Pain and brain scanning Physiology of pain Acupuncture

Pain and brain scanning • Physiology of pain • Acupuncture and pain • f. MRI imaging results with acupuncture • Hypnosis and pain • Imaging results with hypnotic analgesia • Learning theory, pain, and imaging For an overview on scanning and pain, see Chen (2001) International Journal of Psychophysiology, 42, 53 -65

Physiology of pain: A primer • Nociceptors = pain fibers • A-Delta Fibers • Large, (thinly) myelinated • Triggered by mechanical pressure or heat • Produce a fast, bright, localized pain sensation • In muscles, they are called Group III fibres • C-Fibers • Small, unmyelinated • Triggered by thermal, mechanical and chemical stimuli (polymodal) • Produce a slow, diffuse, aching sensation • In muscles, they called Group IV fibres
: • A-Beta Fibers • Large, myelinated,")
Another type of Peripheral Afferent Nerve (not nociceptive): • A-Beta Fibers • Large, myelinated, low threshold mechanoreceptors • Respond to light touch and low intensity mechanical info • In muscles, called Group II fibres
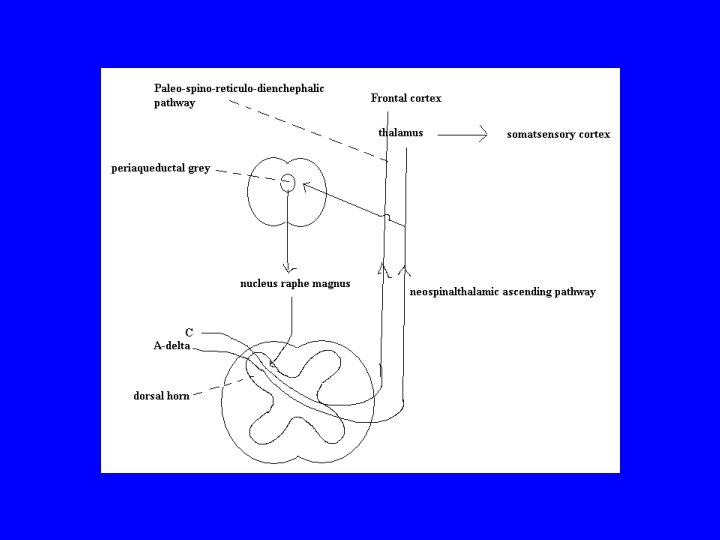

These receptors terminate in the dorsal horn of the spinal cord. There are two types of interaction (Gate theory of Melzack and Wall): 1. Within the dorsal horn of a spinal segment, there are direct local interactions between the different receptors; 2. The receptors project up the spinal column to the brain (various pathways); these trigger various descending inhibitory influences that act on the receptors of many spinal segments

Within the dorsal horn two interactions occur: 1. A-beta fibres stimulate GABA-ergic interneurons that inhibit C fibres 2. (Rubbing can ease pain) 2. A-delta fibres activate enkephalinergic interneurons that inhibit C fibres 3. (Pinch yourself to ease pain!) 4. These are local “segmental” effects: You must rub yourself in the same “dermatome” (I. e. area of skin subserved by the same spinal segment) to get the local effects
 to the nucleus raphe")
A descending inhibitory pathway comes from the periaqueductal grey (opiate) to the nucleus raphe magnus in the medulla To the dorsal horn (5 -HT), inhibiting C fibres This path is activated by 1) Projections from A-beta fibres 2) Projections from the neo-spino-thalamic tract, activated by A-delta pin prick fibres 3) These are non-local effects

