Outcomes and Factors Contributing to the Success of

Outcomes and Factors Contributing to the Success of a Community Based Patient Self-Management Diabetes Program: The Asheville Project Daniel G. Garrett, MS Senior Director, Medication Adherence APh. A Foundation dgarrett@aphanet. org

Objectives - Describe the Asheville Project and the Outcomes being achieved - Share the perceptions of patients, providers and managers on the factors contributing to success of the Asheville Project Care Model

Our Mission “The mission of the American Pharmacists Association Foundation is to improve the quality of consumer health outcomes that are affected by pharmacy. ” http: //www. APh. AFoundation. org/

Patient Centric Drug Therapy • Patient is the: – Applier – Utilizer – Determiner . . . of the outcomes associated with medication “technology” Patients on drug therapy ultimately “manage their own care”.

Original Intent of the North Carolina Pharmaceutical Care Project- 1993 • To demonstrate that community pharmacists could provide pharmaceutical care that results in positive patient outcomes • To demonstrate the value of pharmaceutical care to employers so they would pay pharmacists for “clinical” services

Original Design of the NC Pharmaceutical Care Project • Committee with representatives from all state pharmacy organizations, schools of pharmacy, industry and a PBM • Met for 3 years to come up with protocol for 3 projects (asthma, diabetes and HTN) in 3 communities, with control groups and computer software supported care ($150, 000 price tag) • ECHO model for outcomes tracking

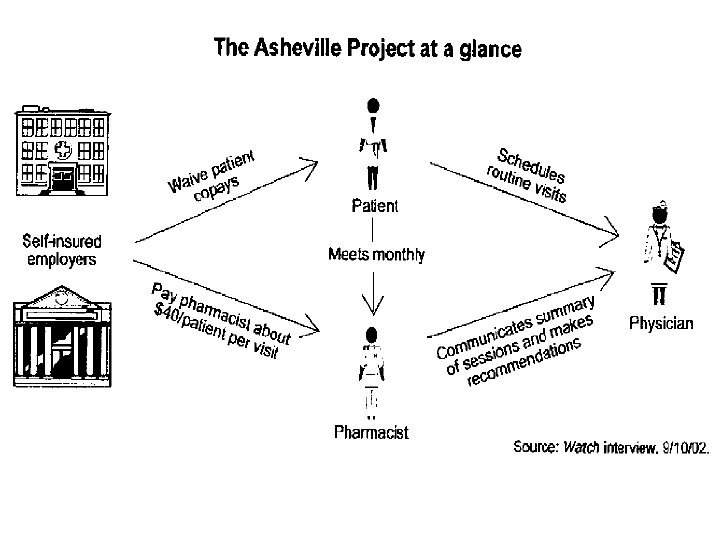
*“The Answer to How? Is When. ” • Decided in 1996 to try one project in one disease state • • • using pencil and paper The City of Asheville agreed to try for one year and see if it worked before they paid the pharmacists Diabetes was selected by the City’s Medical Consultant as the place to start The pharmacists training program was created in conjunction with the MSJ DEC with a grant of $10, 000 The City decided to waive patient co-pays and the PBM issued special rx cards The original patients were identified from a PBM report with a yellow highlighter *Peter Block, Stewardship, 1993; 234 -237

The Asheville Project

“You cannot control the system… you can only disturb it” Bennett Sims, Servanthood, Leadership for the 3 rd Millennium
 • Patient selection /")
Patient Incentives and Care Model (how we “disturbed the system”) • Patient selection / recruitment • Patient education — Mission + St. • • • Joseph’s Diabetes Center Matching patients to pharmacists Incentives – Glucose meters – PBM co-pay waivers – Labs without co-pays The operative word in pharmaceutical care is “care” (Madge Testimonial)

How They Do It “Patient making better food choice. Blood glucose much improved. 2 x 1. 5 c cm wound RLE. Referred to physician for evaluation and therapy. ”

Asheville Clinical Outcomes: Avg. Glycosylated Hemoglobin Hb. A 1 c n=136 81 55 39 26 16 Cranor et. al. JAPh. A 2003; 43(2): 175 -176. 11
: 184.")
70 70 n=50 Cranor et. al. JAPh. A 2003; 43(2): 184.
; 183.")
Asheville Enrollee Average Total Healthcare Costs Cranor, et. al. JAPh. A 2003: 43(2); 183.

Total Healthcare Costs, Combined Missions St Josephs and City of Asheville for all enrollees (unpublished data) COA & MSJ Total Healthcare Costs (avg/patient/year) prior to program for diabetes and each year of the program for 1 st 5 years $8468 $7239 $7485 $7762 $8088 20% Medical CPI Increase $2, 195, 228 Cumulative savings
 Cranor et. al. JAPh. A; 43 (2):")
City of Asheville Diabetes Sick-Leave Usage (n=37) Cranor et. al. JAPh. A; 43 (2): 180.

