Ovarian tumors Management Treatment Obestrics and genicology ward

Ovarian tumors Management &Treatment Obestrics and genicology ward Alavi hospital

Follicular cyst: • the most common functional cyst of the ovary Causes: • • • Chronic pelvic congestion as with chronic pelvic infection, fibroid and endometriosis Hormonal: excessive gonadotrophin secretion as in metropathia hemorrhagica or exogenous gonadotropin therapy. Capsular thickening and adhesions preventing the rupture of the follicle.
 Pathology • Cysts arise from the ovarian follicles either as")
Follicular cyst (cont. ) Pathology • Cysts arise from the ovarian follicles either as retention cyst of Graafian follicle which has failed to rupture or from cystic overdistension of atretic follicle. • May occur at any age before the menopause • Cysts are multiple (rarely single) and small in size (rarely exceed 5 -7 cm) • Cysts are unilocular, has thin wall and contain clear fluid • Their lining cells (granulosa and theca cells) may secrete excessive quantities of estrogens. The ovum degenerates early, while the lining granulosa cell persist functioning for a variable time. Ultimately, the increased pressure of the liquor causes the granulose cells to flatten and cease function and finally it disappears. Cysts become lined only by theca cell layer.

• Symptoms: may be asymptomatic • Pain in the iliac fossa • Menstrual disturbances: delayed menstruation or irregular bleeding It may simulate ectopic pregnancy in its presentation. Diagnosis: pelvic examination and ultrasound Complications: hemorrhage and rupture Treatment: the cyst usually regress spontaneously. Hormonal therapy e. g. gestagens or COCs may be used to enhance disappearance of the cyst. Surgery is rarely indicated if ruptured follicular hematoma or the cyst persist or increase in size

Corpus luteum cyst: Pathology: • • Occur due overdistension of the corpus luteum with fluid The cyst is usually unilocular, of variable size, has thin wall and contains clear content or hemorrhagic fluid Symptoms: Pain and delayed menstruation Diagnosis: pelvic examination, ultrasound and BHCG to exclude ectopic pregnancy Treatment: the cyst usually disappears spontaneously. Surgery is rarely indicated if the cyst ruptures.

Theca lutein cyst: Pathology: • • Result from excessive amount of HCG in the circulation which may be due to pregnancy or induced by ovulatory drugs. They are found in of cases of vesicular mole and of chorion epithelioma due to high HCG output. They usually atrophy after evacuation of the mole. They may reach large size as in ovarian hyperstimulation They are bilateral, multilocular thin walled and contained clear fluid Treatment: The cyst usually regress spontaneously after evacuation of vesicular mole or after stoppage of HCG

Theca lutein cysts

Polycystic ovary syndrome
, bilateral and separate from CL")
Pregnancy luteoma: Pathology: • Rare, size (8 -15 cm), bilateral and separate from CL • It is yellow or gray on cut section. • Formed of luteinized cells usually theca – lutein cells • Rarely result in virlization of the mother or her female fetus Symptoms: asymptomatic and usually discovered accidentally (during CT or U/S) Treatment: It is not true neoplasm and regress after delivery

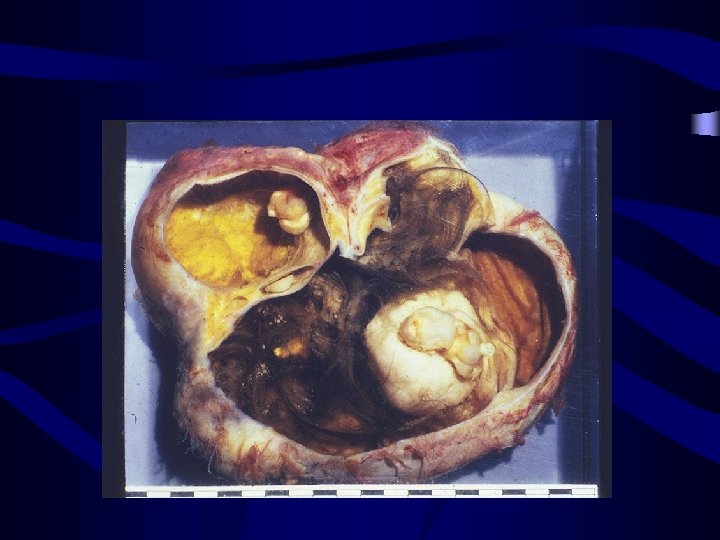
Endometriotic cyst: Pathology: • One or more cysts filled with thick brown fluid (dark altered blood) similar to liquid chocolate (chocolate cyst due to the colour of the content) • Due to lack of resistance, the cyst may reach a large size and usually rupture during attempt of removal • 1/3 of cases is bilateral and can be multiple, rarely exceed a diameter of 10 cm • Lined by epithelium resembling that of endometrium. Symptoms: see endometriosis Treatment: see endometriosis

