Outline Preterm Preeclampsia Gestational diabetes Postpartum hemorrhage Ectopic

Outline • • • Preterm Preeclampsia Gestational diabetes Postpartum hemorrhage Ectopic pregnancy Gestational emesis

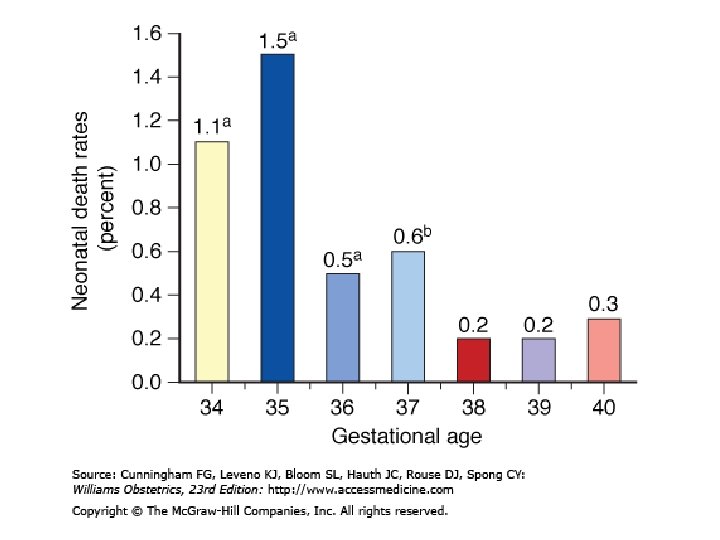
定義 • 早產:小於 37週出生 • • Late preterm = 34 to 36 weeks Moderately preterm = 32 to 34 weeks Very preterm = <32 weeks Extremely preterm = <28 weeks

• Low birth weight: <2500 g • Very low birth weight: <1500 g • Extremely-low birth weight: <1000 g

早產的影響 週數 24 25 26 存活率 40% 75% RDS 70% 93% ICH 25% 30% Sepsis 25% 29% 30% NEC 8% 17% 11% Intact 5% 50% 60% 27 28 29 30 31 32 33 34 80% 92% 93% 94% 95% 96% 97% 84% 65% 53% 55% 37% 28% 34% 16% 4% 3% 2% 2% 1% 0% 0% 36% 25% 11% 14% 3% 5% 4% 10% 25% 14% 15% 8% 6% 2% 3% 70% 85% 90% 93% 95% 96% 97%
 (n=426 6) 1001–")
Birthweight Groups Outcome 501– 750 g 1000 (n=404 g 6) (n=426 6) 1001– 1250 g (n=455 7) 1251– 1500 g (n=528 4) Overall survival (%) 55 88 94 96 Survival with complications(% ) 65 43 22 11 Bronchopulmonary dysplasia alone 42 25 11 4 Severe IVH alone 5 6 5 4 NEC alone 3 3 3 2 Bronchopulmonary dysplasia and severe IVH 10 4 2 <1
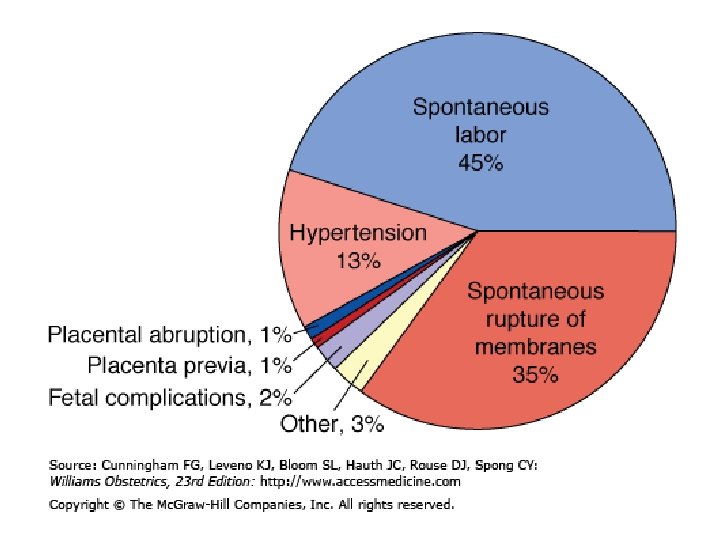
 • 孕婦及產科合併症 – Preeclampsia – Fetal distress – IUGR – Abruptio placentae –")
原因(1) • 孕婦及產科合併症 – Preeclampsia – Fetal distress – IUGR – Abruptio placentae – Fetal death
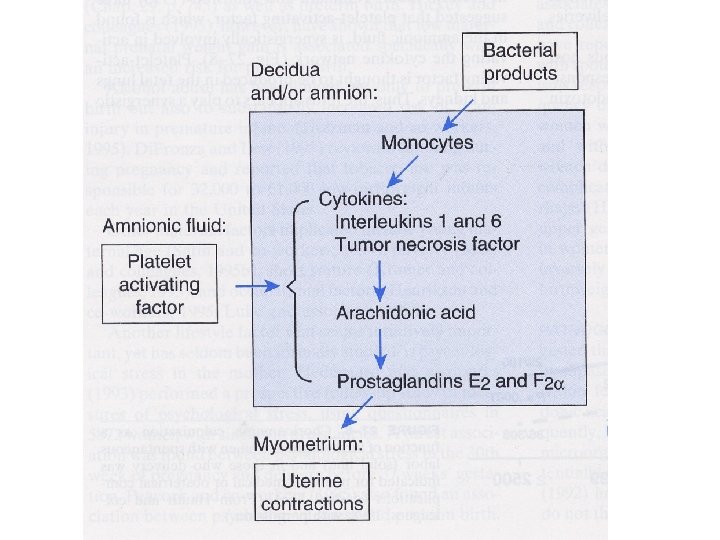
 • 羊膜炎 – 制病機轉 • Phospholipase A 2活化 • 細菌內毒素 • Cytokines: IL-1,")
原因(3) • 羊膜炎 – 制病機轉 • Phospholipase A 2活化 • 細菌內毒素 • Cytokines: IL-1, TNF, IL-6 • Platelet activating factor – 診斷
")
早產的危險因子 壓力 Single women Low socioeconomic status Anxiety Depression Life events (divorce, separation, death) Abdominal surgery during pregnancy 職業倦怠 Upright posture Use of industrial machines Physical exertion Mental or environmental stress

