Other databases in the United States 1 QUESTRA

Other databases in the United States 1. QUEST-RA 2. National Data Bank for the rheumatic diseases 3. RAPID Scores t. pincus@vanderbilt. edu
")
Quantitative Patient Questionnaire Monitoring in Standard Clinical Care of Patients with Rheumatoid Arthritis (QUEST-RA) • 100 RA patients from site over 2 -6 months • Patient questionnaire: 4 pages HAQ + HAQ II, MDHAQ items; MDHAQ • MD questionnaire: 3 pages SPERA Standard Protocol to Evaluate RA: clinical features, medications, 42 joint count 4 major goals: • Experience with questionnaires in standard care • Database for patient scores, DAS, work status, etc. in different sites and countries • Compare therapies atdifferent sites • Paient self-report RADAI joint count vs physician/assessor joint count
")
Quantitative Patient Questionnaire Monitoring in Standard Clinical Care of Patients with Rheumatoid Arthritis (QUEST-RA) Possible advantages over existing databases: • All RA patients over a given period – not only those taking anti-TNF, etc. • Predicition of going on to anti-TNF? • Enhance clinical rheumatology as a quantitaive science Please contact TP if interested. t. pincus@vanderbilt. edu Thank you

 § Founded 1998 § Goal: a")
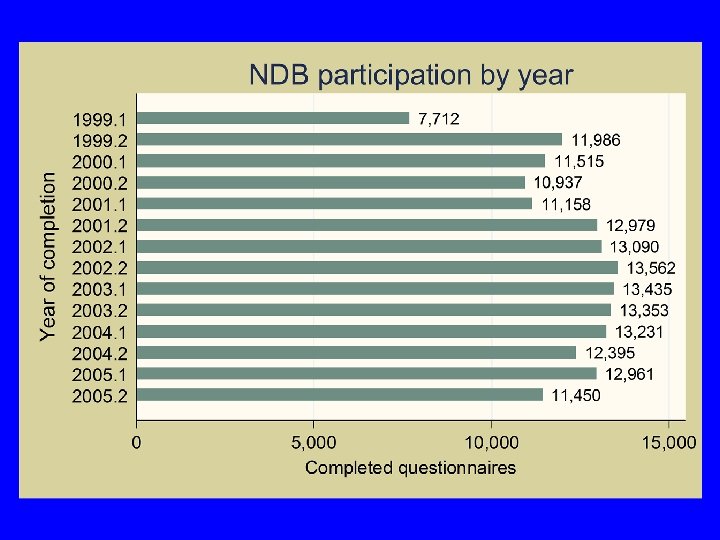
The National Data Bank for Rheumatic Diseases (NDB) § Founded 1998 § Goal: a generalizable, comprehensive, valid, reliable, believable national databank for research and teaching § Surveys at 6 month intervals § Mailed surveys, Internet, Telephone interviewing § Follow-up medical records, MD and patient contact § RA 77%, also OA, SLE, fibromyalgia, etc. § Programmers, research analysts, verifiers, QC staff, callers, records department, mortality staff, designers, administrators
")
Treatment in NDB At Last Assessment (NDB – 2005)
 § Treatments (all) § Adverse events § cardio-vascular, GI, immune")
Variables § Demographics (full) § Treatments (all) § Adverse events § cardio-vascular, GI, immune disorders, § Infection, cancer, etc § Hospitalization § Work § Costs, cost-utility § SF-36, HAQ family § Pain, fatigue, sleep, satisfaction, anxiety, depression, global, RADAI, § Utilities: Euro. Qol, HUI, Sf 6 D Euro. Qol
 §")
NDB Data Processing Hardware § T 1 -> Cisco Router § Firewall (Sonicwall) § WWW (HTTP) § VPN § E-mail § Network printers (4) § High speed scanner § Digital scanner § 4 Servers (hardware) § § § § Web Server NT 2 (E-mail) NT 1 (SQL Database) FS-ARC (On-line SQL DB for Web. Quest) Workstations (27) VPN workstations (5) Tape back-up Disk-based back-up (SQL)

The Report Project

")
NDB Privacy and Confidentiality Policy § General § Protection of participant identifying information (PII) in computer databases § Faxed questionnaires § Hard Copy questionnaires § Web-based data entry § SSL Encryption

HIPPA Compliance § As a covered entity under HIPAA, NDB has met the timelines for implementation of the initial HIPAA standards (privacy and security) that are applicable to our business. IRB approval of this implementation is available upon request. § The NDB has processes and procedures in place as they relate to the protection of data, as well as patient information.

Data Bank Questions/Projects § Costs of illness, C/E, C/U § Rates/predictors of outcomes: mortality, joint replacement, work disability, ADR § Effectiveness of therapies § Measurement of severity, development of clinical and research instruments § Psychosocial issue & predictors § Statistical techniques


Complexities in assessment of patients with rheumatic diseases: No single “gold standard” (eg, blood pressure, cholesterol) for clinical trials or standard care: therefore, indices of 3 -7 measures. 2. Laboratory tests limited in both diagnosis and treatment - primary criteria are clinical. 3. Patient questionnaires to assess physical function, pain, global status, often best quantitative measures. 1.