Origin of Ovarian Tumors Surface epithelial tumors Germ cell tumors Sex cord-stromal tumors • Cystadenoma • Cystadenocarcinoma • Granulosa-theca cell tumor • Sertoli-Leydig cell tumor • • Teratoma Dysgerminoma Yolk sac tumor Choriocarcinoma

Epithelial ovarian tumours: Serous cystadenoma • • • 25% of all ovarian benign tumours Unilateral but bilateral in 12 -20% 20 -50 y Size is variable 5 -15 cm Unilocular Mitosis rare and no nuclear atipy
 in")
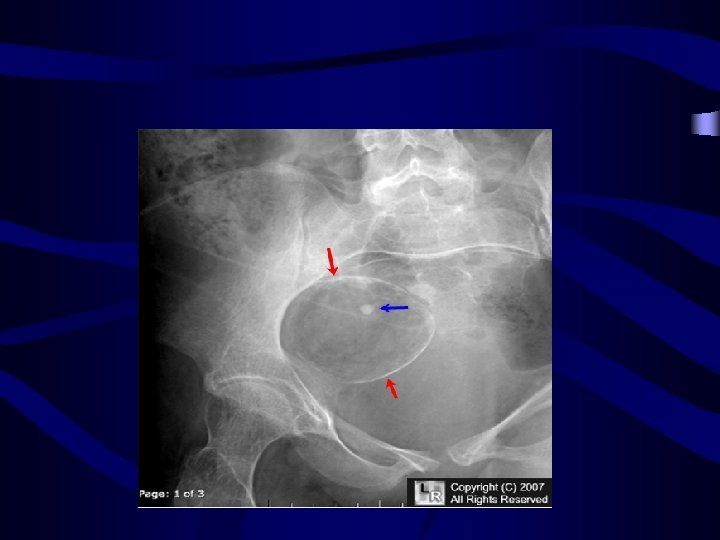
Epithelial ovarian tumours: Serous cystadenoma • Sometimes, it contains calcareous granules (psammoma bodies) in 15% of cases, we can see in abdomen X-Ray • • Treatment: Want to be pregnant: cystectomy Want to not be pregnant: USA Bilateral tumor: BSA
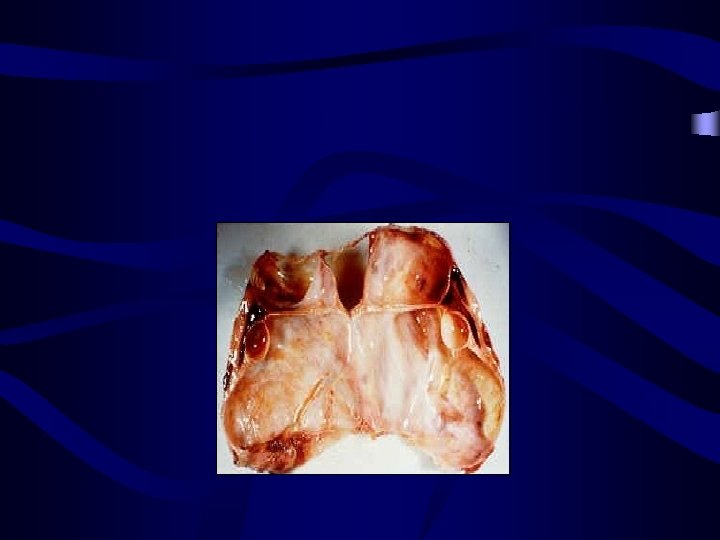

