Pacemaker Therapy in Congenital AV Block Alpay Celiker

+ Pacemaker Therapy in Congenital AV Block Alpay Celiker M. D. Acıbadem University Istanbul, Turkey

+ Pacing in Pediatric Patients n Advances in lead and device technology allow pacemaker system implantation in children and even in neonates n Specific problems in children such as small vessel size, cardiovascular abnormalities often lead to implant problems. n Physical activity and somatic growth may affect lead longevity in young patients

+ Class I-IIa Indications n n Advanced second- or third-degree AV block associated with symptomatic bradycardia, ventricular dysfunction, or low cardiac output. (Level of Evidence: C) Congenital third-degree AV block with a wide QRS escape rhythm, complex ventricular ectopy, or ventricular dysfunction. (Level of Evidence: B) Congenital third-degree AV block in the infant with a ventricular rate less than 55 bpm or with congenital heart disease and a ventricular rate less than 70 bpm. (Level of Evidence: C) Congenital third-degree AV block beyond the first year of life with an average heart rate less than 50 bpm, abrupt pauses in ventricular rate that are 2 or 3 times the basic cycle length, or associated with symptoms due to chronotropic incompetence. (Level of Evidence: B)
 Epicardial Leads: Implant")
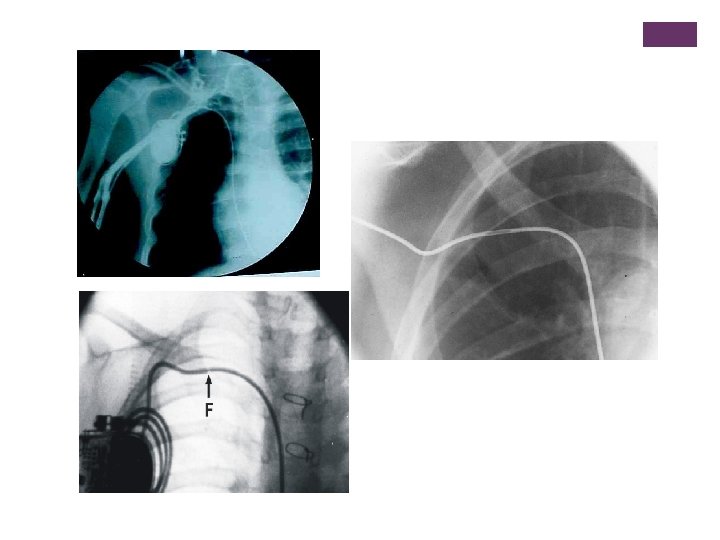
+ Points of Interest Leads: Route Endocardial Classical Lumenless (4 F) Epicardial Leads: Implant Place Right ventricle vs Left ventricle Apex vs septum Chamber Paced VVIR, DDD, or VDD Leads: Fixation Mechanism

+ Pros and Cons of Transvenous Leads n Leads generally more reliable than epicardial implants n Procedure n n more easy § § Less thresholds Fast adaptation to new pacemaker systems § § Venous obstructions Pace related impaired ventricular function. Lead infections Lead extraction necessity Interaction with cardiac valves Impossible in some patients
 total venous obstruction; 10 (12%) partial obstruction.")
Venous Occlusion: 11 out of 85 (13%) total venous obstruction; 10 (12%) partial obstruction. Age, body size and lead type not associated with occlusion > 3 years. Bar Cohen 2006 Tricuspid valve issue: 27 out of 123 TR increased. No severe TR. No change (63%) or improved (12%). Berul 2008.

15 year old boy with postoperative AV block. VDD pacemaker. Needs biventricular pacing. What to do? ? ?

: n. Superficial 1, 2 %")
+ Pediatric Pacemaker Infections* n Perioperative Infections (before discharge): n. Superficial 1, 2 % n. Deep 0, 2 % n Early Pacemaker Infections (< 60 days) n. Superficial 3, 1 % n. Deep 1, 2 % n Late Pacemaker Infections n. Superficial 0, 5 % * Cohen et al J Thorac Cardiovasc n. Deep 0, 7 % Surg 2002; 124.

LEAD EXTRACTION WITH SEVERAL METHODS Cecchin et al. Circ Arrhythm Electrophysiol. 2010.

+ Excimer-laser extraction in children n n n 25 patients, 43 leads (36 pacing/7 ICD leads) Median age at extraction 13, 9 years (8, 4 -29, 2) Mean duration of lead 49, 4 months (3 -128) Lead fracture 37/43 leads (86, 6%) Lead position: Ventricular 58%, atrial 42% Complete removal 39/43 (91%), partial in four Major complication 2/25 n Cardiac perforation and tamponade n Thrombosis of left subclavian and innominate vein Moak J et al. PACE 2006.

