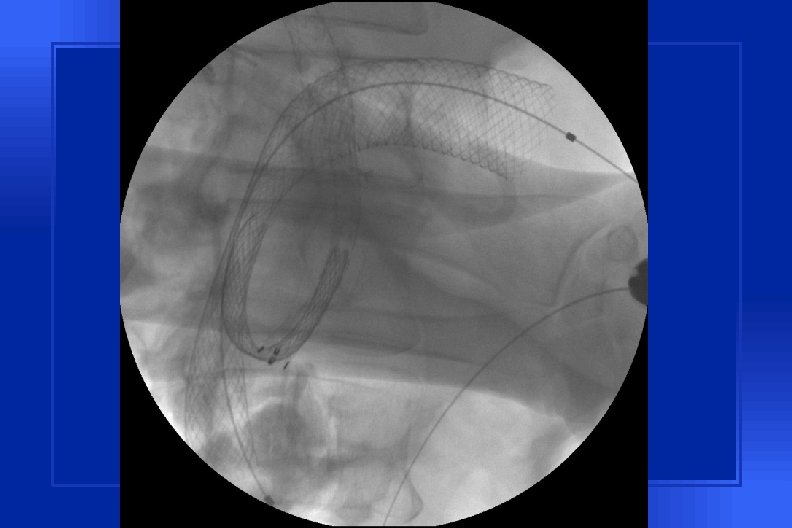
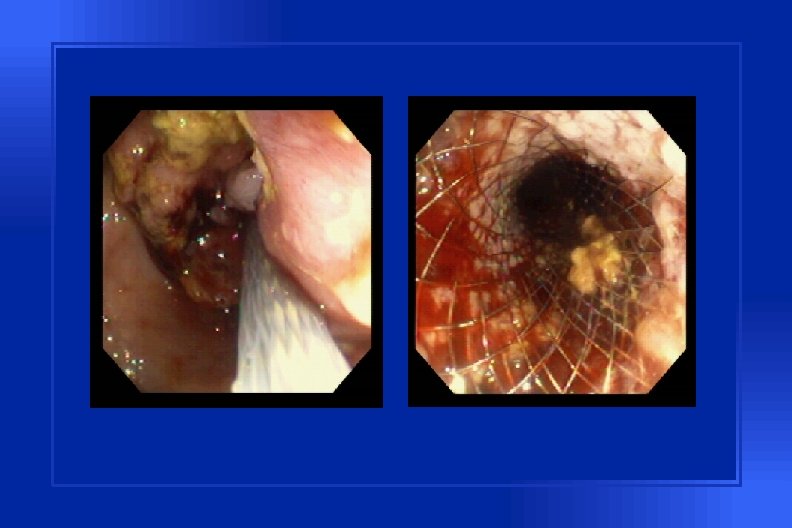
SEMS: Overview • May be placed endoscopically or radiologically • Non-TTS difficult but possible • TTS placement - can be placed beyond ligament of Treitz uncovered

Wallstent • Delivery diameter: 10 F • Deployed diameter: 20 mm 22 mm • TTS



Cost of Palliation: Pancreatic CA ENDO GASTRO-J Number of patients 12 15 Median survival (days) 94 92 NS Median charges incurred $9921 $28, 173 < 0. 005 Median hospitalization stay required (days) 4 14 < 0. 005 Number requiring repeat procedures and hospitalization 7 (58. 3%) Yim, et al. , GIE, 2001 15 (100%) p



Malignant Colorectal Obstruction

Metal Colonic Stents • Wilson-Cook Z stent • Microvasive Wallstent • Precision Ultraflex Colonic OTHER • Ultraflex Esophageal Stent
 • Deployed diameter: 35/25 mm")
Colonic Z-Stent • Delivery diameter: 10 mm (30 F) • Deployed diameter: 35/25 mm

Indications for Colorectal Stents • Pre-operative • Palliative • Indeterminate
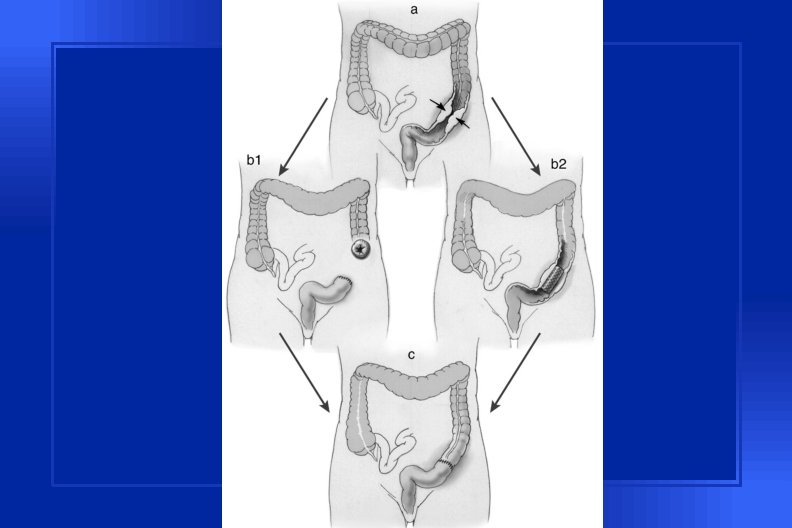

Potential Benefits of Pre-operative Colon Stents • • • One-stage operation Reduced costs Improved QOL Elective operation Pre-operative assessment tumor resectability patient operability

Complications of Enteral Stents • • • Tumor ingrowth/overgrowth Migration Perforation immediate delayed Impaction Bleeding Pain/Tenesmus

Conclusions • SEMS are effective for closing TEF and treating all forms of malignant esophageal obstruction • SEMS are cost-effective for palliation of malignant GOO for pancreatic CA • SEMS can be used for both preoperative and palliative treatment of malignant colonic obstruction
- Slides: 28