Outline Dementia and delirium facts and figures Patients















 • The diagnosis of delirium by CAM requires the presence")








- Slides: 36
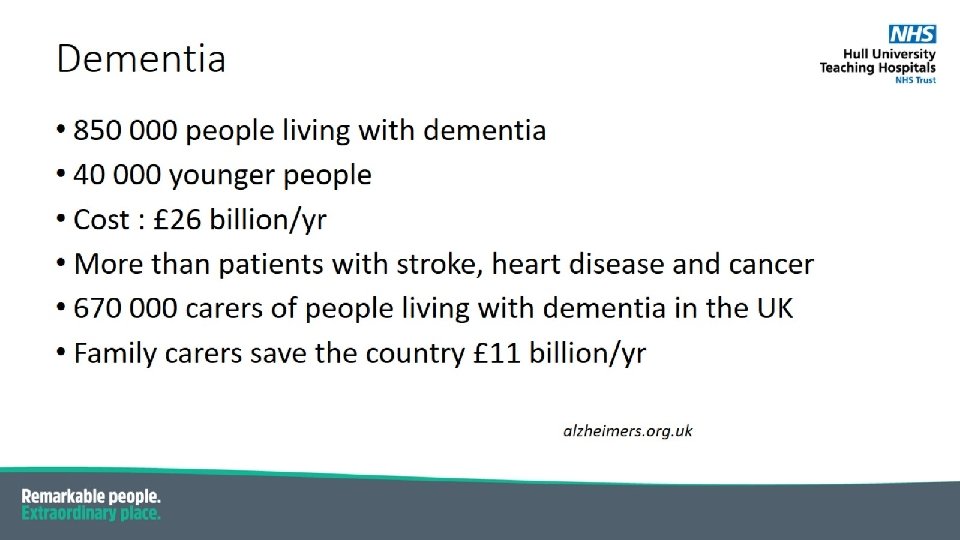
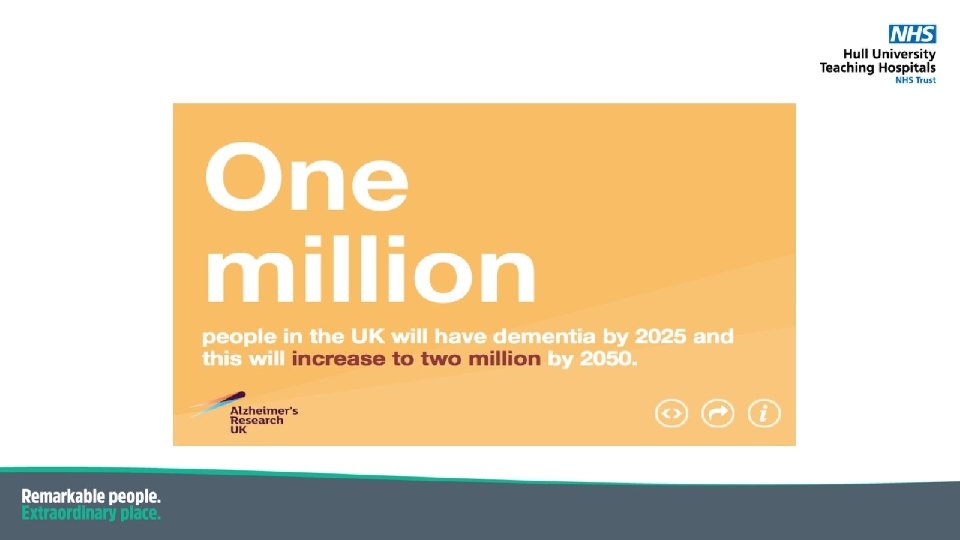
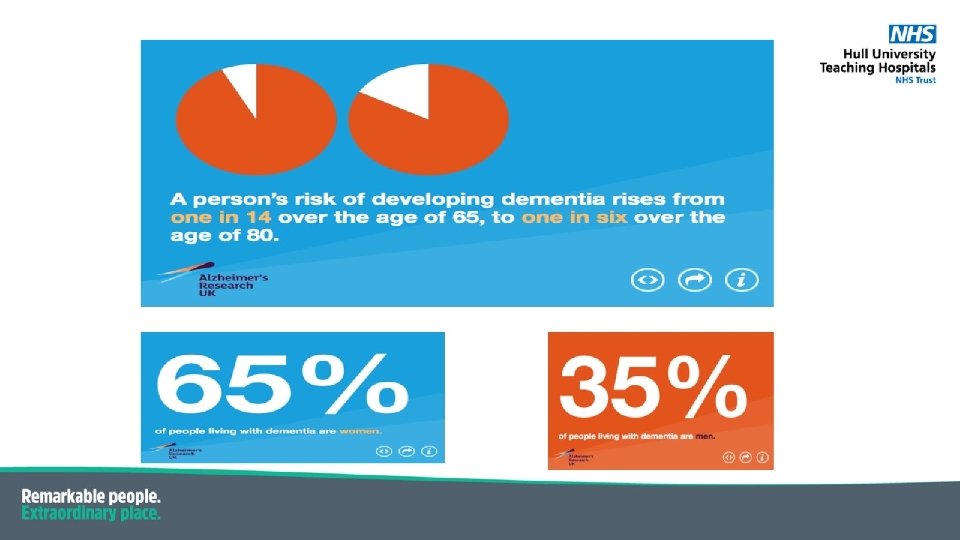
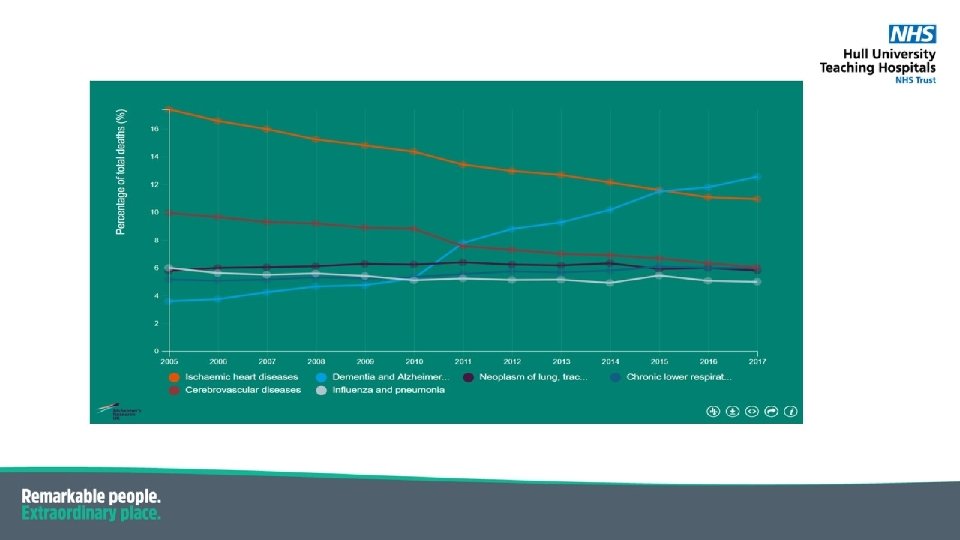
Outline • Dementia and delirium – facts and figures
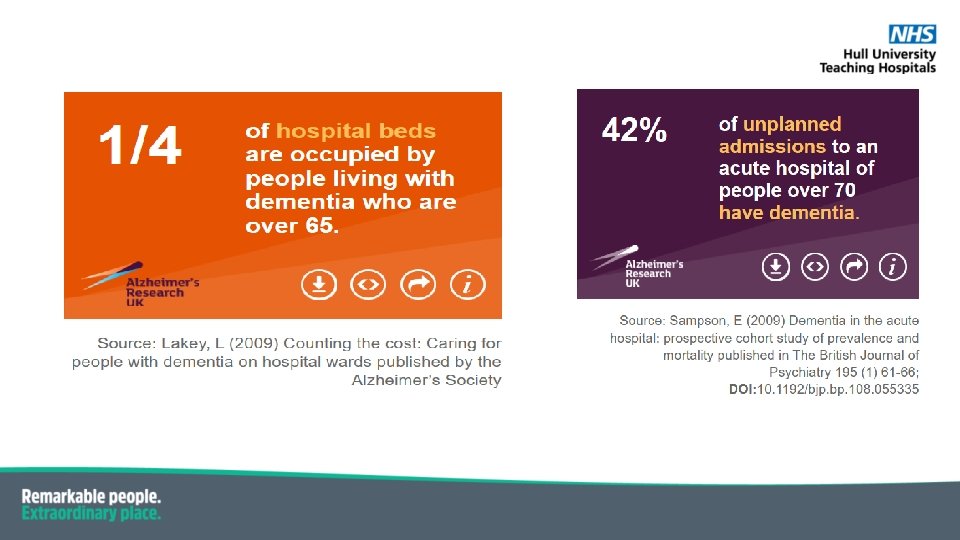
Patients with dementia : • Longer length of stay • Risk of hospital acquired harm higher • Mortality higher • Discharge process more complex • Readmission rates higher
Person centred care
Stages Of Dementia Early Moderate Severe Advanced / end stage • MMSE 21 - 24 • STM loss • Disorientation • MMSE 11 – 20 • Assistance for personal cares • MMSE < 10 • “unable to have sensible conversation” • “does not recognise family members” • Nutritional problems / swallowing problems • Prone to infections • Poor physiological reserve
Behavioural disturbance or unmet need ?