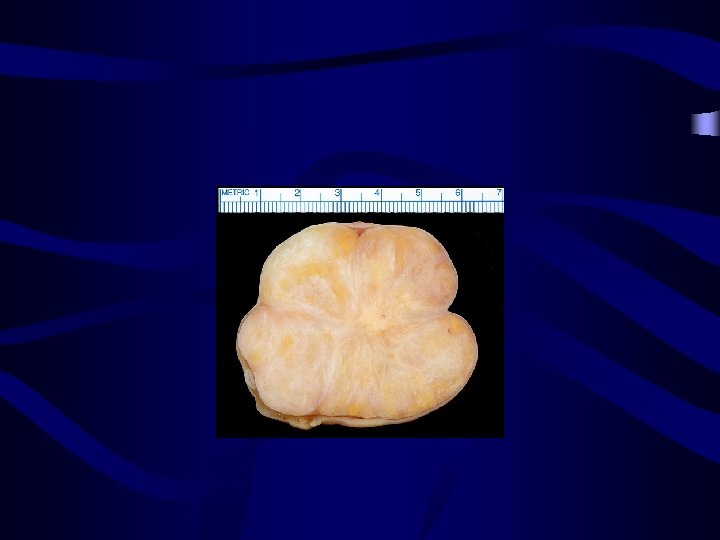
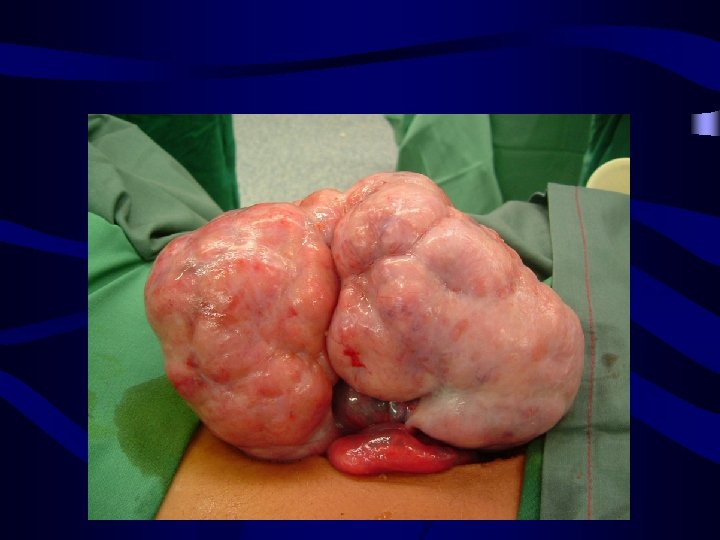
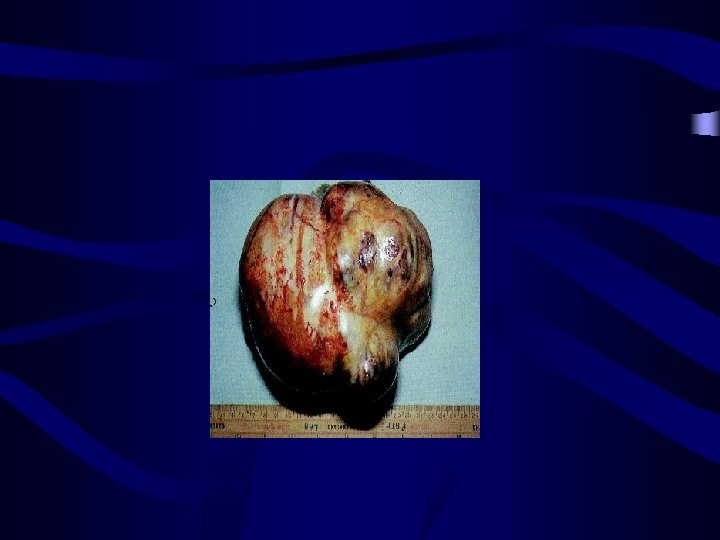
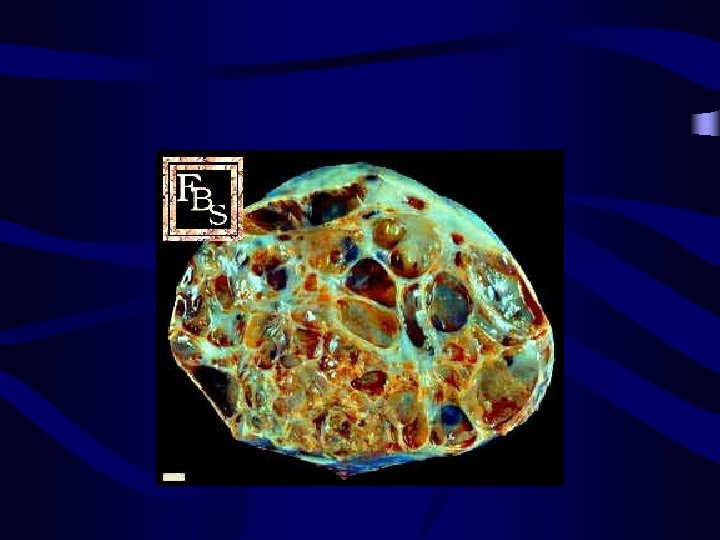
Epithelial ovarian tumours: mucinous cystadenoma: • • • 25% of benign ovarian tumours Occur at 20 -50 age Usually unilateral and is bilateral in 2 -3% of cases Multilocular which may reach a huge size (50 cm or heigher). Symptoms: pain+abdominal or pelvic mass

