Ovarian Involvement by Metastatic Colorectal Adenocarcinoma Still a

Ovarian Involvement by Metastatic Colorectal Adenocarcinoma Still a Diagnostic Challenge Michael R. Lewis, MD, Michael T. Deavers, MD, Elvio G. Silva, MD, and Anais Malpica, MD Am J Surg Pathol 2006; 30: 177– 184
.")
Introduction Ovaries, an anatomic site prone to involvement by metastatic colorectal adenocarcinoma(3. 4% ). n Most: a diagnosis of colorectal carcinoma would prior to the recognition of an ovarian lesion. n Occasionally, an ovarian mass is the initial manifestation of disease clinical management may be adversely affected (both therapeutically and prognostically). n

Introduction Overlap between the gross and histologic features of metastatic colorectal adenocarcinoma and those of primary epithelial ovarian neoplasms, especially endometrioid adenocarcinoma. n We reviewed 86 cases of ovarian involvement by metastatic colorectal adenocarcinoma, to analyze their clinical and pathologic features, to facilitate correct classification of these lesions. n

MATERIALS AND METHODS n n 86 cases were retrieved from Pathology Department of the University of Texas Anderson Cancer Center. From january 1, 1995 to April 30, 2005. Diagnosis of metastatic colorectal adenocarcinoma was based on histologic features, clinical information, review of the colorectal primary for histologic similarity, review of immunohistochemical findings. The colorectal primary tumor was confirmed either histologically or by clinical means (imaging

MATERIALS AND METHODS Clinical features recorded included age, presenting symptoms, anatomic site in which malignancy was first clinically suspected, initial and subsequent treatment, additional sites of tumor involvement, and survival data. n Gross features included laterality, size, surface involvement, and characteristics on sectioning. n H/E stained sections of one or both ovaries involved by meta were reviewed in all cases. n

MATERIALS AND METHODS In 13 of the 48 cases with bilateral involvement, sections of only one ovary were available for review a total of 121 ovaries were reviewed. n Sections number averaged six, range of 1 to 31. n Immunohistochemically stained for CK 7, CK 20, CEA, CDX 2 were available in 30, 29, 7, 6 cases. n

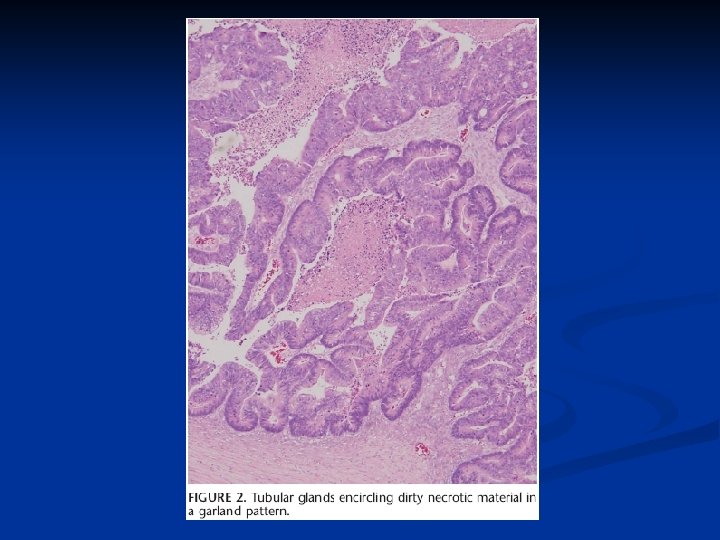
MATERIALS AND METHODS Architectural patterns n Dirty necrosis n Garland pattern (cystic glandular structures containing necrotic debris encircled by an array of round tubular glands) n Segmental necrosis of malignant epithelium n The presence of epithelium with mucinous cystadenoma or mucinous neoplasm of low malignant potential (ie, non-carcinomatous epithelium) n Evidence of surface involvement. n
;")
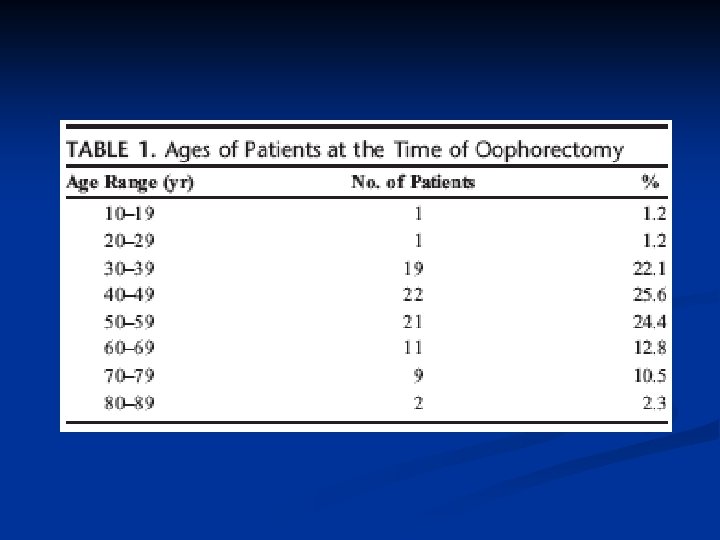
RESULTS n Clinical Features : age from 19 to 85 years (mean, 51 years); 24% were under the age of 40 n Abdominal pain: 36 pelvic pain : 9 Changes in bowel habits : 20 bleeding per rectum : 13 fullness or bloating : 8 fatigue or weight loss : 9 nausea and vomiting : 3 vaginal bleeding : 5 asymptomatic : 6 pelvic mass : 3 heme-positive stools : 2