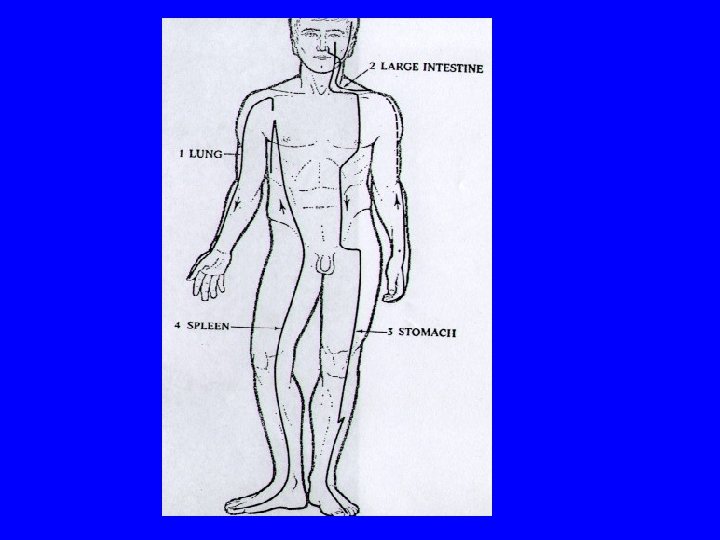
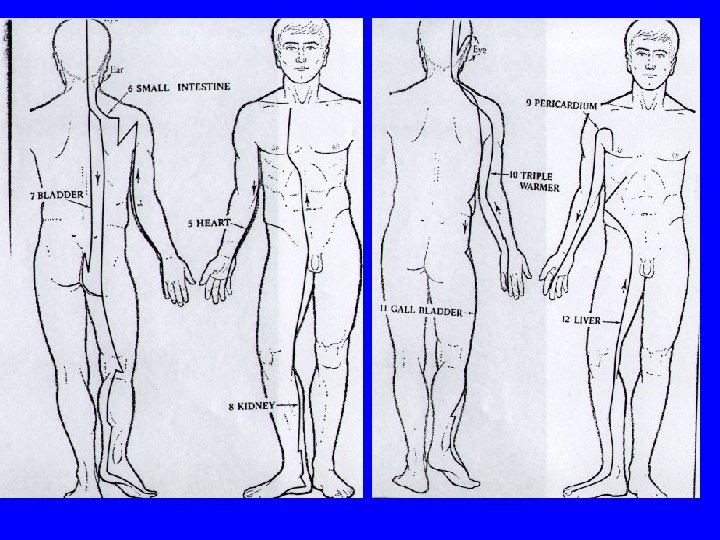
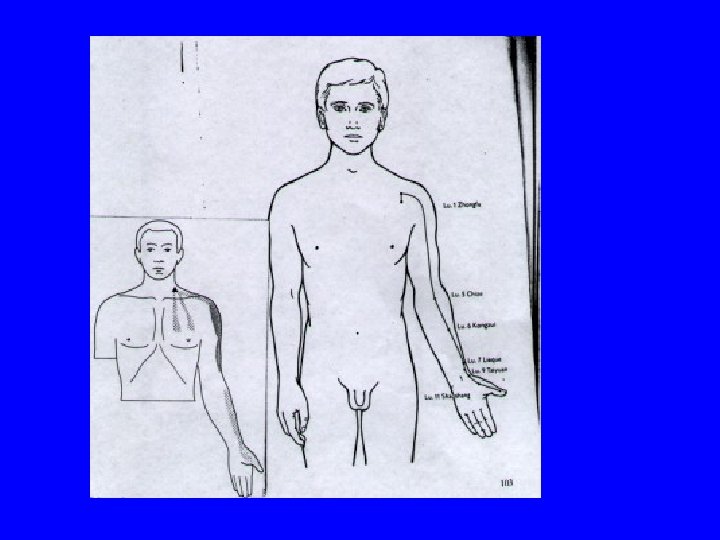
Traditional Chinese Medicine 2 nd century BCE Huang Di Nei Jing “The Yellow Emporer’s Classic on Internal Mecicine” specified that • there were 365 (classic) acupuncture points • These points lay on 14 meridians • The qi flowing through these meridians, as well as the blood through the blood vessels, constituted a circulatory system (postulated 1700 years before Harvey!) • Pain and illness generally could be cured though inserting needles in the points according to certain methods, which restored appropriate qi flow

Scientific evidence for acupuncture: 1. Acupuncture can be an effective method of pain relief: 2. Placebo: 30% 3. Sham points: 4. Real acupuncture: 5. 50% 70% Lewith & Machin (1983) Pain, 6, 111 -127 6. Acupuncture points are rich in A-delta fibres (in skin or muscles). Stimulation of Type II (A-beta) and Type III (A-delta) creates the “ de qi” sensation (numbness, heaviness, and mild aching) required for successful treatment; this stimulation triggers the segmental and central pain gating effects.
 reviewed 33 studies – under double blind conditions, P")
2. Pericardium 6 Vickers (1996) reviewed 33 studies – under double blind conditions, P 6 is an effective anti-emetic Journal of Royal Society of medicine, 89, 303 -310 P 6 stimulation is as effective as standard anti—emetic drugs (in treatment of nausea associated with chemotherapy, pregnancy, or surgery). Neighbouring sham points not so effective. How does it work? ? Don’t know of any scanning studies, but may be useful.
 on the back for various organs correspond to the")
3. “Alarm points” (Shu points) on the back for various organs correspond to the appropriate spinal segment for each organ.

