PAIN AND THE BRAIN A Biopsychosocial Approach to

PAIN AND THE BRAIN A Biopsychosocial Approach to Pain Management Jennifer L. Johnson, DNP, MSN, BSN, FNPC

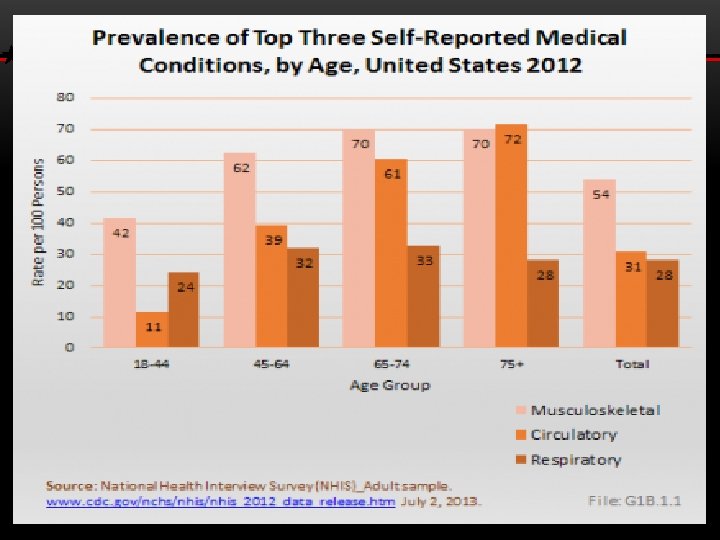
SCOPE OF THE PROBLEM 100 Million in U. S. with Persistent Pain § 42% with pain lasting over one year § 33% report pain as disabling § Second most common reason for outpatient visits $635 Billion Annual Costs § Healthcare expenses § Lost income American Academy of Pain Medicine (2015) www. painmed. org § Lost productivity Institute of Medicine. 2011 Relieving Pain in America. Washington D. C.

Background • 2016, 63. 1% opioid deaths related to prescription opioids • 20% higher than 2010 • 2016, leading cause of death in United States • Usefulness of opioids for treating pain is short term • Evidence demonstrated in end of life care • Limited evidence of benefit for long term pain (Dowell & Haegerich, 2016; US Department of Veterans Affairs, 2016 a, 2016; Burgess, Siddiqui, & Burgess, 2014; & Cheatle & Baker, 2014 Schell, 2017; Shorn, Doorenbos, Gordon and Read-Williams, 2014) management
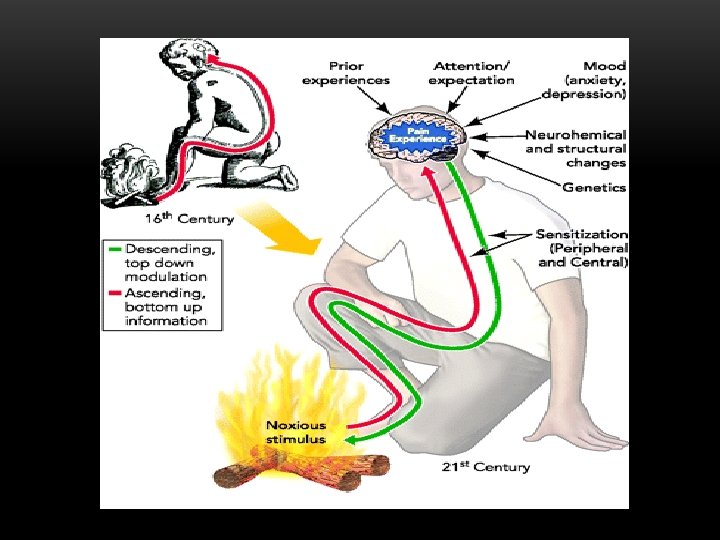
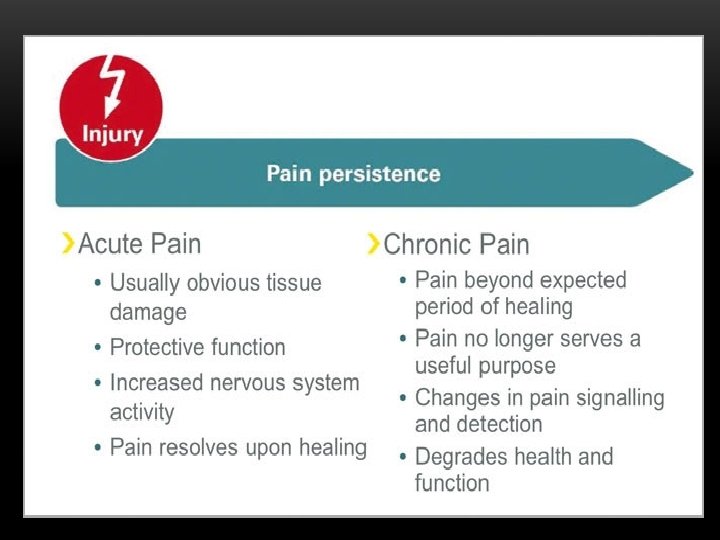