Primary Colorectal Tumors sigmoid colon : 38 rectum : 9 cecum : 9 ascending colon : 12 transverse colon : 14 descending colon : 2 n T 3 : 58, T 4 : 17. One : T 1 NX at the time of resection. CT scan of the pelvis 37 months after the colonic resection. n 29 had 4 or more nodes N 2. n 81% had other involvement. Omentum : 59 n

Gross Features of Involved Ovaries 24% ovarian mass measured at least 10 cm in greatest dimension. Ranged from 2 to 24 cm (mean, 10. 1 cm) n Most were described as solid and cystic. n Among the 46 cases for which data were available, 21 featured an ovary with evidence of surface involvement by tumor, and 7 showed evidence of surface rupture. n

Histologic Features n Large glands lined by columnar epithelial cells with variable nuclear stratification, apical eosinophilic cytoplasm, and abundant mitotic figures, features similar to those of endometrioid adenocarcinoma.
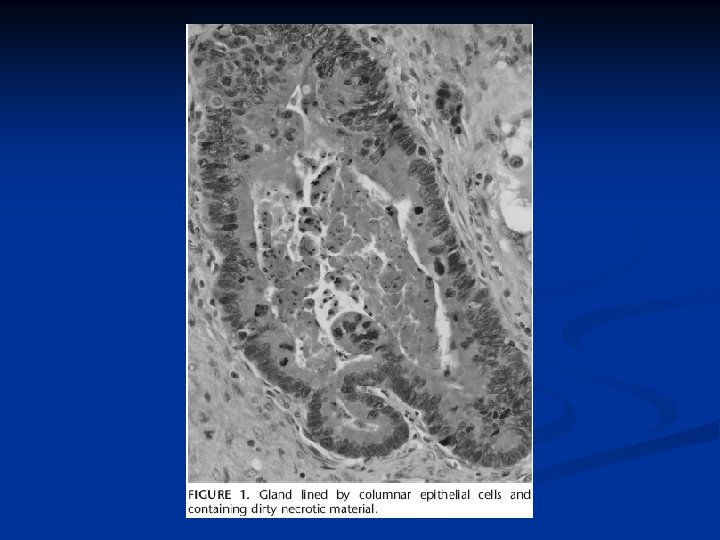