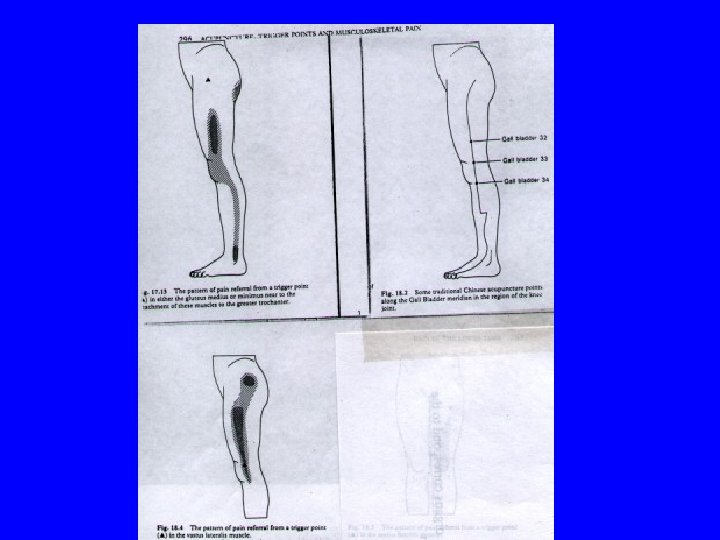
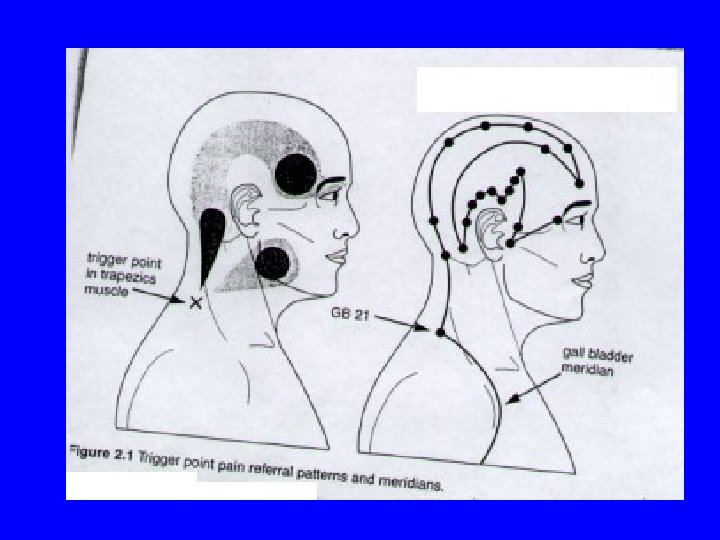
4. Referred pain: • Pain in an area where no clinical signs exist • Occurs because of a cross branching of nerve fibers to different areas • Thus the signals get confused by the brain and interpreted in a different manner e. g. injecting saline into muscle can cause pain to appear in other locations. Organ injury often refers pain; e. g. heart attack along the left arm, renal injury to the right shoulder, appendicitis to the lower abdomen and groin Palpable points or bands (trigger points) can refer pain along pathways. Trigger points are activated by trauma, stress, or by being located in the referred region of another trigger point (secondary activation).
 Trigger points and acupuncture points (71% concordance: Melzack) (b) Pain")
Strong correspondence between (a) Trigger points and acupuncture points (71% concordance: Melzack) (b) Pain referral pathways of trigger points and meridians. (c) Further, the best treatment of trigger point pain sydromes is to needle the trigger point! (d) See Baldry, P. E. (1998) Acupuncture, trigger points, and musculo-skeletal pain. (e) Churchill Livingstone.

When obtaining de qi, 20% of patients describe sensations that radiate for short distances, and 0. 4% had sensations propagate along channels (expectancy effect? )

f. MRI and acupuncture 1. One widely cited study: 2. Needling “eye” points in the foot created activation in the visual cortex similar to actual visual stimuli. Needling of non-acu points in the foot 2 -5 cm caused no activation in the occipital lobes. 3. Cho et al (1998). Proceedings of the National Academy of Science, 95, 26702673. 4. BUT: The authors claim the points used (BL 67 -60) are used for treating eye-related disorders based on the references: 5. Stux, G. , & Pomeranz, B. (1987) Acupuncture. Springer 6. (An abridged version is in the library) and 7. Kaptchuk, T. (1983). The web that has no weaver. Rider. 8. The abridged Stux and Pomerantz and Kaptchuk do NOT mention these Bladder points for eyes; in fact, they mention completely different meridians!
")
Acuxo web site: http: //www. acuxo. com/meridian. Pictures. asp (Excellent resource for acupuncture points) Does list Bl 60 -67 as eye-related – but they treat a whole range of other types of disorders as well. They don’t seem to be the main eye points. Also, some subjects showed acupuncture response in same direction as visual response, some in opposite direction. (yin and yang subjects? ? ) Gareus et al (2002) JOURNAL OF MAGNETIC RESONANCE IMAGING, 15 (3): 227 -232 Stimulated GB 37 which is an important eye point. NO f. MRI response detected in the visual cortex.
 Human Brain Mapping, 9,")
2. Stimulating analgesic point LI 4: Hui et al (2000) Human Brain Mapping, 9, 13 -25. LI 4 was needled in 13 volunteers (not in any current pain), and de qi sensation obtained in 11. These 11 showed increases in f. MRI signal in the somatosensory cortex DECREASES in nucleus accumbens, amygdala, hippocampus, hypothalamus, ventral tegmental area, insula and anterior cingulate (I. e. in limbic system areas associated with pain processing) The 2 volunteers who just felt pain produced INCREASES in anterior cingulate and insula (and no decreases). Suggests acupuncture mechanisms that go beyond the account I gave earlier. Replication in Wu et al Radiology 1999 Jul; 212(1): 133 -41 using LI 4 and St 36