Delirium • Also termed ‘acute confusional state’ • Occurs across a range of settings • Characterised by disturbed consciousness, distractibility, perceptual abnormalities and change in cognitive function • Acute onset and fluctuating course. • Usually develops over 1– 2 days. • It is a serious condition that is associated with poor outcomes. • An estimated 30 -40% of cases preventable (Siddiqi et al, 2006)
Compared with people who do not develop delirium, people who develop delirium may: • • • need to stay longer in hospital or in critical care have an increased incidence of dementia ( 3 folds ) have more hospital-acquired complications, such as falls and pressure sores be more likely to need long term care on discharge Increased risk of readmission be more likely to die- mortality rate between 35 -40% (George et al, 1997)
• The chances of an event triggering delirium varies according to a person’s threshold • Young, fit and non cognitively impaired people – precipitant is severe • Older, frailer people with dementia – minor metabolic disturbance • Group at risk: Older people (above 65), people with dementia, severe illness or a hip fracture are more at risk of delirium. • The prevalence of delirium in people on : admission to hospital : 14 -24% during hospital admission : 6 -56% (Inouye, 1998) post operatively in surgical patients over 65 : 15 -53 % ( Inouye, 2006) ICU over 65 : 70 -87 % (Pisani et al, 2003)
Image from Hypoactive Delirium, BMJ 2017; 357: j 2047
Hypoactive delirium • Associated with poorer outcome compared to hyperactive or mixed delirium • Increased mortality and admission to longer care facility • May not come to the attention of the care provider
Why hypoactive delirium can be missed? • The nature of the condition -patient too withdrawn to alert healthcare provider -condition fluctuates and period of near normality may coincide with clinician’s assessment -establishing the diagnosis requires a degree of longitudinal overview • The nature of healthcare systems -lack of continuity of care, poor access to records, sensory impairment -delayed assessment- patient not triaged as urgent Hypoactive delirium. BMJ 2017
• Misunderstandings within the workforce -it is normal for older patients to be forgetful or disorientated -hyperactive symptoms must be present for a diagnosis to be made -patients are offended by having their cognition tested -hypoactive delirium is irreversible • Factors inherent within the population at risk -elderly patients may be socially isolated - Age UK- more than 2 million live alone -More than 1 million go for a month without speaking to family, friends or neighbours Hypoactive delirium. BMJ 2017
Delirium assessment • SQi. D • 4 AT • CAM
4 `A’s Test • Alertness • AMT 4 • Attention • Acute change or fluctuating course • Maximum score of 12 • 4 or above- possible delirium • www. the 4 AT. com
Confusion Assessment Method (CAM) • The diagnosis of delirium by CAM requires the presence of features A and B and either C or D A acute change and fluctuating course B inattention C disorganised thinking D altered consciousness
Disturbance of perception in delirium • Hallucinations, illusions and delusions up to 40% of cases • Hallucinations usually visual • Ranges from terrifying images to surreal visions
Vision and dementia • Reduced visual acuity and colour vision in patients with Alzheimer’s disease (Colour vision deficiencies in Alzheimer’s disease; Age and Ageing 2003; ) • Posterior cortical atrophy – difficulty recognising faces and objects
Pain and cognitive impairment • Often under recognised and under treated • 39% experience pain during admission (sampson 2015) • 57% able to express pain • Pain associated with slightly longer length of stay • Patients with dementia with pain – 3 times more likely to be delirious • Alzheimer’s Society -50% patients with dementia in hospital have pain Age and Ageing Journal November 2018.