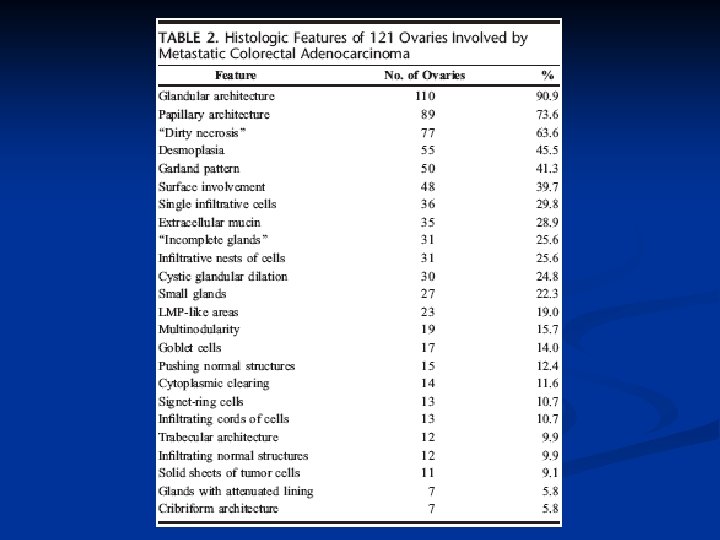
Histologic Features In 50 of the ovaries with glandular architecture, there were glands with features of the garland pattern classically associated with colorectal metastases. n The presence in glandular lumina of necrotic material containing karyorrhectic debris was not restricted to glands with the garland pattern; so-called “dirty necrosis” was identified in 77 of the 121 ovaries. n
. n The papillae")
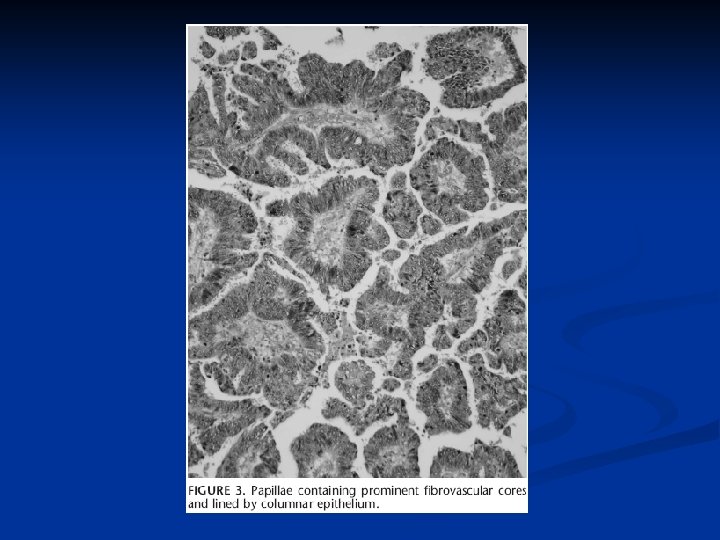
Histologic Features Papillary architecture was also frequently noted (89 of 121). n The papillae were large, featured prominent fibrovascular cores, and were lined by epithelium similar to that described above in glandular foci. n

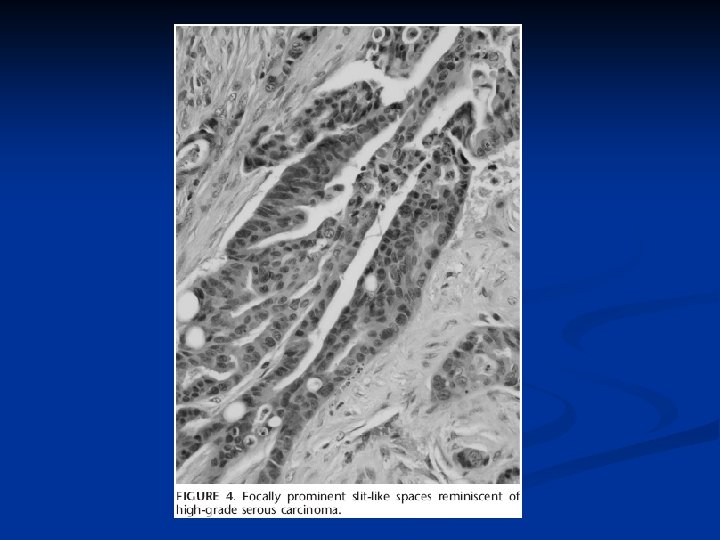
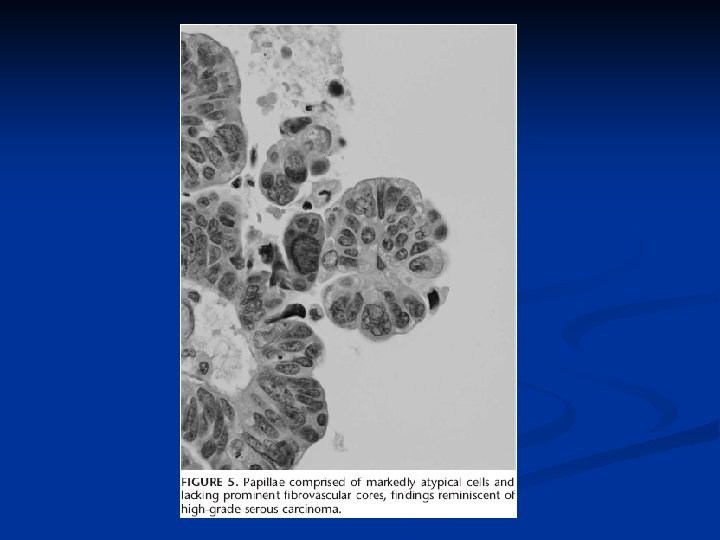
Histologic Features n In rare foci, small papillae composed of cells with marked nuclear atypia and lacking fibrovascular cores were seen and gave rise to slit-like spaces reminiscent of high-grade serous carcinoma.

