Pain Management for patients with Sickle Cell Disease





 hallmark acute complication –")






 ED • Ave. pain scores on discharge")












 •")
 •")






. Neuropathic pain in patients")


- Slides: 37
Pain Management for patients with Sickle Cell Disease: Acute and Chronic Pain Education Series Natalie Madar ARNP,
Pain Physiology 2
Chronic Pain in SCD • Defined as pain greater than or equal to 3 X per week over past 3 months 3
Sickle Cell Disease • Inherited blood disorder involving an abnormality of hemoglobin, leading to numerous painful syndromes. – The pain can be somatic, visceral, acute, chronic, persistent, or recurrent. – Vaso-occlusive episodes account for 79 -91% of emergency room visits and 59 -68% of hospitalizations in patients with sickle cell disease (SCD) (Freiermuth et al. , 2014). 4
Pain in Sickle Cell Disease • Two types of SCD pain: – The vaso-occlusive crisis (VOC) – also known as a “sickle cell crisis”; an attack of acute pain due to vaso-occlusion that is the “hallmark symptom” of the disease – Chronic Pain : Due to accumulation of organ/tissue damage over time…may also be due to chronic levels of vaso-occlusion 5
Acute Pain in Sickle Cell Disease • VOC (Vaso-occlusive crisis) hallmark acute complication – severe pain – Sudden vs gradual – Commonly occur extremities, chest, back – Hv. SS or Hb. SB more frequent 6
Acute Pain in Sickle Cell Disease • As of this time, there are no objective indicators that can be used to reliably indicate the presence &/or severity of a VOC • The patient’s self-report is the gold-standard by which a VOC is identified • Pain Management must be guided by patient report of pain severity 7
Sickle Cell Pain Phases 1. Pre-pain or prodromal 2 -4 days pain described as low intensity or aches Teach to recognized clues by keeping diary of symptoms 2. Initial or infarctive Pain more intense and difficult to treat Decreased activity Fear and anxiety about seeking care 8
Sickle Cell Pain Phases 3. Established Pain at peak, steady, persistent No relief from home medications Seek care via ER Lasts 4 -6 days Joints swollen/stiff Often requires hospitalization 9
Sickle Cell Pain Phases 4. Resolving, recovery, or post crisis Pain is now tolerable Usually last 1 -2 days 10
Best Practice Guidelines • Rapid Clinical assessment • Age appropriate pain scale • Pharmacologic management (prescribed by the medical team) • Ongoing monitoring until pain stable/controlled • Hydration 11
Treating Acute Pain in Sickle Cell Disease • Opioids – Severe pain every 2 -4 hours, around clock dosing – IVPCA – Reassessment and titration of dose • Non opioid – NSAIDs when not contraindicated – Acetaminophen 12
ED vs Acute Care Unit (Molokie, 2018) ED • Ave. pain scores on discharge 6. 4 • 70% admitted • Dose of initial and hourly opioid lower than ACU Acute Care Unit • Ave. pain scores on discharge 4. 5 • 37% admitted • Dose of initial and hourly opioid higher than ED 13
Chronic Pain in Sickle Cell • seen in 23% of children with SCD • Etiology often unclear • Avascular necrosis • Neuropathic pain caused by 1. tissue damage due to ischemia to nerves 2. inflammation 14
15
Central Sensitization Definition: The nervous system goes through a process called wind-up and gets regulated in a persistent state of high reactivity. 16
Central Sensitization Two Characteristics: 1. Heightened sensitivity to pain hyperalgesia Amplify 2. Heighted sensitivity to touch allodynia 17