Epithelial ovarian tumours: mucinous cystadenoma: • The cyst is lined by tall columnar epithelium secreting a mucin like epithelium resemble that of gut or both with goblet argentafine cells glycoprotein. . The the endocervix or cells, panet cells • Treatment: • same of serous cystadenoma+apendectomy

mucinous cystadenoma

Patient with ovarian cystadenoma

Ovarian cystadenoma
: • • 2%of ovarian tumors occur in")
Epithelial ovarian tumours: Brenner's tumour(transisional cell tumor): • • 2%of ovarian tumors occur in old age mean 50 y Unilateral and 6 -7% bilateral Benign in 99% in many cases associated with mucinous cystadenoma. Variable in size (microscopic to 30 cm) Symptom: variable(non symptomatic or palpable mass+pain) Solid or cystic

Epithelial ovarian tumours: Brenner's tumour: • It was though to be totally benign but reports of a number of malignant Brenner tumours are present • Microscopically, the tumour is composed of cell nests of epithelial cells that resemble transitional epithelium of urinary tract and has characteristic coffee bean nuclei • • Treatment: tumor resection
: • • • Commonest ovarian")
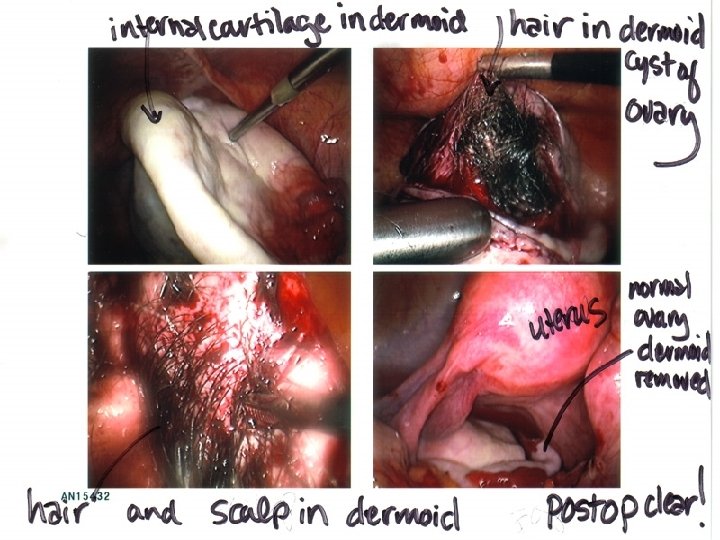
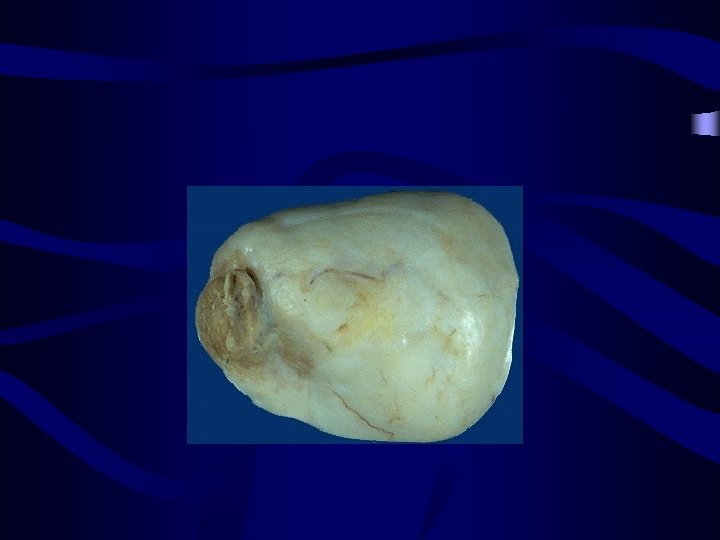
Germ cell ovarian tumours: Dermoid cyst (benign cystic teratoma): • • • Commonest ovarian benign tumor It appears at a relatively young age 20 -40 y 5 -10% of cystic ovarian tumour Show derivatives of all the 3 germ cell layers Size is usually ( 5 -10 cm) Globular oval shape. Bilateral in 8 -15% of cases White or grayish in colour Unilocular