早產的危險因子 子宮過度擴張或受損 Multiple gestation Polyhydramnios Uterine anomaly Uterine leiomyoma Diethylstilbestrol 子宮頸的因素 History of second trimester abortion History of cervical surgery Premature cervical dilatation or effacement

早產的危險因子 感染 Sexually transmitted infections Pyelonephritis, appendicitis, pneumonia Systemic infection Bacteriuria Periodontal disease 胎盤病理學 Placenta previa Abruption Vaginal bleeding
 African-American")
早產的危險因子 雜項 Previous preterm delivery Substance abuse Smoking Maternal age (<18 or >40) African-American race Poor nutrition and low body mass index Inadequate prenatal care Anemia (hemoglobin <10 g/d. L) Excessive uterine contractility Low level of educational achievement Genotype

早產的危險因子 胎兒因素 Congenital anomaly Growth restriction
 % 早產的相對風 險(RR) 信賴區間(CI) ≤ 35 50 2. 35 1. 42 to")
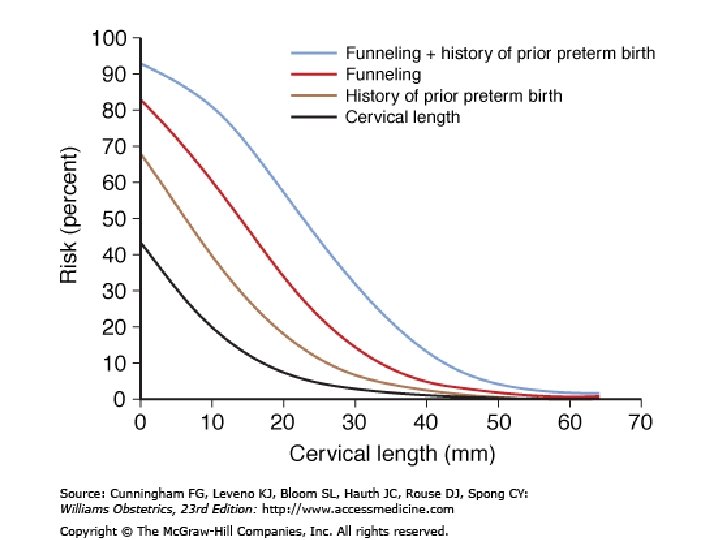
子宮頸長度 (mm) % 早產的相對風 險(RR) 信賴區間(CI) ≤ 35 50 2. 35 1. 42 to 3. 89 ≤ 30 25 3. 79 2. 32 to 6. 19 ≤ 26 10 6. 19 3. 84 to 9. 97 ≤ 22 5 9. 49 5. 95 to 15. 15 ≤ 13 1 13. 99 7. 89 to 24. 78
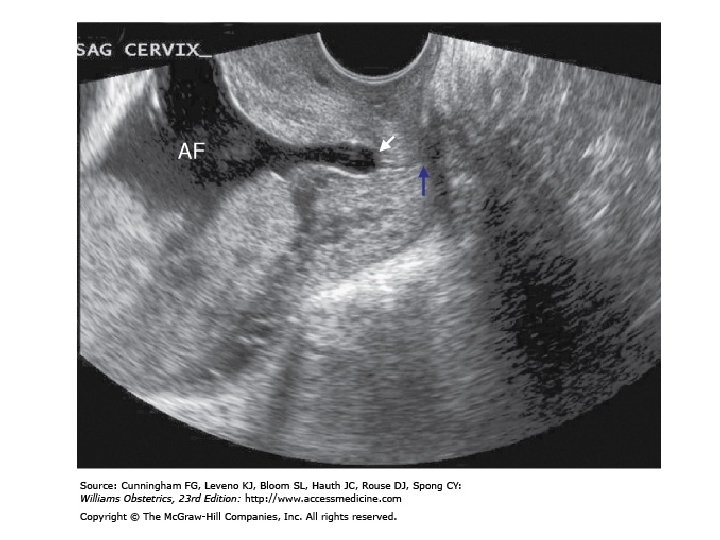