Hypnosis and pain Hypnotizability varies along a coninuum: About 10% of people are “lows” and are barely able to experience hypnotic effects; about 10% of people are “highs” and can experience even the most difficult suggestions. Induction: ~10 minutes “you are becoming more and more relaxed, more and more deeply hypnotized…” Analgesia suggestion: e. g “You begin to notice how your arm is feeling more and more comfortable. . The pain is melting away. . the sensations in your arm becoming more and more pleasant…” Hypnotic analgesia correlates with hypnotizability about 0. 5.
 wrote")
Are hypnotized subjects just faking, or trying to please the hypnotist? Esdaile (1846) wrote of the large numbers of patients flocking to his clinic in India for the removal of tumors: “There must be some reason for this, and I only see two ways of accounting for it: my patients, on returning home, either say to their friends similarly afflicted, "Wah! brother, what a soft man the doctor Sahib is! he cut me to pieces for twenty minutes, and I made him believe that I did not feel it. Isn’t it a capital joke? Do go and play him the same trick…". Or they say to their brother sufferers, -- "look at me; I have got rid of my burthen…, am restored to the use of my body, and can again work for my bread: this, I assure you, the doctor Sahib did when I was asleep, and I knew nothing about it…".
: 56% of hypnotizable patients completed dental procedure without any chemical analgesic (75%")
Gottfredson (1973): 56% of hypnotizable patients completed dental procedure without any chemical analgesic (75% of very highly hypnotizables.
, whereas naloxone does impair acupuncture (and")
Hypnotic analgesia is unaffected by naloxone (opiate antagonist), whereas naloxone does impair acupuncture (and placebo) analgesia – different mechanisms involved with hypnotic and acupuncture analgesia. Some contrasting accounts of hypnosis: Woody & Bowers 1994 Hypnotic induction weakens Supervisory Attentional System so that action schema can be directly controlled by hypnotic suggestion Hilgard 1992 Hypnotic responding involves part of the supervisory attentional system splitting off from consciousness and then controlling action schema
. Anales de psicologia, 15, 133 -146. On course web site.")
Crawford et al (1999). Anales de psicologia, 15, 133 -146. On course web site. PET, f. MRI, r. CBF imaging techniques indicate hypnotic analgesia results in Higher anterior frontal activation Reduced anterior cingulate activation In highs rather than lows Crawford et al: Hypnotic analgesia depends on inhibitory processes in the anterior cortex - associated with the supervisory attentional system supporting Hilgard’s position. (For an introduction to hypnosis see Bowers (1983) Hypnosis for the seriously curious; for recent discussion of theories of hypnosis see Psychological Bulletin, 123 (1998), pp 100 -115, 186 -202. )

Learning theory and pain Rescorla-Wagner: Learning depends on the SIGNED difference (actual amount of pain - expected amount of pain) (signed mismatch) Mackintosh, Pearce-Hall depend, in addition, on the absolute amount of surprise, i. e. the UNSIGNED difference |actual amount of pain - expected amount of pain| (absolute mismatch)
 Proceedings of the National Academy of Sciences, 97, 92819286: A")
Ploghaus et al (2000) Proceedings of the National Academy of Sciences, 97, 92819286: A coloured light predicted a painful stimulus on most trials. After some trials, sometimes the painful stimulus occurred when it was not expected; sometimes it did not occur when it was expected. f. MRI activations showed an area responsive to signed mismatch: superior parietal gyrus AND areas responsive to absolute mismatch: hippocampus, superior frontal gyrus, cerebellum Supporting learning rules like Mackintosh, Pearce-Hall
- Slides: 29