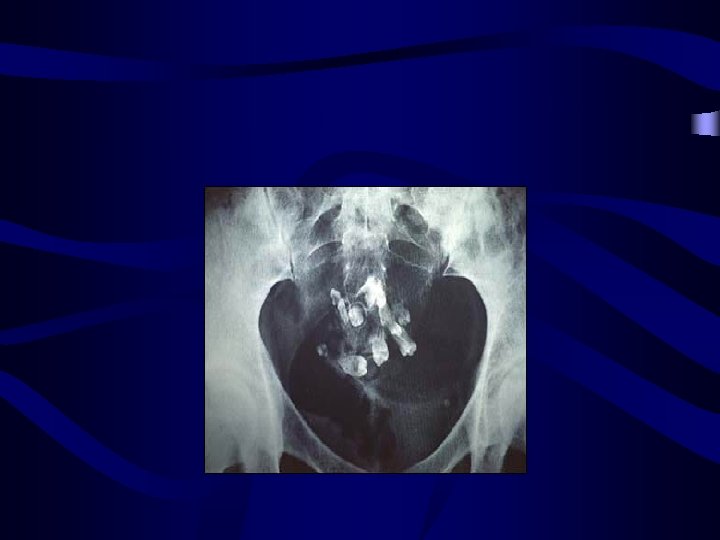
Germ cell ovarian tumours: • Dermoid cyst: o o o Its contents are derived from the three embryonic cell layers: Ectoderm: skin, hair, teeth & nervous tissue (prominent) Mesoderm: cartilage, bone and muscles Endoderm: thyroid, stomach and intestinal tissue • Solid compenent of the tumor is named rocky tansky prominence • Diagnosis: • Radiological diagnosis gives radio-opaque appearance (teeth & cartilage) but transvagianl sonography is the choice for diagnosis MRI • •
 Malignancy: SCC •")
• • • Complication: Torsion (It is freely mobile ) Malignancy: SCC • • Treatment: Laprascopic cystectomy and look at other ovary

Germ cell ovarian tumours: Struma ovarii: • Very rare, mostly benign but may undergo malignant transformation. • Composed mostly of thyroid tissue • Usually found with mucinous cystadenoma and rarely alone. • Produce thyrotoxicosis in 5% • Folicular cancer • Diagnosis: I 131