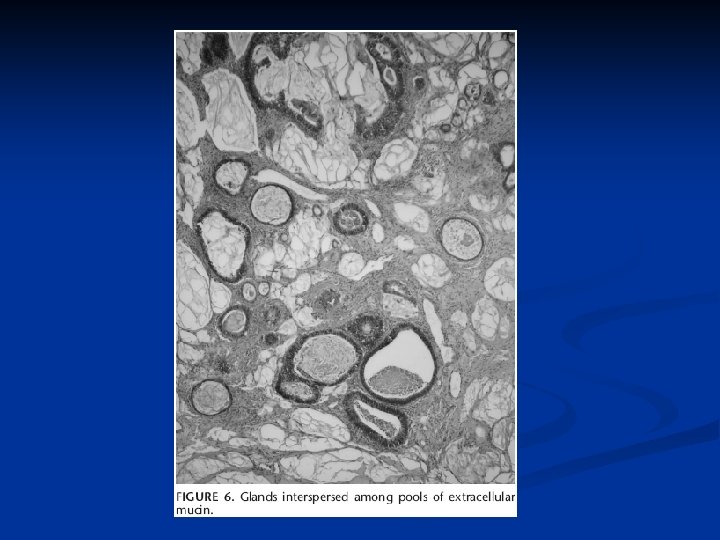
Histologic Features n Nearly 1/3 of involved ovaries had features of mucinous carcinoma. Pools of extracellular mucin were more common than prominent intracytoplasmic mucin, but goblet cells were identified at least focally in 17 ovaries (14%).
 contained areas in which the epithelium")
Histologic Features n 23 of the ovaries (19%) contained areas in which the epithelium had features similar to those of mucinous neoplasms of low malignant potential (borderline), and a few even had areas in which focally the cells had a benign appearance.


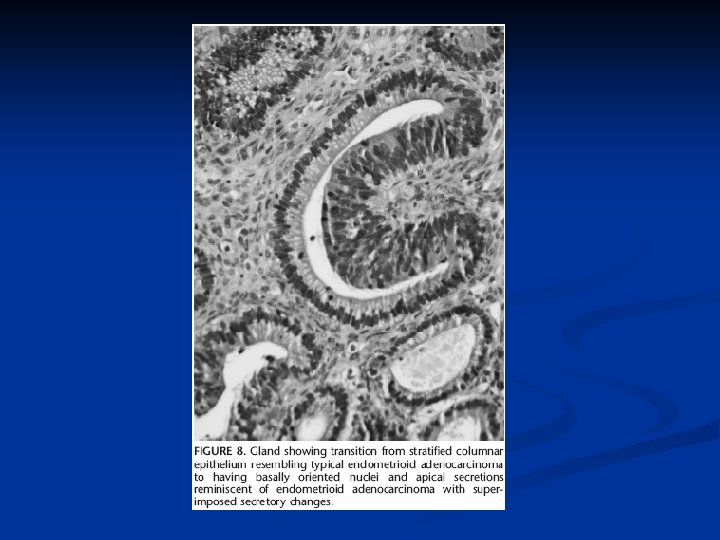
Histologic Features n 14 cases contained foci of cytoplasmic clearing yielding an appearance similar to that of endometrioid carcinoma with superimposed secretory changes

Immunohistochemical Findings Immunohistochemically stained sections were available for review in 30 cases. n CK 20 was positive in all 29 cases studied (100%) n Focal positivity for CK 7 was present in 5/30 cases (17%); the remaining 25 cases were negative. n Tumor cells expressed CDX 2 in 6/6 cases, villin in 4/4 cases, and CEA in 6/7 cases, with the 7 th CEA case showing equivocal staining. n

Frozen Section Diagnoses In 56 cases, a frozen-section diagnosis rendered. n Metastatic carcinoma was diagnosed, favored, or mentioned in 25 cases (45%). n In 10 cases (18%), a diagnosis of malignancy or adenocarcinoma was rendered. n A diagnosis of mucinous adenocarcinoma was in 8 cases. n An ovarian primary was diagnosed or favored in 13 cases: endometrioid carcinoma : 7, serous carcinoma : 2 n

