Paediatric Ophthalmology Community to the hospital Siobhan Wren

Paediatric Ophthalmology Community to the hospital Siobhan Wren Consultant Ophthalmologist

Hospital Service Workload Amblyopia Visual development/assessment Evaluation of the paediatric patient Red reflex Detecting squints Red eyes
 68% 40. 0% Possible Amblyopia present in 124")
Diagnosis of Paediatric Referrals (March 09) 68% 40. 0% Possible Amblyopia present in 124 35. 0% 30. 0% 25. 0% 20. 0% 15. 0% 10. 0% 5. 0% 0. 0% Squint Glasses NAD Other includes ptosis/NF/retinal ab. N Red eye Learning disability Epiphora Other Data available for 319/337

Amblyopia • Strabismus • Refractive • Occurrence – 1 -3% population – up to 5% pre-school

Visual development • 1 month – pupils react to light – defensive blink present by 6 -8 weeks – 3 weeks onwards watches familiar nearby face when being fed – gaze caught and held by dangling bright toy gently moved in line of vision at 15 - 25 cm

• 3 months – very alert – fixes and follows toy at 15 -25 cm – converges eyes if toy brought toward eyes • 6 months – any squint now is abnormal – reaches out for objects – searches for toy once it leaves visual regard

• 9 months – very alert to people – immediately grasps for toys – watches activities of people or animals within 3 -4 metres with sustained interest for several minutes • 12 months – interest in pictures – points to objects of interest

Health Visitor Questionnaire at 8 months and 2½yr contact 1. Do the parents suspect a squint? 2. Are there any concerns about vision, eye lids, eye movements, pupil size or shape? 3. Is there any family history of squint, amblyopia, glasses in early childhood, or wearing a patch. 4. Are there any risk factors of squint combined with family concerns i. e. prematurity or developmental delay

Conclusions of Study into Fast track appointments ØFast track clinic run by a highly specialised orthoptist and paediatric optometrist can successfully assess large numbers of amblyopia &/or strabismus suspects. ØA 74% discharge rate of 1 st referrals, following the protocol, has a significant impact on paediatric outpatient clinic. ØSurgical rates within this group of patients is in line with the national surgical rates.

Making a diagnosis EXAMINATION HISTORY • Family history • Identify risk factors – Prematurity – Developmental delay – Juvenile Rh Arthritis • • Family album Photophobia Redness Discharge – Purulent, watery • • External inspection Red reflex Corneal light reflex Cover test – Squinting – Head tilt – Eyelid closure • Visual acuity >3 yrs – Defective ocular fixation/ interactions

Red reflex technique ü Sit in front of the child and parent at about arm’s length. Set the ophthalmoscope to around +2 (green or black) ü Focus on the parent’s eyes to show that the test is non-invasive and recognition of the normal red reflex in that particular ethnic group. ü Then focus on the child’s face and encourage the child to look at the light. Focus on the red reflex within the pupil.

The Childhood Eye Cancer Trust


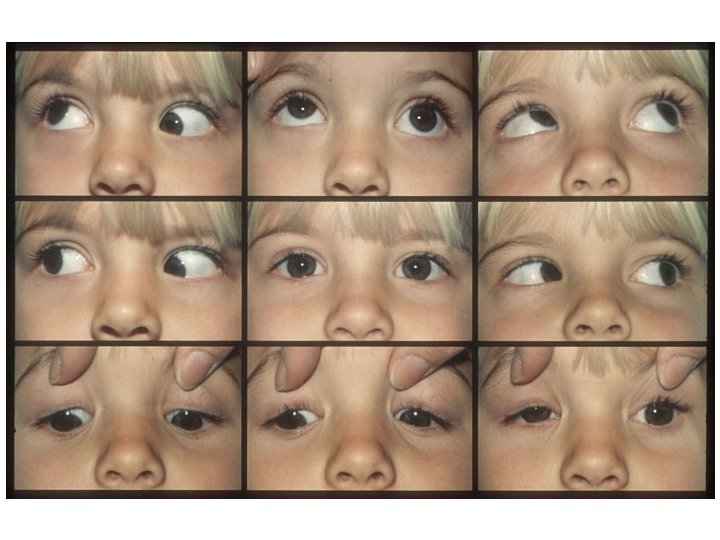
Head postures • Check motility

Conjunctivitis • • • Close contacts affected Unilateral bilateral Sticky discharge Diffuse redness Cornea and pupil normal Chloramphenicol • Cellulitis- Refer urgently • Neonatal conjunctivitis: refer urgently – Risk of corneal perforation from n. gonorrhoea
 Perennial allergic conjunctivitis (PAC) • Vernal keratoconjunctivitis")
Allergic conjunctivitis • Seasonal allergic conjunctivitis (SAC) Perennial allergic conjunctivitis (PAC) • Vernal keratoconjunctivitis (VKC) Atopic keratoconjunctivitis (AKC) • Giant papillary conjunctivitis (GPC)

Symptoms Itching Tearing 0 Absent Rubbing eyes No desire 1 Trace Transient Rare 2 Mild Occasional 3 Moderate Frequent 4 Severe Constant

Signs Redness 0 1 Absent Mild Eyelid/ Conjunctiva swelling Absent Mild 2 Moderate 3 Severe Sub-tarsal Normal Uniform ‘velvety’ papillae appearance Non uniform with papillae Giant papillae

Management • Allergy testing • Cool compress • Artificial tear substitutes • Systemic and/or topical antihistamines • Vasoconstrictors • Mast cell stabilizers • Nonsteroidal antiinflammatory drugs (NSAIDs) • Corticosteroids • Immunotherapy
 >5 yrs")
Otrivine-antistin BD/TDS £ 2. 35 antazoline & xyometazoline antihistamine and vasoconstrictor (weak) >5 yrs NB sympathomimetic Optilast QDS £ 6. 40 azelastine Antihistamine >4 yrs 6 weeks Emadine BD £ 7. 49 emadastine Antihistamine >3 yrs Relestat BD £ 14. 00 Epinastine Antihistamine >12 yrs 8 weeks Sodium chromoglycate QDS £ 3. 08 (many other names eg Optichrom) sodium chromoglycate mast sell stabiliser (weak); very safe Rapitil BD/QDS £ 5. 12 nedocromil sodium mast sell stabiliser >6 yrs 12 weeks Alomide QDS £ 5. 48 lodoxamide mast sell stabiliser >4 yrs Zaditen BD £ 9. 75 ketotifen mast sell stabiliser >3 yrs Opatanol BD £ 4. 11 olopatidine mast sell stabiliser >3 yrs 16 weeks Acular £ 5. 00 ketorolac prostoglandin inhibitor Ocufen £ 37. 15 fluriprofen prostoglandin inhibitor Voltarol £ 6. 68 diclofenac prostoglandin inhibitor
- Slides: 22