Recommended Screening Strategies to Prevent Preterm Birth • No current data support use of home uterine-activity monitoring or bacterial vaginosis screening. • Screening for risk of preterm labor, other than historical risk factors, is not beneficial in the general obstetrical population. • Sonography to determine cervical length and/or fetal fibronectin level measurement may be useful in determining women at risk for preterm labor. However, their value may rest primarily with their negative-predictive value given the lack of proven treatment options.

早期破水處置建議 妊娠週數 處置 >=34 週 • Proceed to delivery, usually by induction of labor • Group B streptococcal prophylaxis is recommended • Expectant management unless fetal pulmonary maturity is documented • Group B streptococcal prophylaxis is recommended • Corticosteroids—no consensus, but some experts recommend • Antimicrobials to prolong latency if no contraindications 32 -33 週

早期破水處置建議 妊娠週數 處置 24 -31 週 • Expectant management • Group B streptococcal prophylaxis is recommended • Single-course corticosteroids use is recommended • Tocolytics—no consensus • Antimicrobials to prolong latency if no contraindications

早期破水處置建議 妊娠週數 處置 < 24 週 • Patient counseling • Expectant management or induction of labor • Group B streptococcal prophylaxis is not recommended • Corticosteroids are not recommended • Antimicrobials—there are incomplete data on use in prolonging latency

初產婦 年齡>40歲 家族史 慢性腎病 慢性高血壓 抗凝脂質血症 糖尿病 多胞胎 高BMI Angiotensinogen gene T 235 Homozygous Heterozygous 3: 1 5: 1 20: 1 10: 1 2: 1 4: 1 3: 1 20: 1 4: 1

 • Situs inversus (84 x) • Spinal bifida,")
先天畸形 • Caudal regression (258 x) • Situs inversus (84 x) • Spinal bifida, Hydrocephaly, other CNS defect (2 x) • Anencephaly (3 x) • Heart anomaly (4 x) • Anal/rectal atresia (3 x) • Renal anomaly (4 x)
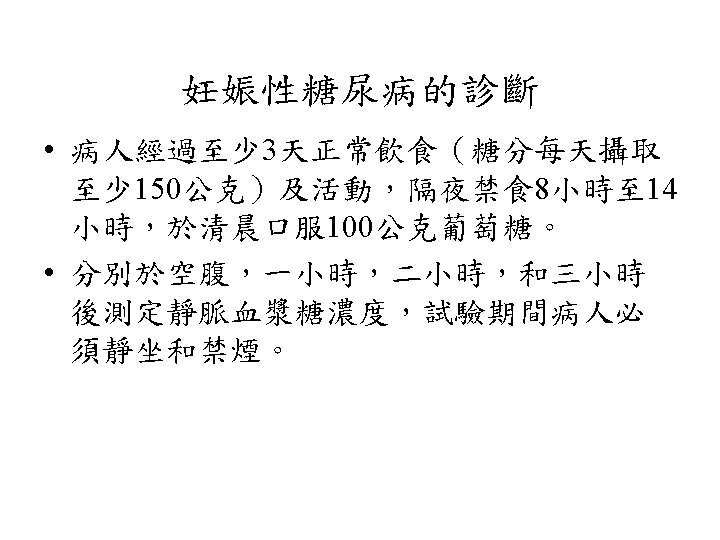