Germ cell ovarian tumours: Struma carcinoid: • Rare tratoma: thyroid tissue+carcinoid tissue • Serotonin and bradykinin • 50%Size over 4 cm= Carcinoid syndrome
: • • • 2% of ovarian tumors")
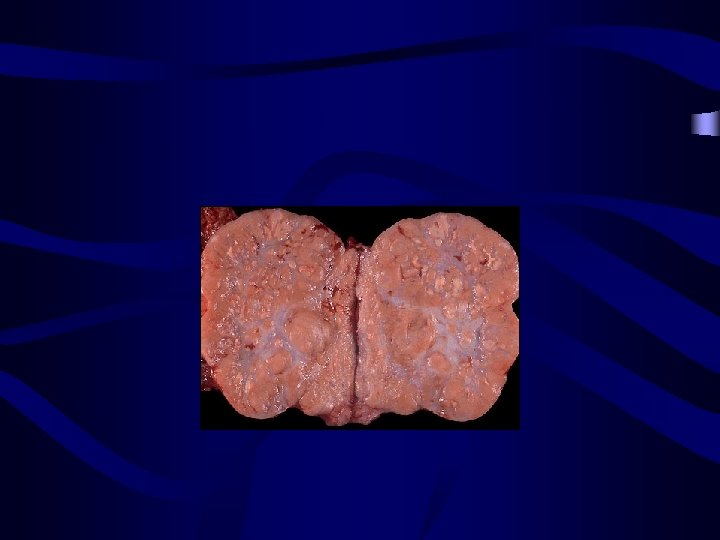
stromal ovarian tumours: Thecoma (Theca cell tumour): • • • 2% of ovarian tumors Comonest in postmenstural woman usually unilateral that occur in older age (cause PM bleeding). Symptoms: AUB or PM bleeding Associated with andometrial adenocarcinoma (secetion of strogen) • Size variable: non palpable to solid mass 15 -20 cm • Treatment related to age of patient
 Mostly unilateral")
stromal ovarian tumours: Fibroma: • • No particular age of incidence(40 -60) Mostly unilateral and multinodular Cut surface is trabeculated. Size variable: non palpable to solid mass 15 -20 cm
 • It")
Complications of the Fibroma: Meig's syndrome: (Ascites + hydrothorax + Ovarian fibroma) • It was thought to occur only with fibroma, but now known to be associated with other tumour as Brenner tumour or Krukenberg tumour. • • Treatment: Removal of the tumour results in prompt resolution of abdominal and pleural fluid

Complications of the Fibroma: Herdiatery basal cell nevus syndrome: Early BCC+jaw cratocytes+dura calcifacations+ mesenteric cysts

Thanks for your attention
")
Staging The Federation Internationale de Gynecologie et d'Obstetrique (FIGO)

Stage I ovarian cancer • limited to the ovaries

Stage IA: tumour limited to 1 ovary, the capsule is intact, no tumour on ovarian surface and no ascites

Stage IB: tumour limited to both ovaries, capsules intact, no tumour on ovarian surface and no ascites

Stage IC: tumour is limited to 1 or both ovaries with any of the following: capsule ruptured, tumour on ovarian surface

Stage II ovarian cancer • tumors involving 1 or both ovaries with pelvic extension and/or implants

Stage IIA: extension and/or implants on the uterus and/or fallopian tubes.

Stage IIB: extension to and/or implants on other pelvic tissues
; capsule ruptured or")
Stage IIC: Pelvic extension and/or implants (stage IIA or stage IIB); capsule ruptured or with malignant cells in ascites or peritoneal washings.

Stage III ovarian cancer • tumours involving 1 or both ovaries with microscopically confirmed peritoneal implants outside the pelvis. Superficial liver metastasis equals stage III.
. No lymph nodes metastasis")
Stage IIIA: microscopic peritoneal metastasis beyond pelvis (no macroscopic tumour). No lymph nodes metastasis

Stage IIIB: macroscopic peritoneal metastasis beyond pelvis less than 2 cm in greatest dimension. No lymph nodes metastasis

Stage IIIC: peritoneal metastasis beyond pelvis greater than 2 cm in greatest dimension and/or regional lymph node metastasis.