+ Epicardial Pacing Pros: n n Venous access not required Usable patients with compromised venous access n Allows left ventricular pacing, even in small patients n Dual chamber pacing in small patients Cons § Implantation procedure more invasive than endocardial § Surgery required § Leads are weaker

Papadopulos et al. Long-term follow-up after steroid-eluting epicardial pacemaker implantation in young children: a single centre experience. 45 patients, mean age at implant 3, 2 yrs, 5. 7 years + 15 months (range of 6 months to 7. 3 year) follow-up

Retrocostal approach is neither superior nor inferior to the subrectus or subxiphoid approach in terms of lead longevity and from failure. Lichtenstein BJ, et al. Does Pocket Location Affect Lead Survival? Pediatr Cardiol 2010.

+ Epicardial versus Endocardial Pacing: Conclusion Epicardial: <15 kg Compromised venous access or a univentricular heart Pace the left ventricle Endocardial Possible implant >15 kg Venous occlusion Risks of future lead extraction Beware of pacing induced heart failure

+ VVIR vs DDD Pacing VVIR n. Pros: One lead required, Smaller generator, gives satisfactory exercise tolerance, slower heart rates than DDD n. Cons: Heart rate response is not physiological, loss of AVsynchrony, DDD Pros: Physiological heart rate response, AV synchrony maintained, reduced risk of atrial fibrillation Cons: Two leads required, larger generator, faster heart rates than VVIR, pacemaker mediated tachycardia

+ VDD Pacing n Disadvantages n Advantages n Single lead dual chamber sensing n Avoid of many electrodes n Provide AV Synchrony n Avoid of venous thrombosis? ? Atrial sensing problems in postop. cases n Relative change of atrial dipole with the growth n Decrease of AV synchrony with time n Lack of active fixation n Large electrodes n No indication in SSS n Lack of epicardial use n

An inhomogeneous and dyssynchronous electrical activation of ventricles, leading to changes in myocardial architecture and left ventricular mechanical contractions. This problem is secondary to right ventricle apical pacing via transvenous pacing. Karpawich P. Pace 2008

+ Site Selective Pacing • Pioneereed by Karpawich. • Implant possible to desired place • Less material at venous system and heart • Similar results compared to conventional systems • Lead extraction issue? • Long-term results? Select Secure system: steroid eluting, bipolar, lumenless, nonretractable screw-in 4, 1 F lead (model 3830, Medtronic, Inc. ), delivered through a 8 F steerable catheter (Select Site) Karpawich et al. Altered cardiac histology following apical right ventricular pacing in patients with congenital atrioventricular block. Pacing Clin Electrophysiol 1999

+ Gabbarini and Agnoletti. Selective-site pacing in paediatric patients: use of the Select Secure System and risk of vein occlusion. Europace 2010 20 patients 40 leads. No sign of venous occlusion at the ultrasound exam at a median follow-up of 19 mos (range 6 -44 mos)

Khan a, Zelin K and Karpawich P. Performance of the Lumenless 4. 1 -Fr Diameter Pacing Lead Implanted at Alternative Pacing Sites in Congenital Heart: A Chronic 5 -Year Comparison. PACE 2010.
 3. 3 ±")
+ Group I Group 2 n= 80 n=91 P-wave (m. V) 3. 3 ± 1. 9 3, 7 ± 2. 2 R-wave (m. V) 10 ± 4. 2 12 ± 5, 6 Impedance (Ω) 747 ± 251 881 ± 224 Threshold (msec at 2, 5 V) 1, 02 ± 0, 5 0, 056 ± 0, 2 Follow-up (4 -5 year) n=80 n=11 P-wave (m. V) 3. 9 ± 2. 4 6, 2± 4, 8 R-wave (m. V) 11, 2 ± 6. 9 10 ± 4, 3 Impedance (Ω) 677 ± 267 562 ± 75 Threshold (msec at 2, 5 V) 0, 05± 0, 02 0, 08 ± 0, 07 Implant

Preserved cardiac synchrony and function with single-site left ventricular epicardial pacing during mid-term follow-up in paediatric patients. Tomaske M, Breithardt OA, and Bauersfeld U. Europace 2009.
 Interventricular mechanical delay (ms) 62± 15 17±")
+ RV PACE (N=10 LV PACE (N=15) Interventricular mechanical delay (ms) 62± 15 17± 10 Septal-to-posterior wall motion delay (ms) 294± 84 59± 23 Septal-to-lateral wall delay, by TDI (ms) 59+12 40± 19 LV mechanical delay, 2 D strain (ms) Mitral valve level 159± 44 72± 31 LV mechanical delay, 2 D strain (ms) Papillary muscle level 127+25 64± 23 RV mechanical delay, 2 D strain (ms) 62± 33 57± 23 RV (ms) 197± 42 210± 43 LV ejection fraction (%) 45± 6 60± 6 LV end-systolic volume index (m. L) 33± 11 22± 5 Aortic velocity – time integral (cm) 21± 2 26± 4 LV Tei index 0, 63± 0, 11 0, 38± 0, 07

+ Conclusion n Long term complications of pacing in childhood include venous occlusion, impaired ventricular function, lead failure, and risks of multiple implants and explants. n Right ventricular apical pacing should be minimised where possible. n In small infants epicardial pacing should be encouraged. n Long term complications largely related to problems with the leads.

- Slides: 27