Central Sensitization Carrol et al in 2016 studied adult SCD on chronic opioid therapy (COT) and compared to no use of COT had greater levels of clinical pain (particularly non crisis), central sensitization, depression, less function and increase healthcare utilization on crisis and non crisis days. 18
Factors affecting pain • • • Tolerance of dosing Hyperalgesia Depression Anxiety Feeling of despair Insomnia • Lack of support • Poor coping skills • Inappropriate therapeutic expectations • Loneliness • PTSD 19
Treating Chronic Pain in Sickle Cell Disease • • Antidepressants Clonidine Gabapentin Pregabalin • Hydroxyurea • Prevention of crisis 20
Non Pharmacological techniques – Distraction – Guided imagery – Meditation – Cognitive behavior therapy (CBT) – PT/OT – Healing touch – Massage – Acupuncture – Hypnosis – Biofeedback 21
Patient Pain Coping Behaviors • There is great variation in patient’s ability to cope with pain and in the expressions they exhibit while in severe pain • Patients may not express as much distress in their appearance as clinicians might assume given the patient’s reported level of severe pain • A patient with SCD is able to watch TV, talk on the telephone, talk with visitors, or appear relatively comfortable & still be in severe pain in need of aggressive treatment & close monitoring • These behaviors & responses to pain are a subset of the coping skills patients have developed from years of experiencing painful episodes
CASTROPHIZING • An exaggerated negative thoughts in response to experience or anticipated pain • • Perceived threat of pain causes heightened pain, emotional distress, pain related fear, and activity avoidance resulting in disability 23
CASTROPHIZING Poorly understood • Seen in pediatric chronic pain • reported increased pain intensity • functional disability • more school absences 24
CASTROPHIZING • Poor parental coping and increased parenting stress • Parents’ engagement in pain promoting behavior (poor coping, frequent health care use) 25
Pediatric Sickle Cell Disease and Parent and Child Castasrophizing (Sil et al. 2015) • Parent –child dyads important to assess on multiple levels • Cognitive behavioral therapy effective in improving daily function and reducing pain • Early identification for referral for behavior pain treatment 26
Pediatric Sickle Cell Disease and Parent and Child Castasrophizing (Sil et al. 2015) • Sample 100 children • Comparable with other pediatric chronic • Age 8 -18 (average pain conditions 13. 5 yo) • Higher levels of • Children Hosp in castastrophizing Southeast US associated with • Use of Pain greater disability Catastrophizing Scale 27
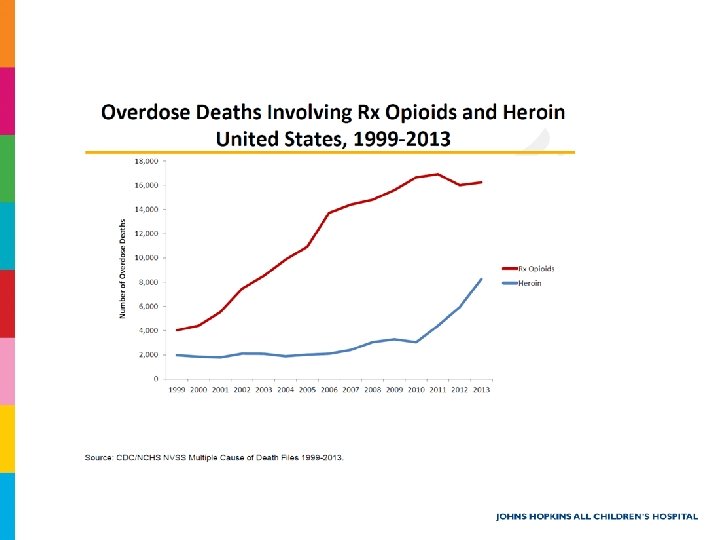
Opioid Epidemic
Addiction & Substance-Abuse among Patients with SCD • Clinician fears about contributing to, or causing, addiction to opioids among patients with SCD are a recognized barrier to the delivery of high quality pain management • Multiple research studies have found the prevalence of substance abuse and addiction among patients with SCD to be lower than, or at most the same as, that found in the general population
What you need to know • Patient-Provider goals and expectations on treatment outcomes • Proper Opioid and other controlled substance selection • Limit therapy duration and quantity # dispensed upon discharge • “E-forcse” Florida Prescription Drug Monitoring program – Link https: //flpdmpph. hidinc. com/fllogappl/bdflpdmqlog/pmquserlo gin. html
