Ovarian Stimulation An overview BY Mohammad A Emam

Ovarian Stimulation An overview BY Mohammad A. Emam Prof. of Obstetrics and Gynecology Mansoura Faculty of Medicine Mansoura Integrated Fertility center (MIFC) EGYPT 2005 www. ivfmifc. com

Indications • Some cases of primary amenorrhea. • Some cases of POF. • Some cases of delayed puberty. • Infertility ( anovulatory or ovulatory cycles).

Objective • To highlight the rationale , philosophy and different protocols of ovarian stimulation in cases of infertility

Introduction • First child, Louise brown 1978 was the product of ovulation in a sopontaneous cycle (Steptoe & edwards) • First I. V. F pregnancy using ovarian stim. Was ectopic.

Ov. Stim. Vs Spontaneous cycle - Advantages of spontaneous cycle ovulation: Avoidance: - Endocrine abnormalities - Luteal phase defect (LPD) -Advantages of ovarian Stimulation: – Avoidance Low pregnancy rate (single pre - ovulatory follicle. –Avoidance Difficulty of monitoring a spontaneous cycle(need 24 hs) – oocytes embryo pregnancy.
: • Major advances in understanding")
Advances in Ov. Stim. Over the past decade (Triad): • Major advances in understanding of ovarian physiology. • New medical technologies for management of infertility(GNRH analogue , self administered). • New Monitoring techniques(TVS replace Laparoscopy). Simplifying procedure + improving results.

Ovarian physiology Two roles – gametogenic – endocrine • The gametogenic potential is established early in the fetus • Endocrine role of the ovary is not realized until puberty
= (Apoptosis). Only")
Physiological Key Points Each Month: 600 – 650 occytes are destroyed (Atresia)= (Apoptosis). Only one oocyte ovulate HOW?

Physiological Key Point Normally : A cohort of primordial follicles Continuously intiating follicular growth (Independent of Gn stim. = intrinsic mechanism) Preantral stage Ov. Stim Disturb mechanism Need FSH in appropriate level Pre- ovulatory stage E + FSH receptor content Dominant follicle E FSH atresia of less developed foll. s Many follicles

Philosophy of Ovarian Stimulation 1. Induction of a single dominant follicle. 2. Induction of small number of follicles (1 -4). 3. Multiple follicular development (IVF&ICSI)
. 2.")
Factors guiding Ovarian Stimulation 1. Clinical circumstances( age , wt …. . ). 2. Aim: • Office therapy + timed Sex. I. • IUI • IVF or ICSI. 3. Number of eggs needed.

Types of Ov. Stimulation 1. Induction of ovulation. 2. Superovulation. 3. Controlled ovarian hyperstimulation (COH).
")
Induction of Ovulation • Use of medications to stim. Development of one (? ) or more mature follicles in anovulatory cycles.

Superovulation Intentional Production of many mature follicles in one cycle triggered by medication that stim. Ovaries early in follicular phase.
 Regulated Superovulation by turning off the patient’s own Hs (down")
Controlled Ov. Hyperstim. (COH) Regulated Superovulation by turning off the patient’s own Hs (down regulation) followed by stim. Aim: 1. Multiple follicles growth. 2. Control timing of ovulation eggs can be surgically retrieved before they are ovulated. 3. Prevention of premature LH surge.

Drugs for Ov. Stim. • cc • Gonadotrophins: • HMG • highly purified ur FSH • Rec LH • Gn. RH (pulsatile). • Gn. RHa (intranasal-S. C- I. M) • Gn. RH ant (involved in final steps of oocyte maturation). • HCG & Bromocripitine (!? )

CC • Competitive inhibitor of E 2 blocks E receptor in hypothalamus. Gn. RH FSH & LH. Follicles • After last tablet by one W: Freeing of hypothalamus receptors from blockage. Trigger LH surge (response to E 2).
 1 - long lasting(till 14 -22 day of cycle) cycle 2")
Problems with (cc) 1 - long lasting(till 14 -22 day of cycle) cycle 2 - subclinical pregnancy loss compared to normal population 3 - LH sec > FSH miscarriage 4 - (LUF)syndrome(unexplained infertility) infertility 5 - Anti E(cx &endometrium) &endometrium 6 - ectopic (tubal transport) 7 - side effect : -Minor (nausea-vomiting-flush skinhair loss) loss OHS Multiple pregnancy.