• BMI 22 to 27: 30 to 35 kcal / kg current weight / day • BMI 27 to 29 (overweight): 24 kcal / kg current weight / day • BMI >30 (obese pregnant women): 12 to 15 kcal / kg current weight / day • BMI < 22: 30 to 40 kcal / kg current weight / day

• carbohydrate intake be restricted to 33 to 40 percent of calories • the remainder divided between protein (about 20 percent) and fat (about 40 percent, primarily unsaturated fats)

• Breakfast — The breakfast meal should be small (approximately 10 percent of total calories) to help maintain postprandial euglycemia. Carbohydrate intake at breakfast is also limited since insulin resistance is greatest in the morning. • Lunch — 30 percent of total calories • Dinner — 30 percent of total calories • Snacks — Leftover calories (approximately 30 percent of total calories) are distributed, as needed, as snacks.

Insulin dosage and adjustment • Initial dose: 0. 6~0. 8 U/Kg IBW in the 1 st trimester 0. 7~0. 9 U/Kg IBW in the 2 nd trimester 0. 8~1. 2 U/Kg BW in the 3 rd trimester • Morning: 2/3 total dose with 2/3 NPH & 1/3 RI (ie: 20 u NPH +10 u RI) Evening: 1/3 total dose with 1/2 NPH & 1/2 RI (ie: 5 u NPH +5 u RI)
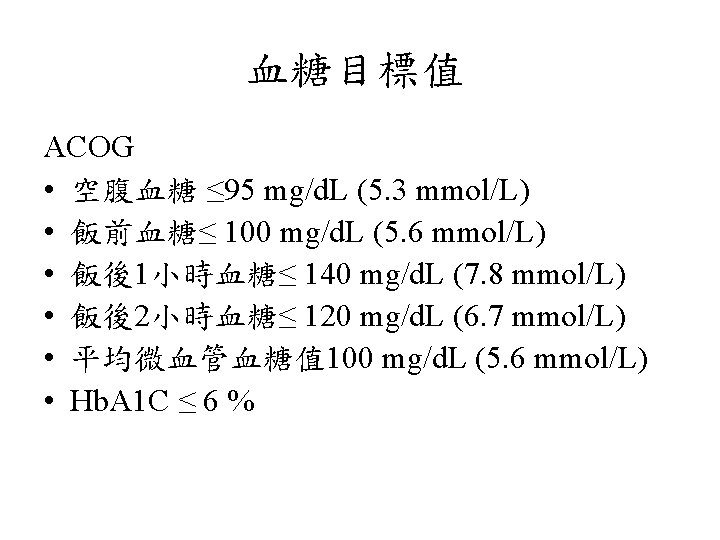

ADA • 飯前, 睡前血糖 60 to 99 mg/d. L (3. 3 to 5. 5 mmol/L) • 飯後最高血糖 100 to 129 mg/d. L (5. 6 to 7. 2 mmol/L) • Hb. A 1 C < 6. 0 %

待產中血糖 • The American College of Obstetricians and Gynecologists' and the American College of Endocrinology's goal • 70 to 110 mg/d. L (3. 9 to 6. 1 mmol/L).