Stage IV ovarian cancer tumours involving 1 or both ovaries with distant metastasis. Parenchymal liver metastasis equals stage IV.

tumours involving 1 or both ovaries with distant metastasis. Parenchymal liver metastasis; pleural effusion with citology+ equals stage IV.

Germ cell malignant tumors

Tumor markers in gerrm cell ovarian cancer

LDH • • Yolk sac tumor: elevated Imature teratoma: probably Dysgerminoma: elevated Choriocarcinoma: non elevated

h. CG • • Yolk sac tumor: probably Imature teratoma: probably Dysgerminoma: rarely Choriocarcinoma: ever

CEA • • Yolk sac tumor: elevated Imature teratoma: probably Dysgerminoma: non elevated Choriocarcinoma: non elevated

CA 125 • • Yolk sac tumor: elevated Imature teratoma: probably Dysgerminoma: rarely Choriocarcinoma: non elevated

AFP • • Yolk sac tumor: ever Imature teratoma: probably Dysgerminoma: non elevated Choriocarcinoma: non elevated

Dysgerminoma: • • • Highly malignant tumour but radiosensitive. It is the commonest malignant germ cell tumour of ovary Occurs primarily in young women & 80 % occur in young age (below 30 years) and rarely in old age. 10 -15%of cases bilateral and rapidly growing Usually small & smooth surface. Hormonally in 10% Bhcg+ Serum LDH elevated=Tumor marker follow up and treatment In children: early maturity or primary amenoreha Solid tumour. show cystic degeneration. Cut surface is grayish white with areas of hemorrhage & necrosis. Microscopically, it looks like seminona and is composed of large round cells

Treatment of dysgerminoma: Treatment depend to the age of patient: • • Young multiparous women: unilateral salpingoophrectomy Old patient: TAH & BSO Very sensative to radiotherapy and chemotherapy Chemotherapy is choice after surgery in patient with stage 1 a or heigher (BEP)
 or Endodermal Sinus Tumour (EST): • • The tumours are")
Yolk Sac Tumour (YST) or Endodermal Sinus Tumour (EST): • • The tumours are soft and friable with a smooth external surface Patient are younger than 30 years Severe cases in pregnancy AFP is elevated=Tumor marker follow up and treatment solid variegated yellow or gray sectioned surface 3 -30 cm Extensive hemorrhage and necrosis is usual. Microscopically, there is a wide variety of patterns and several histologic subtypes. Typical features are Schiller-Duval bodies • • Treatment: Adjuvant chemotherapy (BEP) after surgery

Immature teratoma: • • Show derivatives of all the 3 germ cell layers +embreyonal tissues AFP cna be elevated Occurs at young age : in 2 first decades smooth surface and unilateral Size: 9 -28 cm capsular ruptures are seen in nearly half Most immature tissue: nervous tissue derived from ectoderm Immature is associated with poor prognosis • • • Treatment: To satge 1 a: only surgical therapy Heigher than 1 a stage: adjuvant chemotherapy after surgery

Choriocarcinoma of the ovary: • is another rare germ cell tumor • The endocrine activity of this neoplasm may cause precocious puberty • DD: EP • Big unilateral solid

Emberional carcinoma • • Mean age 15 y Very malignant AFP and h. CG both elevated AUB

Gonadoblastoma • • • Gonadal dysgenesia or pseudohermafrodism Kariyotype: 46 XY, 45 X46 XY Most in female phenotype With dysgerminoma Wooman with pelvic mass and abnormal maturity=kariyotype

• • • Symptoms: Primary amenoreha, virilization Second decade of life Most in right gonad Treatment: BSO

Sex cord-stromal malignant tumors

Granulosa cell tumour: Feminizing tumour producing estrogen and the commonest sex cord stromal tumour (1 -2% of malignant ovarian tumours) • Can occur at any age most in 50 -55 y • Tumor produce estrogen and leads to: * In prepubertal female leads to menorragia, amenoreha, metroragia * In postmenopausal leads to P. M. bleeding *hyperplasia or endometer carcinoma • • It is unilateral, rounded with smooth surface. It is generally small (10 -12 cm). Cut section: small grayish, white or yellow with hemorrhages High inhibin level may be associated which can be used as tumour marker • The cells may be arranged around small cavity forming rosettes of cells which create the appearance of Call Exner bodies.