Gonadotropins Unlike CC – Gn acts directly on the ovaries.

Advantages of Recombinant Human Gonadotropins • Better batch-to-batch consistency. • Steady supply. • A purified compound. • Well tolerated. • No antibodies formation.
. -Half life time")
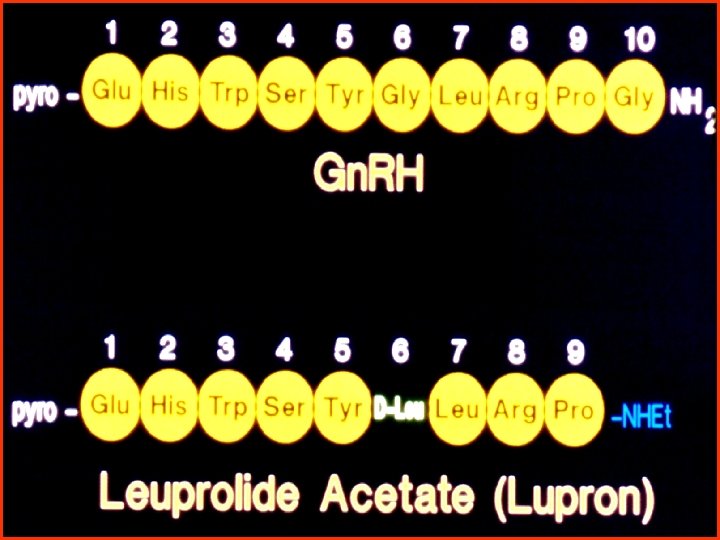
Gn. RH Natural -Is a deca peptide ( ten AA ). -Half life time is 8 min (10 min bursts every 60 min) Synthetic - By selective A. A or ethylamide substitutions at 6 and/or 10 (Gly) postions. - affinity for Gn. RH receptors (100 -200 times). - 1/2 life to 5 hours.

Gn. RHa Advantages • Prevent the possibility of premature LH surges (as a result of E in response to Gn) cancealed cycles. • Suppression of endogenous basal LH levels recruitment of a larger cohort of follicles. • Decrease LH stimulation of ovarian androgen production (may interfere with follicular development) Allow better timing of oocyte retrival &synchronise follicular growth.

Gn. RHa Routes: - Intranasal. - S. C. - Depot (Longer period + need higher doses Gn+ need more luteal support) (Devreken et al , 1996). Effect: - Agonistic (flare up) phase LH & FSH. - Down regulation (on continuous administration) Within two weeks).

Gn. RH Antagonist • Chemically it is also a decapeptide with changing the aminoacid sequense at positions 1, 2, 3, 6 and 10. • When Gn. RH antagonist is applied for short period it leads to abortion of LH peak, diminished E 2 production and impairment of follicular growth.

How to induce a single dominant follicle?

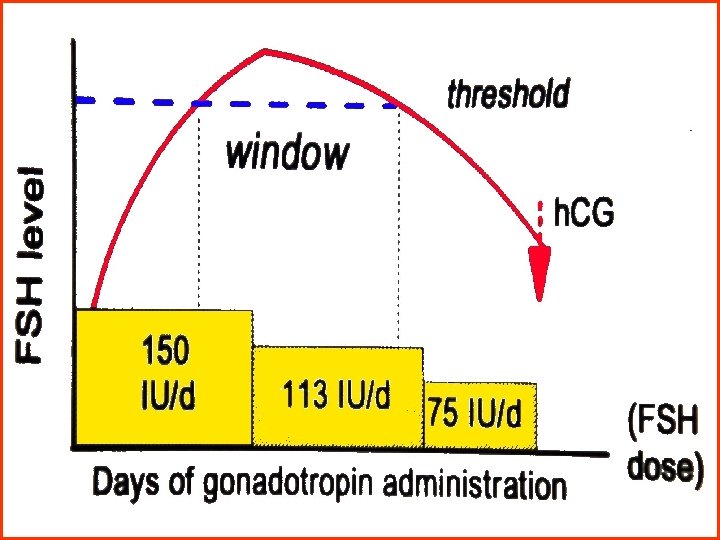
Induction of a Dominant Single Follicle? ! • Induction ovulation protocol which mimic more closely the FSH threshold and window of the natural cycle? !. Low dose step down Gn. Stim. Regimen.