Bimanual compression of the uterus

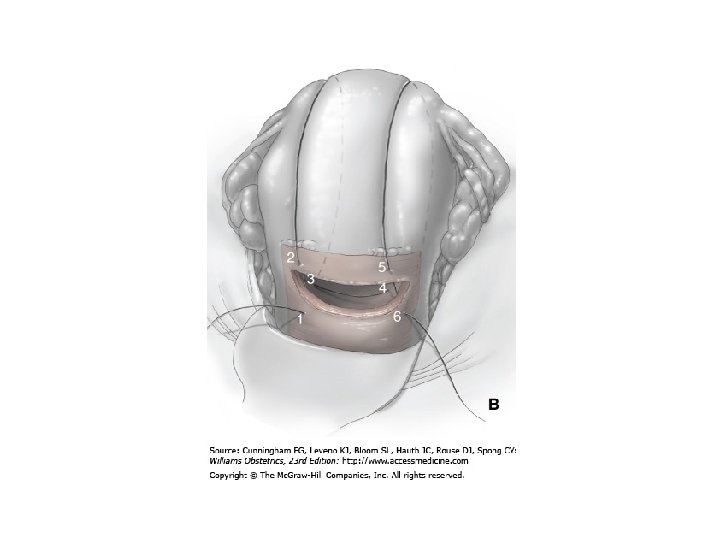
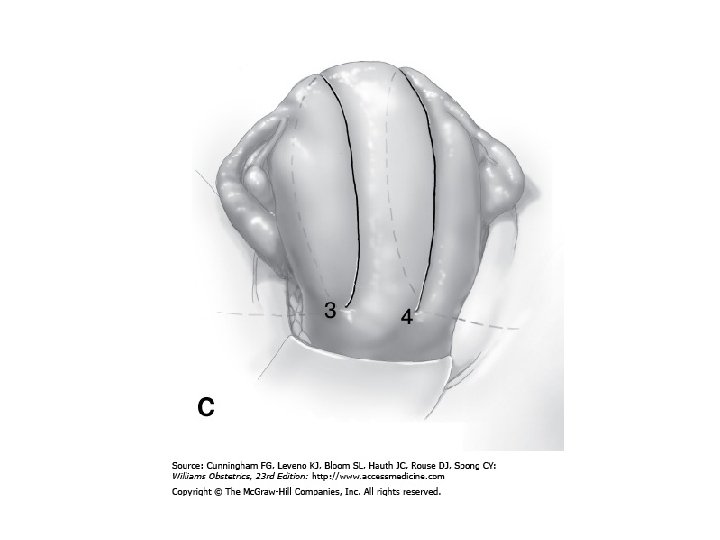
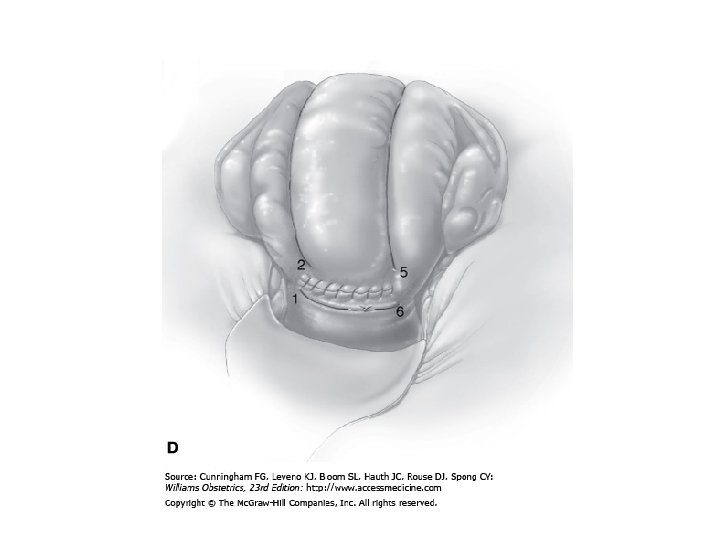
B-Lynch uterine compression suture