What you need to know • Encourage and discuss safe storage and disposal of prescribed narcotics. – Document education provided with patient/family in medical record. – Remind the patient of the dangers of prescription opioid diversion and the importance of secure storage of their medications. – Safe Disposal Resources • • FDA guideline DEA approved take-back program FDA Safe Disposal of Medicines End the Epidemic Retrieved from: https: //www. fda. gov/drugs/resourcesforyou/consumers/buyingusingmedicin esafely/ensuringsafeuseofmedicine/safedisposalofmedicines/ucm 186187. htm
What you need to know • Pharmacologic Alternatives – Non opioid analgesics for mild to moderate pain – Consider antidepressants (TCAs/SNRIs) and anticonvulsants for neuropathic pain – melatonin, TCAs, trazodone, or other noncontrolled substances if the patient requires pharmacologic treatment for insomnia • Non-pharmacological interventions – Massage, TENS unit, aromatherapy, meditation, guided imagery, PT/OT
JHACH Pain Management Department • Inpatient Acute Pain Service – 7 days a week, 71472, 71473, 71476 – Attending Physicians: • • • Allison Fernandez, M. D. Richard Elliott, M. D. Jenny Dolan, M. D. Will Nelson, M. D. Jibin Samuel, M. D. – Advanced Practice Nurses (A. R. N. P. ) • • • Kay Rhoades Natalie Madar Christine Georgeff Lauri Haffner Erin Cafiero Kristina Banks • Outpatient Chronic Pain Clinic – Fridays 1 -5 pm OCC 3 rd floor 727 -767 -PAIN
References • • • Antunes, F. B. et al. (2017). Neuropathic pain in patients with sickle cell disease: a cross-sectional study assessing teens and young adults. Annuals of Hematology. 96, 1121 -1125. Bader, M. K. , & Litttlejohns, L. (2016). American Association of Neuroscience Nurses Core Curriculum for Neuroscience Nursing 6 th Edition. Saunders. Bozimoski, G. (2012). Patient Perceptions of Pain management Therapy: A Comparison of Realtime Assessment of Patient education and Satisfaction and Registered Nurse Perceptions Vol 13 NOo 4. Pain Management Nursing, 186 -193. https: //www. google. com/search? safe=active&rls=com. microsoft%3 Aen-US%3 AIESearch. Box&biw=2133&bih=1044&tbm=isch&sa=1&ei=Kt. Sm. Wt 3 m. FIy 0 zw. K 9 w. Yzg. CQ&q=electricit y&oq=electricity&gs_l=psyab. 1. 0. 0 l 10. 3234. 5793. 0. 8542. 12. 8. 0. 4. 4. 0. 249. 1069. 0 j 6 j 1. 8. 0. . . 1 c. 1. 64. psyab. . 0. 1185. 0. . . 104. a. Wzf. Yez 4 Av. M#imgrc=xi. K 9 H 69 h 8 o. An 3 M: &spf=1520882739914 March 12 1530 Mookie, R. et al. (2018) Opioid doses and acute care utilization outcomes for adults with sickle cell disease: Ed versus acute care unit. . American Journal of Emergency Medicine, 36, 8892. 35
References. • • • Manito, C. , Kost-Byerly, S. , White, E. , Lee, C. , Rudek, M. , Thompson, C. , Yaster, M. (2011). The Optimal Dose of Prophylactic Intravenous Naloxone I Ameliorating Opioid-Induced Side Effects in Children Receiving Intravenous Patient-Controlled Analgesia Morphine for Moderate to Severe Pain: A Dose Finding Study. Anesthesia & Analgesia. Vol 113, 834– 42. Sil, S. , Damiper, C. , & Cohen, L. (2015) Pediatric Sickle Cell Disease and Parent and Child Catastrophizing. The Journal of Pain, 17(9). 963 -971. Sil, S. Cohen, L. & Dampier, C. (2016) Psychosocial and Functional Outcomes in Youth with Chronic Sickle Cell Pain. Clinical Journal of Pain, 32(6). 527 -533. Wilson, B. & Nelson, J. (2015) Sickle Cell Disease Pain Management in adolescents: a literature review. Pain management Nursing, 16(2), 146 -151. Williams, A. , Toye, C. , Deas, K. , Fairclough, D. , Curro, K. , & Oldham, L. (2012). Evaluating the Feasibility and Effect of Using a Hospital-Wide Coordinated Approach to Introduce Evidence. Based changes for Pain Management Vol. 13 No. 4. Pain Management Nursing, 202 -214. US health and Human Resources. (2014). Evidence- based management of sickle cell disease, expert panel report 36
Discussion/Questions