Low dose Step-down regimen h. CG 2 FSH/d 1½ FSH/d 2 -3 3 -4 amp. D 7 2 -3 days Day 33 3 -4 U/S U/S & & E 2 Foll >11 mm mm FSH dose may be high or low: • Need to dose by one ampoule. 1 FSH/d
")
How to Obtain Small Number of Follicles (1 -4)

protocols 1. 2. 3. 4. 5. CC. CC ± FSH or ± HMG. Gn. Standard step-up protocol. Gn. Low dose step-up, stepdown protocol.

Unripe follicle Ripening follicle Ovulation Corpus luteum Regression of Corpus luteum Oocyte mature Clomiphene 100 mg day 2 for 5 days Gonadotrophin stimulation from day 4 to day of HCG 38 hrs HCG Leading follicle > 18 mm

Standard Step-up Protocol Starting dose = 150 IU/day Follicle > 12 mm E 2 > 400 U If Continue 2 FSH/day U/S and E 2 3 FSH/day for 3 more days Endocrine Rev. 1997; 18: 71
 OHSS (14%)")
Standard Step-up Protocol cont… Complications : Multifetal pregnancy (36%) OHSS (14%)

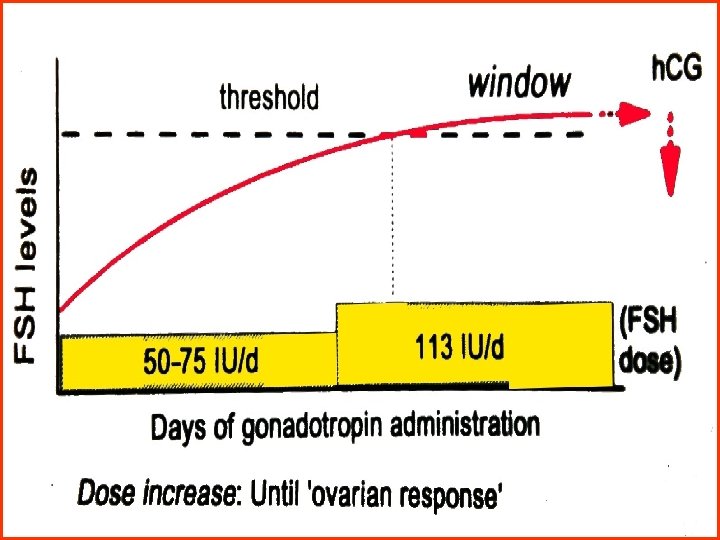
Low dose Step-up regimen It allows the FSH threshold to be reached gradually, minimizing excessive stimulation decreasing the risk of multifollicular response.

Low dose Step-up regimen Starting dose = 37. 5 -75 IU/day 37. 5 -75 FSH/h. MG/day Day 33 55 days Day 77 Follicle > 12 mm E 2 > 400 US If Continue 1 FSH/day no response 1. 5 FSH/day for 1 more week (max. 3 amp. ) Endocrine Rev. 1997;

Low dose Step-up Step-down regimen Day 3 one FSH/day step-up till 14 mm foll. step-down h. CG

Multiple Follicular Development

• Rationale of COH: To disturb the normal relationship between FSH&E by increase FSH available to follicles other than the dominant follicle increase total number of follicles that reach the pre ovulatory stage.
 • Production of sufficient number of very high-quality embryos (transfer 2")
Aim of (COH) • Production of sufficient number of very high-quality embryos (transfer 2 -3 embryo cycle) • Placement >3 : ( multiple pregnancy not pregnancy rate) • Freeze remaining embryos (for 2 nd use & decrease number of stim. Cycles) Cycles
 Programes • Transient neurological disturbances (6%). • Ovarian cysts")
Complication of Gn. RHa (COH) Programes • Transient neurological disturbances (6%). • Ovarian cysts (14 -29%). • Multiple pregnancy. • OHSS. • Hypoestrogenic effect? ! • Short luteal phase.
: utilizes pituitary desensitiz. suppression Shorter")
Protocols for Multiple Follicular Development • • Long (suppression): utilizes pituitary desensitiz. suppression Shorter duration Short (flare –up) Lower doses Ultrashort(sequential): sequential difficult timing and program Modifications - Microdose flare up. - Stop over technique (Norfolk protocols) - Step down regimen. • Gn. RH antagonist.