子宮填壓 • Bakri Postpartum Balloon

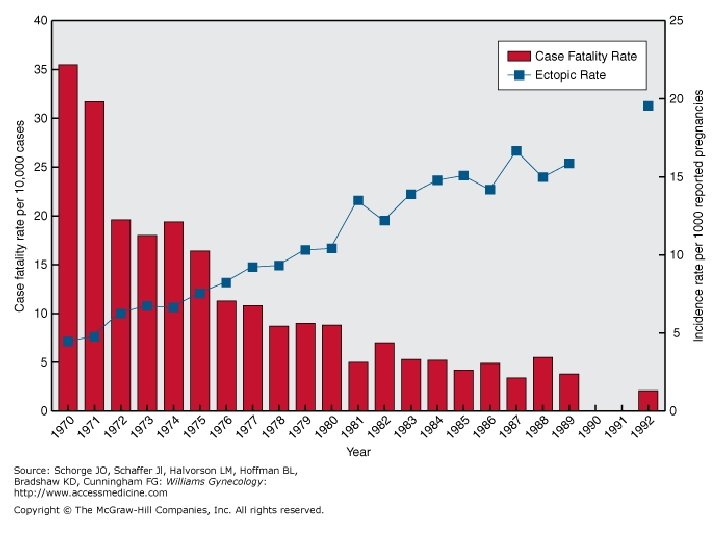
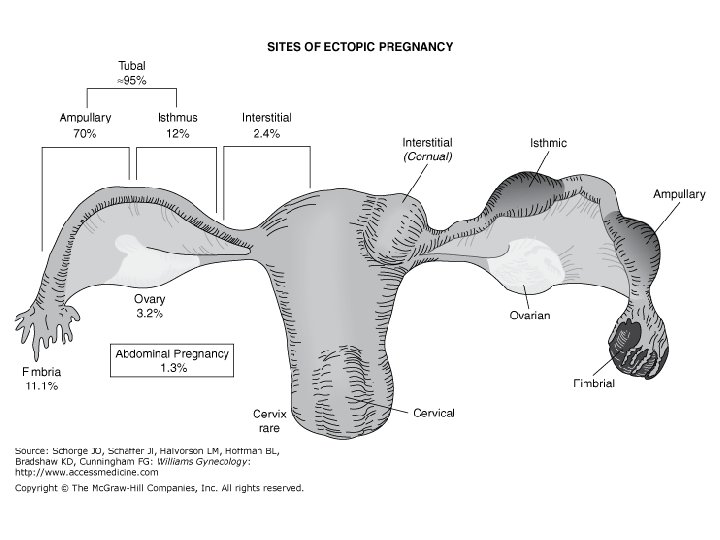
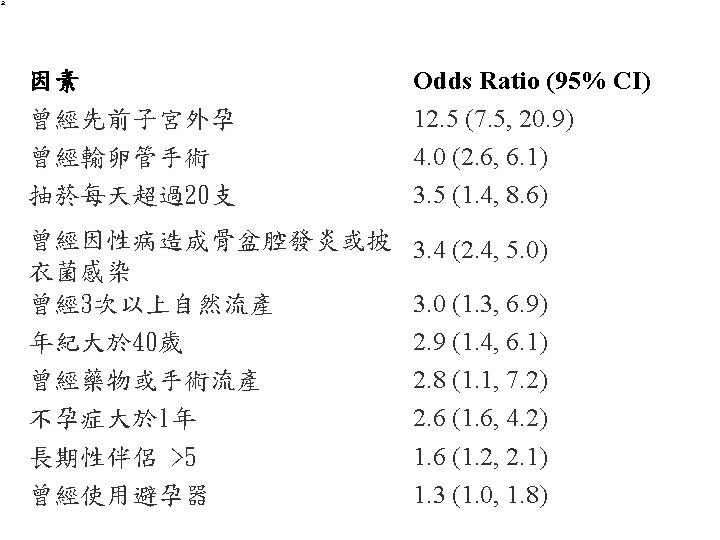
子宮外孕 • 發生率: 1. 3 -2% in US • 機率增加的原因 – STD-chlamydial infection – Tubal factor infertility


Culdocentesis

Interstitial pregnancy

• Cervical pregnancy • Heterotopic pregnancy • Cesarean scar pregnancy

Nausea and Vomiting in Pregnancy

The Clinical Problem • 50 % have nausea and vomiting in early pregnancy • an additional 25% have nausea alone • “morning sickness” • lead to dehydration and weight loss • hyperemesis gravidarum – Incidence 0. 3 to 1. 0 – characterized by persistent vomiting, weight loss of more than 5%, ketonuria, electrolyte abnormalities (hypokalemia), and dehydration (high urine specific gravity).

Stimulation produced by the placenta The onset of the nausea is within 4 weeks peaks at approximately 9 weeks of gestation. 60% resolve by the end of the first trimester 91% resolve by 20 weeks of gestation. less common in older women, multiparous women, and smokers; (smaller placental volumes ) • 63% of multiparous had symptoms in a previous pregnancy. • associated with a decreased risk of miscarriage. • • •
")
correlates closely with the level of human chorionic gonadotropin (h. CG)

• Women with twins or hydatidiform moles, who have higher h. CG levels • vitamin B deficiency may contribute, since the use of multivitamins containing vitamin B reduces the incidence of nausea and vomiting.

maternal complications of hyperemesis • gravidarum peripheral neuropathies due to vitamin B 6 and B 12 • Wernicke’s encephalopathy due to thiamine (vitamin B 1) deficiency. • triad of ophthalmoplegia, gait ataxia, and confusion, this condition may occur after at least 3 weeks of persistent vomiting. • intravenous dextrose without thiamine rapidly consumes the available B 1, triggering acute encephalopathy • have lower mean birth weights and lower percentile weights for gestational age, and they are more likely to be in less than the 10 th percentile of birth weight at delivery.

