Pain Physiology of Pain l l Nociceptors Stimulus





















 l Psychophysiological disorders“ l “Psychoneurotic Disorders” l II")
 l Psychogenic Pain l “incompatible” or “INXS” l")

















 √ Hydromorphone (Dilaudid) √")


















- Slides: 60
Pain
Physiology of Pain l l Nociceptors Stimulus Transmission Termination Modulation
Physiology of Pain l l Multiple Redundant Reciprocal Complex
Assessment of Pain Immediate Pain l Physical Functioning l Psychological Factors l Pain Behaviors l Objective Correlates l
Assessment: Immediate Pain Intensity l Location l Affective Response l Composite Measures l
Assessment: Physical Fx. Impairment l Functional limitation l Disability l
Assessment: Psych factors Influence vs. causation l Mediation l Reinforcement l Resonators l Pain beliefs l
Assessment: Pain Behavior Observation l Role of learning l
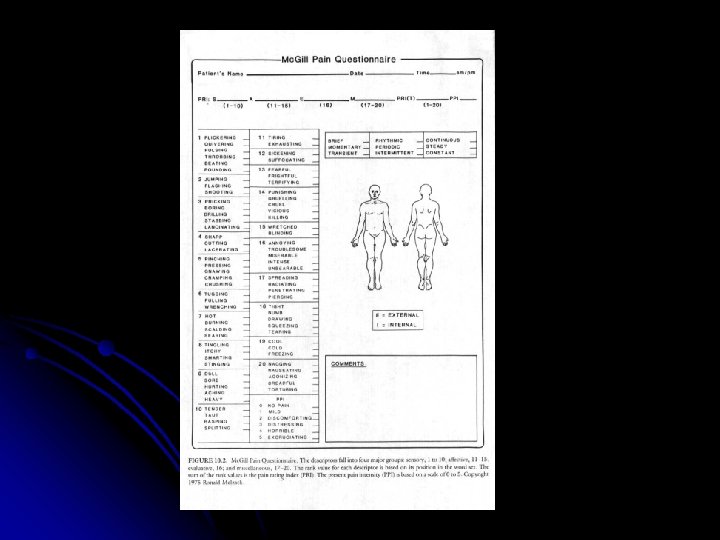
Composite Pain Scales l Attempt to measure one or more dimensions of the pain experience
History Intensity Quality Objective Data Comorb id Side effects
Assessment: Objective Indicators l Ex. Electromyography “Well, Phil, after years of vague complaints and imaginary ailments, we finally have something to work with. ”
Diagnosis Categorization l DSM and Pain l Other Approaches to “Somatoform Pain” l
Categorization l Acute versus Chronic
Acute Pain Not just time l Clearer association l l Subtypes l (ex. Recurrent? ) “nociceptive pain”
Chronic Association? l Types l l By presumed etiology l Neurologic l Ideopathic l By course pain
DSM-IV The concept of Somatoform Pain
DSM and pain l I (1952) l Psychophysiological disorders“ l “Psychoneurotic Disorders” l II (1968) l Hysterical neurosis
DSM and pain l III (1980) l Psychogenic Pain l “incompatible” or “INXS” l Etiologically related l III-R (1987) l Somatoform pain l Dropped etiology part
DSM and pain l IV l Pain Disorder l Pain=predominant focus l Substantial distress/impairment l Psych factors “have role” l Onset or expression l Not malingering/factitious disorder
Problems with DSM l l Utility How to judge? l l l Physical versus Psychological Etiology DSM-IV l l Mind-body dichotomy remains Division of pain based on this.
True psychogenic pain
DSM-IV pain tested l Psychological vs. Psychological+Medical Distinction l No difference on l Pain measures l Intensity l Type l Level of disability (Aigner et al, Compr Psychiatry 1999)
Other approaches to diagnosing pain
IASP 5 axis system I. III. IV. V. Anatomical region Organ system Temporal characteristics/patterns Intensity, time since onset Etiology
IASP l Psychological pain l “Pain specifically attributable to the thought process, motional state, or personality of the patient in the absence of an organic or delusional cause or tension mechanism. ”
Other approaches l Dimensional l Take into account various aspects of pain l Objective findings/physical etiology l Perceptual influences l Presentation
Treatment of Pain
Treatment of Pain Pharmacologic l Psychological l Other somatic treatments l Importance of Multimodal l Cormorbid treatments l Role of C/L Psychiatrist l
Pharmacological Treatment l l “True” Analgesics Everything Else “Yes Billy, but Mr. Phillips pushes legal drugs. ”
“True” Analgesic NSAIDS l Opioids l Local agents l
NSAIDS Mechanism l Indication l Side effects l
NSAIDS Standard l Acetaminophen l Ketorolac l COX-2 inhibitors l
Opioids Mechanism of action l Indication l Side effects l l Common l Uncommon but problematic
Some Typical Opioids Oral Paren Morphine √ √ Propoxyphene (Darvon) √ Hydromorphone (Dilaudid) √ √ Meperidine (Demerol) √ √ Methadone √ √ Tran √ Oxymorphone (Numorphan) Fentanyl (Duragesic, Actiq) √* Oxycodone (Percoset, Oxy--) √ √ √
Combination Opioid/NSAIDs Narcotic +Acet Dihydrocodone DHC plus* Propoxyphene Darvocet, Wyegesic Codeine Tylenol w/ Codeine #2 - Fiorinal*† 4, Fiorecet*† Hydrocodone Vicodin, Hydrocet, Lortab, Zydone Oxycodone Percocet, Tylox Pentazocine‡ Talacen *caffeine † butalbital ‡agonist-antagonist +ASA +Ibu Vicoprofen Percodan
Relative Potency
Treatment Approach
Treatment Approach MEC l Role of pharmacokinetic l l Toxicity l Slow-release preps
Concerns l l l Tolerance Dependence Addiction
Overvalued Concerns l l l Addication Overdose and death Discipline “Damn! I suppose this means another malpractice suit. !”
Adjunctive and other meds l l l Antidepressant Anticonvulsants Local Analgesics Antihistamines Antipsychotics l l Benzodiazepines Stimulants Cannabinoids Placebos
Nonsurgical treatments Cutaneous Stimulation l Electrical Stimulation l Acupuncture l Exercise l
Surgical Treatments Neural Blockade l Surgical lesions l Limitations l
Psychological Treatments Psychoeducation l Hypnosis l Behavioral Treatments l
Behav Txs Relaxation l Biofeedback l CBT l l Focus l Goals
Multidisciplinary Pain Treatment l Different levels l Features included
Comorbid Problems Depression l Anxiety l
Problems of dual diagnosis
Role of Psychiatrist in Pain Mgmt
Role of C/L Psychiatrist in Pain Eval l “Problem Patient” l “Drug Seeker” l “Just in their heads” l “Pain out of proportion…”