The Asheville Project: Participant’s Perceptions of Factors Contributing to the Success of a Patient Self. Management Diabetes Program • Focus groups of patients and diabetes care providers and individual interviews with managers involved in the project • 21 patients, 4 pharmacists, 1 CDE, 6 managers from employer groups Garrett DG, Martin, LA. J Am Pharm Assoc. 2003; 43: 185 -90

Patient Perspective • “The program saved my life” • Patients were positive about experience and enjoyed relationship with pharmacist • Reasons for joining the program: – Financial incentive – Fear of diagnosis Garrett DG and Martin LA. JAPh. A March/April ; 43(2): 187.

Employers’ Perspective • Significant resources were required to run the • • • program; however, the benefits derived far outweighed the costs of the program Employees appreciated reductions in medical costs Enhanced patient well-being and decreased absenteeism Patients sense of hope for controlling their diabetes was increased Garrett DG and Martin LA. JAPh. A March/April 2003; 43(2): 187.
 –")
Pharmacist Perspective • Participated in program because – Professional responsibility (make a difference) – Increased marketability in career • Pharmacists identified two primary factors that affected patients’ success in the program: – Whether the individual viewed his or health as a priority – The willingness of the health care professional to take time with patients Garrett DG and Martin LA. JAPh. A, March/April, 2003 43: (2) 188

Wagner et. al. Chronic Care Model • The health system is part of the larger • community and there appropriate links to health care resources in the community. Effective self-management support and links to patient-oriented community resources help to inform patients and families and motivate them to cope with the challenges of living with and treating chronic diseases. Wagner EH, Austin BT, Davis C et al. Improving chronic illness care: translating evidence into action. Health Aff 2001; 20(6): 64 -78.

Wagner et. al. Chronic Care Model • Teams of physicians and other health care providers • need to have the clinical and behavioral expertise required for productive patient interactions. Guidelines and protocols have a minimal impact unless they are implemented as part of an ongoing system of care that includes education, reminders, specialist involvement, and decision support interventions. An organized and standardized approach to collecting, summarizing, and reviewing individual and aggregate patient data is needed. Wagner EH, Austin BT, Davis C, et al. Improving chronic illness care: translating evidence into action. Health Aff 2001; 20(5): 6478.

Results from Focus Groups consistent with Wagner & colleagues Chronic Care Model • Employer interest was in improving and coordinating • • • healthcare and investing resources in a communitybased system Patients reported that the incentives and communitybased self-management support they received on an ongoing basis was essential in helping them cope with their diabetes Pharmacists and diabetes educators reported it took more than knowledge to care for patients. Key to success was the opportunity pharmacists had to work with individual patients on an ongoing basis to answer their questions and support their selfmotivated behavior changes On-going Outcomes Data collected and reported Garrett DG and Martin LA. JAPh. A 2003; 43(2): 189.

The “Asheville Program” Today • Now over 800 patients from 3 employers are • • enrolled for diabetes, asthma, hypertension and lipid therapy management Patients continue to have improved outcomes & increased medication adherence 50% reduction in sick days Zero workers comp claims in the City diabetes group over 6 years Average net savings of over $1, 600 person with diabetes each year from year 2 on

Lessons Learned that can Applied Anywhere • “Plans are nothing, planning is everything” – the foresight and comprehensive planning of “the committee” resulted in a sound process of care and collection of valuable outcomes data • CAREing makes the difference – the City paid the pharmacists before the data was in • The best way to reduce risk is to share risk – every stakeholder had an incentive to succeed

Jerry Mc. Guire “Show me the money!” “It’s all about relationships”

Question Asked in Asheville in 1996 What are you going to do if “it” works? (Will pharmacists be willing/able to meet the demand for patient care services? ) “It” works…as reported on the front page of the Washington Post, August 20, 2002.

“What Are You Going to Do if It Works? ” • Process vs. demonstration research – How do we scale this up for large employers in diverse markets? – How do we ensure consistency of care and outcomes? – How can we make this efficient? – What are the components of care required for positive outcomes?

Patient Self-Management: Diabetes Program Improving the Health of America’s Workforce and Reducing Health Care Costs Empower the Patient. Improve the Outcomes. Control the Costs. SM

PSM: Diabetes Pilot Sites Employer RPh Network Starting Date VF Corporation 4 North Carolina Sites Piedmont Pharmaceutical Care Network January 03 Mohawk Carpet Dublin, Georgia Pharmacy Association January 03 Healthcare Coalition Manitowoc, Wisconsin Pharmacist Society of Wisconsin March 03 The Ohio State University OSU Managed Care March 03 The Kroger Company Columbus, Ohio March 03 Kroger Pharmacies

“It’s a wonderful thing to have a Beautiful Mind, but more wonderful to have a Beautiful Heart” • “Integral” or “Holistic” approaches are required for “transformation” (vs. “translation”) See Ken Wilber, Marriage of Sense and Soul • At least four quadrants…biological(technical), psychological, • social and cultural are needed for chronic health management John Nash manages his health through growth and support in all quadrants, if the state of NJ had forced him to leave his home to build a bridge would this have adversely affected his health?

Can a Ripple in a Mountain Stream Start a Wave Across the Ocean?
- Slides: 33