Infants of mothers who lost weight in early pregnancy • have lower mean birth weights and lower percentile weights for gestational age, and they are more likely to be in less than the 10 th percentile of birth weight at delivery.
,")
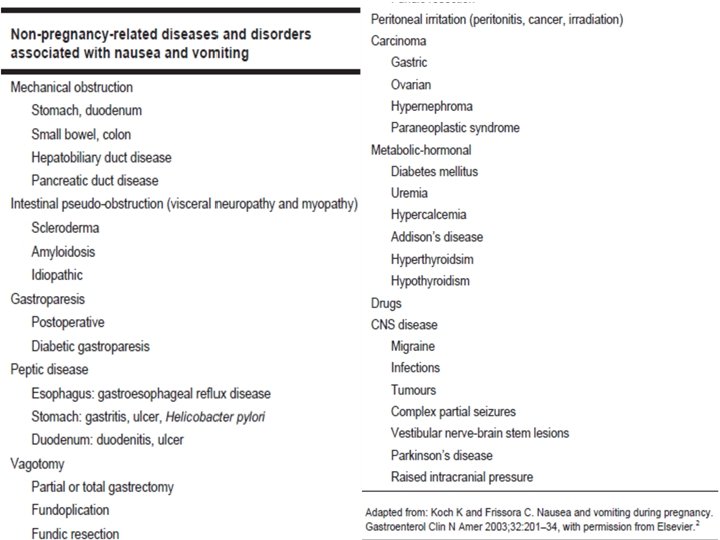
Evaluation • gastrointestinal conditions (e. g. , appendicitis, hepatitis, pancreatitis, or biliary tract disease), pyelonephritis, and metabolic disorders such as diabetic ketoacidosis, porphyria, or Addison’s disease. • An onset of nausea and vomiting more than 8 weeks after the last menstrual period is rare in pregnancy. • The presence of fever, abdominal pain, or headache is atypical in women with hyperemesis and suggests another cause.

Nausea and Vomiting in Pregnancy Is Not Always Nausea and Vomiting of Pregnancy • While causes of nausea and vomiting unrelated to pregnancy can occur at any time, preeclampsia, HELLP syndrome and acute fatty liver of pregnancy typically occur in the third trimester.

Signs • • changes in blood pressure and heart rate. fever meningismus tenderness, guarding, rigidity, peritoneal signs; right upper quadrant • jaundice.

Lab • urinary • ketones, blood urea nitrogen, creatinine, alanine aminotransferase, aspartate aminotransferase, • electrolytes, amylase • Ultrasonographic testing should be performed to detect multiple gestation or hydatidiform mole.

Management

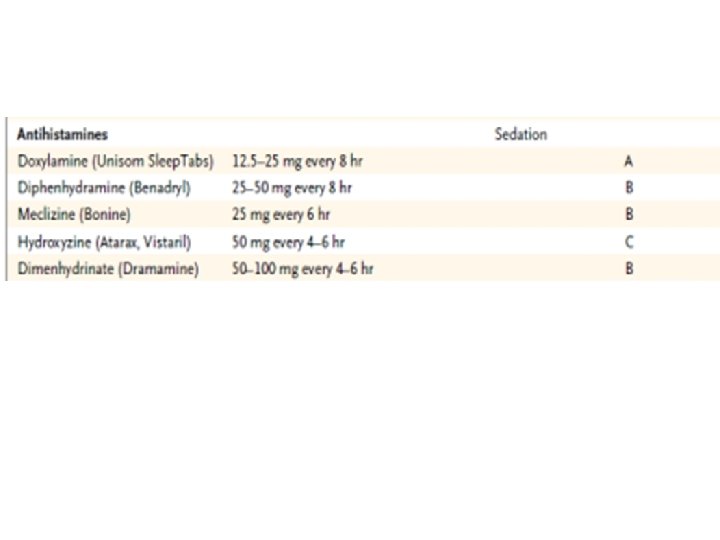
Pharmacologic Therapies • 10% of women with nausea and vomiting in pregnancy require medication

Management of Refractory Cases • Intravenous hydration and nutritional supplementation. • Enteral tube feeding • Total parenteral nutrition – substantial risk of line sepsis (25%); – steatohepatitis • reserved for clinically significant weight loss (>5% of body weight) and no response to antiemetic regimens or cannot be managed with enteral feedings.

Areas of Uncertainty • The cause or causes remain unclear. • The mechanism of action of vitamin B 6 is unknown. • data are lacking to identify factors predicting the response to therapies. • Vitamin B 6 levels do not predict the response to therapy with vitamin B 6.