Initial Diagnoses and Chemotherapy A primary ovarian malignancy was initially diagnosed or favored in 9 cases. n 6/9 initially received platinum-based chemotherapy typically used in cases of ovarian malignancy instead of standard chemotherapy for advanced stage colorectal adenocarcinoma. n

Follow-Up Follow-up data covering at least 6 months post -oophorectomy were available for 60 patients; 4 who died less than 6 months after diagnosis. n 37 patients died between 1 and 103 months after diagnosis (mean, 27. 4 months), 27 were alive between 6 and 73 months postoophorectomy. n 5/6 patients who received platinum-based chemotherapy were alive between 5 and 59 months post-oophorectomy. n

DISCUSSION Metastatic disease from extragenital primary tumors involves the ovary far more frequently than other sites within the female genital tract (3: 1), and approximately 1/3 such cases arises from colorectal primary tumors. n Mazur et al : ovarian lesions were identified prior to the primary tumor in 21 of 149 cases (14%). In our series, even higher (32%). n Many women in this series who presented prior to the age to screen for colorectal adenocarcinoma n

People between 20 and 40 about 3% of patients diagnosed with colorectal adenocarcinoma, but 23% in the present study. n The finding of disproportionate ovarian involvement in young women with colorectal adenocarcinoma, indicating a higher frequency of stage III or IV disease in young patients n An increased likelihood of referral of such women to our institution from nonspecialized centers. n

In our study, 99% had invaded through the muscularis propria into subserosa or beyond, keeping the experience of previous authors. n In the single case of T 1 disease, no lymph nodes were identified grossly for histologic evaluation. n Patients deemed to have “node-negative” colorectal tumors, survival increases significantly as the number of lymph nodes examined rises. n

About gross characteristics, our findings in some ways parallel those of earlier works. n Bilateral involvement somewhat more frequently than other authors (60% vs. 25%43%). n Recent works concerning metastatic mucinous tumors have suggested that ovarian masses measuring 10 cm or greater are more likely to represent primary mucinous tumors than metastases. n

The main histologic feature were glandular and papillary architecture, dirty necrosis, desmoplasia, and the garland pattern. n The combination of architectural and cytologic features often caused the lesions to resemble endometrioid or mucinous neoplasms; features reminiscent of serous carcinoma or clear cell. n 23(19%) of regions resembling ovarian mucinous neoplasms of low malignant potential (borderline tumors). n

This mimicry of the variability so closely associated with primary mucinous tumors poses a significant pitfall in correct diagnosis of metastatic lesions. n Surface involvement in 40% of the ovaries (and grossly in 46%), may be of assistance in distinguishing these lesions from primary tumors n Single-cell infiltration and the presence of signet-ring cells were strongly associated with metastases. n

The findings in the present study are most consistent with those previously reported with respect to CK 7 and CK 20. n In a majority of cases, primary ovarian neoplasms (with the exception of mucinous neoplasms) are (+) for CK 7 and (-) for CK 20; colorectal tumors are most frequently (-) for CK 7 and (+) for CK 20. n Metastases of colorectal origin have been found frequently to express CDX 2 n

One simply cannot be certain whether the tumor is a colorectal metastasis or an ovarian primary, if features associated with colorectal metastases, deferral with respect to site of origin is preferable to an unequivocal diagnosis of ovarian carcinoma. n If one knows of a previous colorectal tumor in a patient with such a lesion, sections of the colorectal tumor should be reviewed if at all possible. n

Inappropriate selection of chemotherapeutic agents may occur; platinum-based regimens standard in the treatment of ovarian malignancies, are not first-line therapy for advanced stage colorectal adenocarcinoma. n The provision of inaccurate prognostic information to the patient based on a diagnosis of stage I ovarian cancer instead of stage IV colorectal carcinoma may take place. n

Eighteen years ago, Lash and Hart noted that “accurate diagnosis of metastatic intestinal carcinoma continues to be a significant problem. ” n Our experience suggests that this observation remains valid. n Colorectal metastases exhibit gross and histologic features similar to those of various ovarian epithelial neoplasms, diagnostic difficulty may persist for some time to come. n

Our department 17 cases n Age: range from 28~84 years, mean 56. 7 years n Ovary involvement: bilateral: 7 right: 7 left: 3 n Colon site: sigmoid: 5 rectum: 4 ascending: 3 descending: 2 transverse: 1 n

Ovary size: range from 1. 8~20 cm mean: 8. 32 cm n Immunohistochemical study: 5/5, CK 20 (+) CK 7 (-) n

Thanks for your attention!
- Slides: 44