Flare Protocol Gn. RH-a h. MG Follicular phase Downregulation Gn. RH-a h. MG Gn. RH-a Luteal phase Downregulation h. MG Ultrashort Protocol Gn. RH-a h. MG 21 1 2 h. CG Cycle day Oocyte Retrieval Embryo Transfer

Pre-Requisites for COH Pattern of Response to COH: FSH on cycle day 3 (provided E 2 < 50 pg/ml) ØLow responder (FSH>15 miu/ml) ØIntermdiate responder (FSH 1015 miu/ml). ØHigh ( FSH <10).
: ØGood in intermediate & high responders.")
Selection of Protocol According to Responders Long (luteal): ØGood in intermediate & high responders. Short: (Flare up) protocol: ØGood in poor responder. Winslow, 1991

Long Protocol Criteria of Pituitary Suppression Ø Serum LH< 2. Ø Serum Estradiol < 50 pg/ml. Ø Absence of ovarian cyst. Ø Transvaginal sonographic measurement of endometrial thickness of <6 mm predicts pituitary down- regulation in over 95% of cases.
 substitutions • 2 x 100 mgm")
Support of Luteal Phase Direct: Direct (progesterone substitutions) substitutions • 2 x 100 mgm supp. or micronized 3 -6 x 100 (from day of embryo transfer). Indirect: Indirect (HCG) - Hyperstim - False pregnancy test.

Protocols of GNRH Antagonist

HMG or FSH on day 2 -3 of the cycle + Two Protocols of Antagonist Lubeck ( multiple doses) doses (0. 25 mg. S. C - 7 th day of the cycle till the day of HCG). French: (Single dose) dose ( 2 -3 mg as single or dual around day 9). NB: Another “soft protocol”= FSH + Gn. RH ant.

Advantages of Gn. RH antagonist 1. Immediate suppression of endogenous FSH and LH without flare up phenomenon. 2. Shortening treatment period with relief of physical, psychological and financial burdens. 3. Decreased number of HMG ampoules per cycle (Diedrich et al, 1994 and 2000).
")
Lubeck ( multiple doses)
 Vs Gn. RHa Metaanalysis Cycle Day 6 Day 2 -3 of FSH")
Antagonist (Lubec) Vs Gn. RHa Metaanalysis Cycle Day 6 Day 2 -3 of FSH Day of h. CG FSH Gn. RH antagonist Cycle Day 21 -24 Down Regulation 2 -4 Weeks Day of h. CG Gn. RH agonist FSH
 Vs Gn. RH-a Metaanalysis “Inany, 2002 ” • No significant difference in")
Antagonist (Lubec) Vs Gn. RH-a Metaanalysis “Inany, 2002 ” • No significant difference in prevention of LH surge. • Lower number of oocytes retrieved. • Lower pregnancy rate in spite of transfer of an equal number of embryos. • No significant difference in prevention of severe OHSS.
. High serum E 2. Multiple follicles. Younger")
Patients at Risk OHSS PCOS HCG (Exo/Endo). High serum E 2. Multiple follicles. Younger age < 32. Gn. RH-a protocols

Prevention of OHSS ü Withholding HCG administration. ü Reduced dose of HCG. ü Administration of rec-LH. ü Freeze the embryos. ü coasting

Conclusions • You should know what is you need from ov stimulation before selecting a certain protocol

Conclusions 1. Long protocols: they are the golden standard for all ART candidates especially those with young age, normal base line pituitary hormones, average size ovaries (more than 3 ml) and normal BMI. 2. Short protocols: they are used in ART candidates with previous poor response, older women with relatively high FSH.

Conclusions cont… 3. Cases of poor response with short protocols, ovaries are stimulated either without analogues (ie HMG alone) OR with the usage of antagonist.

Telfax 0020502319922 & 0020502312299 Email. mae 335@hotmail. com www. ivfmifc. com
- Slides: 60