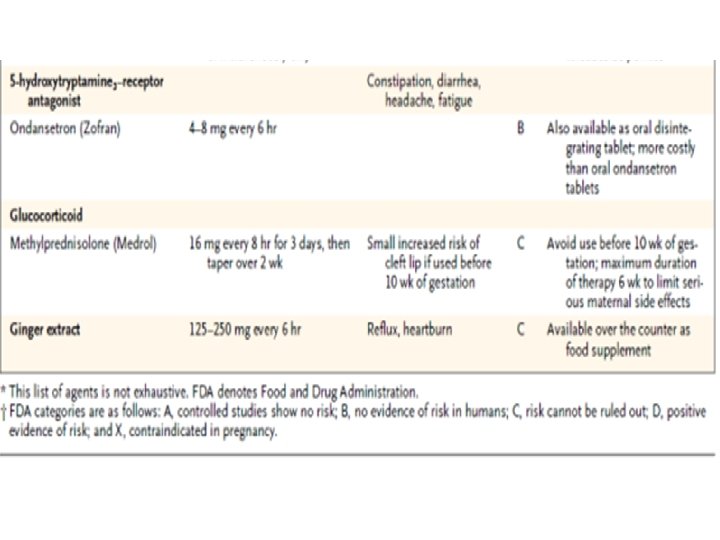
Conclusions and Recommendations • Consider other causes of nausea and vomiting in early pregnancy • Dietary advice • vitamin B 6 [pyridoxine], 10 to 25 mg every 8 hours, and doxylamine, 25 mg at bedtime and 12. 5 mg each in the morning and afternoon • Methylprednisolone should be reserved for refractory cases after 10 weeks of gestation. • Alternative remedies such as ginger and acupuncture may be tried at any time.

• intravenous fluid replacement with multivitamins, especially thiamine • If, after 12 hours of intravenous therapy, the vomiting continues, hospitalization may be required. • Enteral 48 or parenteral nutrition should be reserved for patients in whom weight loss continues despite pharmacologic therapies.

THE MANAGEMENT OF NAUSEA AND VOMITING OF PREGNANCY • 1. Dietary and lifestyle changes should be liberally encouraged, and women should be counselled to eat whatever appeals to them. (III-C) • 2. Alternative therapies, such as ginger supplementation, acupuncture, and acupressure, may be beneficial. (I-A) J Obstet Gynaecol Can 2002; 24(10): 817 -23.

• 3. A doxylamine/pyridoxine combination should be the standard of care, since it has the greatest evidence to support its efficacy and safety. (I-A) • 4. H 1 receptor antagonists should be considered in the management of acute or breakthrough episodes of NVP. (I-A) J Obstet Gynaecol Can 2002; 24(10): 817 -23.

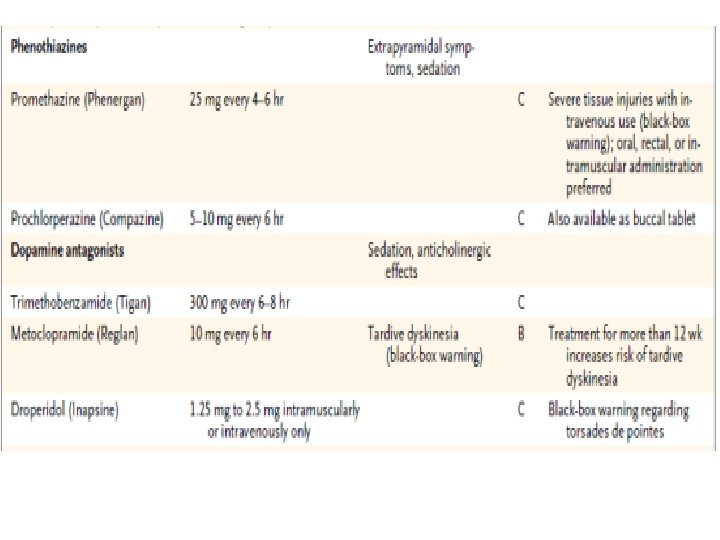
• 5. Pyridoxine monotherapy supplementation may be considered as an adjuvant measure. (I -A) • 6. Phenothiazines are safe and effective for severe NVP. (I-A) • 7. Metoclopramide is safe to be used for management of NVP, although evidence for efficacy is more limited. (II-2 D) J Obstet Gynaecol Can 2002; 24(10): 817 -23.

• 8. Corticosteroids should be avoided during the first trimester because of possible increased risk of oral clefting and should be restricted to refractory cases. (I-B) • 9. When NVP is refractory to initial pharmacotherapy, investigation of other potential causes should be undertaken. (III-A) J Obstet Gynaecol Can 2002; 24(10): 817 -23.
- Slides: 143