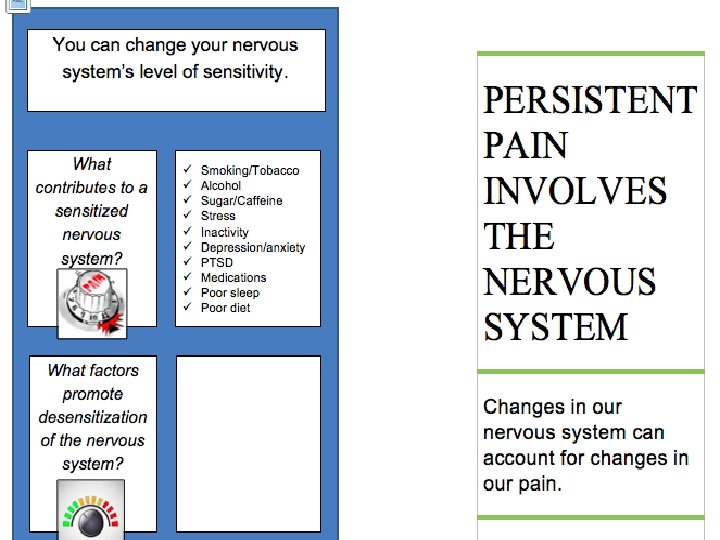
DEVELOPMENT OF CHRONIC PAIN

PRESCRIPTION OPIOIDS & ADVERSE OUTCOMES FOR THOSE WITH MENTAL HEALTH DISORDERS Receiving prescription opioids was associated with an increased risk of adverse clinical outcomes, particularly in those with PTSD § Wounds or injuries § Opioid-related accidents and overdoses § Self-inflicted injuries/Suicide § Violencerelated injuries Seal, KH, et al. JAMA.

CHRONIC PAIN AND PTSD: MUTUAL MAINTENANCE Disability Pain Anxiety/hyperarousal – � pain perception PTSD re-experiencing - evokes pain Dysregulated ANS/Endog. Opioid system PTSD Anxiety Adapted from Sharp TJ, Harvey AG. Clin Psychol Rev. 2001 Aug; 21

Biomedical Management of Chronic Pain

BIOMEDICAL MODEL OF PAIN CARE • Diagnostics to ID singular cause of pain • Interventions target peripheral tissues • Mind and body are separate • Passive interventions • Primarily mono-therapies • “Kill the Pain” • We can fix it! Butler, Neuro Orthopedic Institute WCPT 2011 • Complete pain relief is possible!

BUT…. . Are Opioids Really Effective Against Pain

Noble, M. The Cochrane Collaboration. 2010

ANESTHESIOLOGY® 2016 ANNUAL MEETING • In the study, 2, 030 people with low back pain completed a survey about treatment. • Nearly half (941) were currently taking opioids. • When asked how successful the opioids were at relieving their pain, only 13 percent said “very successful. ” The most common answer – given by 44 percent – was “somewhat successful” and 31 percent said “moderately successful. ” Twelve percent said “not successful. ” • Seventy-five percent said they experienced side effects including constipation (65 percent), sleepiness (37 percent), cognitive issues (32 percent) and dependence (29 percent).


OPIOIDS AND CHRONIC PAIN-RISKS V. BENEFITS • Uncertain Benefits: • ? Pain relief • ? Improved physical functioning, QOL • Potential known harms: • • Fatal overdose Tolerance/physical dependence Addiction/abuse/diversion Respiratory depression--avoid in COPD Cognitive impairment--avoid in dementia Endocrine disruption- ED, muscle wasting, fatigue, OP Sleep disturbances; worsening sleep apnea Hyperalgesia on higher dose opioids

Biomedical To Biopsychosocial Model CULTURAL TRANSFORMATION IN THE WAY PAIN IS VIEWED, ASSESSED, AND TREATED

BIOPSYCHOSOCIAL MODEL OF PAIN Not just a symptom but your patient’s lived experience Pain Function al Disability Psychosocial

GOALS OF CHRONIC PAIN MANAGEMENT • Restore functioning • Improve quality of life • Reduce pain “A car with four flat tires” Medications only fill one tire

MULTIMODAL CHRONIC PAIN CARE Gentle exercise Manual therapies Acupuncture Yoga, Chigong Others CBT Mood/trauma therapies Substance abuse Tx Sleep Hygiene Meditation/Relaxation Physical Behavioral SELF MGT NSAIDS Anticonvulsants Antidepressants Topical agents Others Medication Procedural Nerve blocks/ablation Steroid injections Trigger point injections Stimulators

Multidisciplinary Approach • Biopsychosocial Model • Optimize non-opioid pain care; decrease opioid risk • Improve function and QOL Gatchel et al. , 2014; Wiedemer et al. , 2007; Dorflinger et al. , 2014; VA Do. D 2017, CDC 2016

Integrative Chronic Pain Care GROWING EVIDENCE BASE

INTEGRATIVE MODALITIES FOR PAIN • Safer in patients with comorbidities and polypharmacy • 30 -50% of veterans use CAM/Integrative modalities; only 1/3 disclose to their PCPs Smeeding et al. , 2016 • Integrative modalities for pain are NOT available at many VA’s despite patient preference for
 THERAPIES—PAIN National Center for Complimentary and Integrative Health http: //nccam. nih. gov/health/pain/chronic.")
INTEGRATIVE (CAM) THERAPIES—PAIN National Center for Complimentary and Integrative Health http: //nccam. nih. gov/health/pain/chronic. htm? nav=gsa 27

Additional Focus Accidental Overdose death in Veterans 47% higher (Bohnert, Ilgen, Galea, et al, 2011 and Bohnert, Valenstein, Bair, et al. 2011) Safe opioid prescribing through risk mitigation at time of refill

A Practical Opioid Rx Solution Opioid Risk Mitigation • • • Date of last prescription drug monitoring check Last urine drug screen Medication list Clinic visits dates Consent to long term opioid therapy management • Acknowledges discussion, education, and understanding of risk to benefit

“Motion is the Lotion”

The good physician treats the disease; the great physician treats the patient who has the disease. -Sir William Osler, circa 1900 © 2014 JPEP PAIN MANAGEMENT CURRICULUM

SPECIAL THANKS!! QUESTIONS?
- Slides: 33