Treatment: • • No place for radiotherapy or chemotherapy USA: in children with stage Ia Along the lines of treatment of epithelial cancer: if fertility is not desired

Sertoli cell tumour: • • • Rare solid tumour. Symptom: pelvic or abdominal mass Can secrete: estrogen, androgen and progestron Unilateral size: 9 cm Relationship between this tumor and Putzjeger syndrome • • Treatment : surgery

Sertoli leydig cell tumour: • • • Small tumour 12 -15 cm Young wooman(mean 25 years old) Secrete androgen Symptoms: oligmenoreha, atrofy of breast, achnea, hoarseness, cliteromegaly Secrete estrogen Symptoms: menoragia menometroragia Defrentiate with adrenal tumors(urine 17 -cetostroid elvated) Elevated AFP Composed of mixture of Sertoli & Leydig elements low grade of differentiation with bleeding and necrosis

• Treatment: Unilateral salpingoophrectomy if young patient • TAH+BSO if the patient is > 40 years

2 - Sertoli cell tumour: • • Rare solid tumour. Mean age 58 years old Cut section yellowish or red Well differentiated and benign Symptoms: abnormal periods hirsutism vlirization Reinke cristaloid Treatment: Unilateral salpingoophrectomy

NOS • • • Lipoid tumor 43 -60 years old Secrete androgen Early maturity and virilization Yelowish to black Size: 5 -8 cm Treatment 1 a: USA TAH+BSO

epithlial ovarian malignant tumor cidence of epithlial ovarian cancer: • Epithelial Ovarian cancer is the most common ovarian cancer 80 -90%
 Nulliparity infertility Ovulatory")
Risk factors: • • • Increasing age (up to 60 y) Nulliparity infertility Ovulatory induction drugs Late menopause early menarche Familial ovarian cancer colon& Breast cancer Strongly correlated Non asiatic race

Protective factors: • bilateral TL • TAH • Oral contraceptives: protective due to suppression of ovulation

Symptoms: • • • Abdominal distention Loss of weight Abdominal pain Constipation, nausea, diareha Large tumors may cause a sensation of pelvic weight or pressure • Early satiety

Lab test: • • CA 125 best TM for epithelial tumors CXR for pleural effusion 10% Mamography Songraphy
 Bilateral Metastasis when is diagnosed")
Serous adenocarcinoma : • • Most epithelial tumor(40 -50%) Bilateral Metastasis when is diagnosed Smooth, cystic, multilocular and concist bloody fluid • Psammoma bodies(irregular calcifications)

Mucinous adenocarcinoma • • Intestinal-like cells 5 -10% epithelial ovarian cancer 5 -30 cm Multilocular, solid-cystic

Endometrioidadenocarcinoma • • Second most common epithelial cell tumor 1/3 of patient has endometriosis 20% of patient has endometer adenocarcinoma Small, superficial associated with endometer hyperplasia • Solid-cystic

Clear cell carcinoma • 5 -10% epithelial ovarian tumor • Associated with endometriosis

Undifferentiated carcinoma: • Different patterns may coexist in different areas of the same tumours • Poor prognosis

Surgical diagnosis & treatment: Surgery is the primary method of diagnosis & treatment of ovarian cancer • Every patient who is medically fit for surgery should undergo exploration even if extra-abdominal metastasis have been demonstrated. • USO with complete staging in patient with satage 1 a who want to be pregnant • Other patient TAH+BSO

Second look laparotomy & laparoscopy: • It is a planned re-operation or laparoscopy to evaluate the effectiveness of treatment especially after chemotherapy in a patient with no clinical evidence of disease. Nowadays, it is largely replaced by modern imaging techniques and CA 125

chemotherapy • Stage 1 a or 1 b with grade 1 or 2 no needs chemotherapy • Satge 1 a or 1 b with grade 3 or 1 c or higher needs chemotherapy • Chemotherapy with platiniun base • Intraperitoneal treatment
- Slides: 93