Pain assessment tools
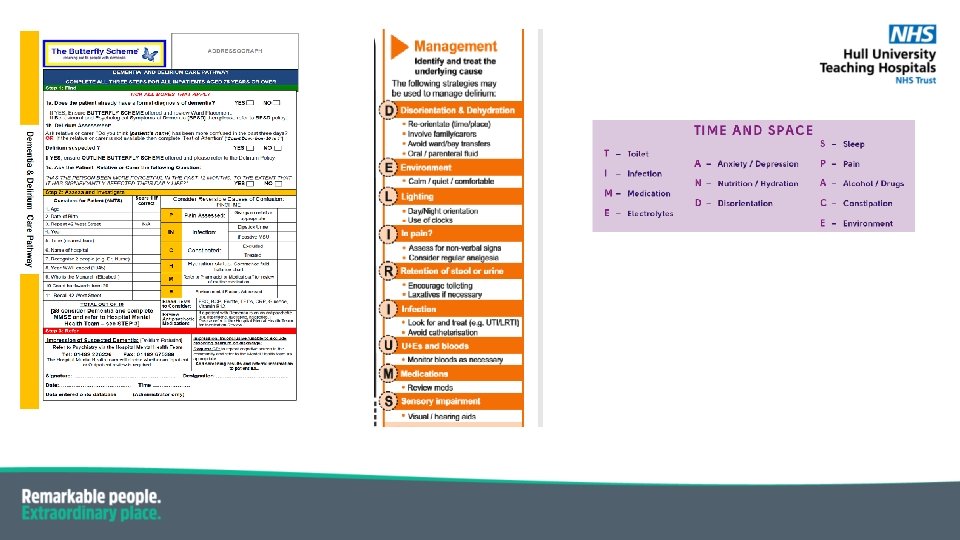
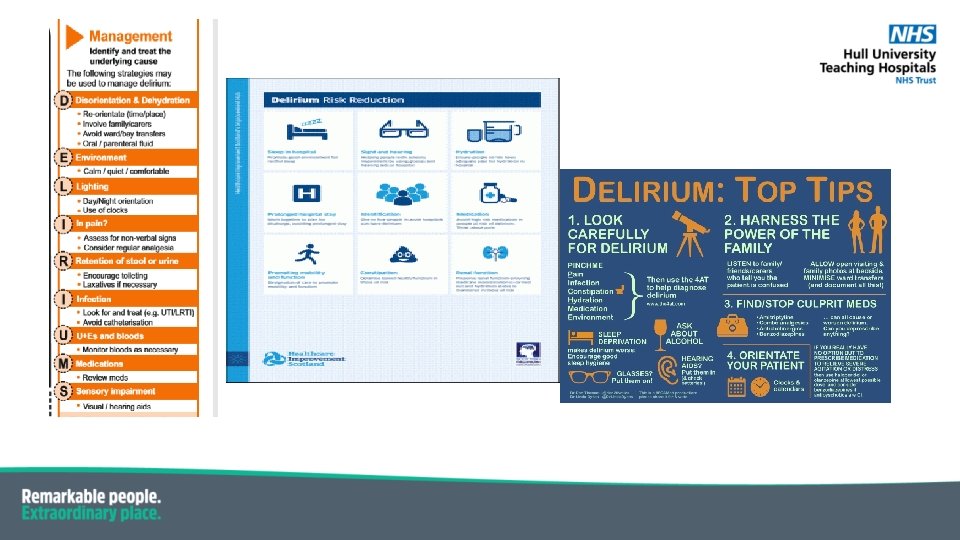
Delirium management • Apart from treating the underlying cause… 1. Patient orientation • Clocks • Calendars • Familiar objects from home • Verbal orientation on every intervention • Avoid room/ward moves • Clear signage • Good lighting
Delirium management • Communication • Bladder and bowel function -glasses, hearing aids, denture -speak clearly and calming manner -manage constipation proactively -avoid catheters • Encourage mobility • Pain -sit out for meals -toileting -monitor carefully -simple medications • Hydration and nutrition • Sleep • Support carers -assist at mealtimes -drinks readily available -information and explanation -reassurance
Pharmacological options • Usually prescribed in response to agitation/ aggression -rapid tranquilisation or treatment of delirium? • Start with lowest dose, shortest period of time • Should ideally discuss with patient/ family about potential side effects • Monitor closely and stop as soon as not needed • Haloperidol drug of choice but can try olanzapine or quetiapine • Benzodiazepines can prolong delirium
Discharge planning. . • Transfer if information from secondary care to primary care • Delirium clinic follow up