Indices to assess RA ACR # Tender joints # Swollen joints MD global ESR or CRP Patient function Patient pain Patient global √ √ √ √ DAS 28 SDAI √ √ √ --√ CDAI √ √ √ ---√ PAS/ RAPID ----√ √ √
 Measures Index: RAPID 2 3 4 PTJC")
RAPID (Routine Assessment of Patient Index Data) Measures Index: RAPID 2 3 4 PTJC RAPID 4 MDGL RAPID 4 MDJC RAPID 5 Physical Function √ √ √ Pain √ √ √ √ √ Patient Global Estimate √ Patient Joint Count (RADAI) √ √ MD/Assessor Joint Count MD/Assessor Global Estimate √ √
 RADAI SJC 28 TJC 28 0. 55")
RADAI vs Core Data Set measures (n=274) RADAI SJC 28 TJC 28 0. 55 --- ESR RADAI --0. 42 0. 13* Swollen 28 0. 42 --0. 23 Tender 28 0. 55 0. 32 MD Global 0. 52 0. 74 0. 57 0. 26 VAS ESR 0. 13* 0. 23 0. 32 --CRP 0. 08*** 0. 18** 0. 21 0. 50 FN MDHAQ 0. 68 0. 47 0. 52 0. 25 Pt Global 0. 69 0. 36 and center, 0. 53 All p<0. 0001, 0. 21 Adjusted for age, disease duration, education VAS except *p=0. 035, **p=0. 003, ***p>0. 05
 0 -5")
RADAI self-report Jt Count vs MD TJt. C RADAI score (0 -48) 0 -5 5 -9 10 -19 20 -48 Total MD tender joint count (0 -28) 0 -2 91 (88%) 39 (63%) 31 (48%) 12 (27%) 173 (63%) 3 -5 6 -11 12+ 8 (8%) 3 (3%) 2 (2%) 6 (10%) 3 (5%) 14 (23%) 16 (25%) 1 (2%) 39 (14%) 14 (22%) 16 (36%) 39 (14%) 3 (5%) 15 (34%) 23 (8%) Total 104 (38%) 62 (23%) 64 (23%) 44 (16%) 274

Spearman Correlation Coefficients in 274 Patients with RA – All p<0. 001 Measure CDAI RADAI 3 RAPID 4 RADAI RAPID 4 MD SJC RAPID 4 MD TJC RAPID 4 MD S&T DAS vs 0. 84 0. 66 0. 65 0. 72 0. 73 CDAI vs --0. 74 0. 75 0. 83 0. 81 0. 83

CDAI by RAPID 4 with RADAI Joint • CCC=0. 558 • Line of perfect concordance • Actual Concordance

DAS 28 Categories <2. 6 = Remission 2. 6 -3. 19 = Low DAS 3. 2 -5. 1 = Moderate DAS >5. 1 = High DAS

DAS 28 and RAPID RA Categories DAS Categories <2. 6 = Remission 2. 6 -3. 19 = Low DAS 3. 2 -5. 1 = Moderate DAS >5. 1 = High DAS Proposed RAPID Categories < 1. 0 = Near Remission 1. 01 -2 = Low Severity 2. 01 -4. 0 = Moderate Severity >4. 0 = High Severity

DAS 28 compared to RAPID 3 scores in 274 patients at 3 sites RAPID 3 Scores DAS 28 01. 0=Near remissio n 1. 1 -2. 0= 2. 1 -4. 0= 4. 1 Low Moderate 10=High Severity severity Total 02. 6=Remissio n 50 (50%) 23 (23%) 18 (18%) 10 (10%) 101 (37%) 2. 6 -3. 19=Low DAS 10 (27%) 8 (23%) 15 (41%) 4 (11%) 37 (14%) 3. 25. 1=Moderate DAS 7 (8%) 16 (18%) 26 (30%) 38 (44%) 87 (32%) >5. 1=High DAS 1 (2%) 11 (22%) 36 (73%) 49 (18%)

DAS 28 compared to RAPID 4 MDCT scores in 274 patients at 3 sites RAPID 4 MDCT Scores DAS 28 01. 0=Near remissio n 1. 1 -2. 0= 2. 1 -4. 0= 4. 1 Low Moderate 10=High Severity severity Total 02. 6=Remissio n 48 (48%) 25 (25%) 22 (22%) 6 (6%) 101 (37%) 2. 6 -3. 19=Low DAS 10 (27%) 9 (24%) 15 (41%) 3 (8%) 37 (14%) 3. 25. 1=Moderate DAS 7 (8%) 15 (17%) 34 (39%) 31 (36%) 87 (32%) >5. 1=High DAS 0 (0%) 2 (4%) 9 (18%) 38 (78%) 49 (18%)

CDAI compared to RAPID 3 scores in 274 patients at 3 sites RAPID 3 Scores CDAI 01. 0=Near remissio n 1. 1 -2. 0= 2. 1 -4. 0= 4. 1 -10= Low Moderate High Severity severity 03. 3=Remissio n 39 (70%) 13 (23%) 4 (7%) 0 (0%) 56 (20%) 3. 4 -11. 0=Low activity 23 (25%) 24 (26%) 31 (33%) 15 (16%) 93 (34%) 11. 1 -26. 0= Moderate activity 5 (5%) 11 (12%) 29 (31%) 50 (53%) 95 (35%) >26=High activity 1 (3%) 0 (0%) 6 (20%) 23 (77%) 30 (11%) Total

Saving time and improving care with a multidimensional health assessment questionnaire: 10 practical considerations T Pincus, Y Yazici, M Bergman J Rheumatol 33: 448 -454, 2006

Question for Rheumatologists For patients with RA under your care (not including patients in clinical trials), how often do you performal tender and swollen joint counts? Never 13% 1– 24% of visits 25– 49% of visits 50– 74% of visits 75– 99% of visits Always 32% 11% 14% 16% 14% Pincus and Segurado Ann Rheum Dis 2006

MDHAQ Page 1

35

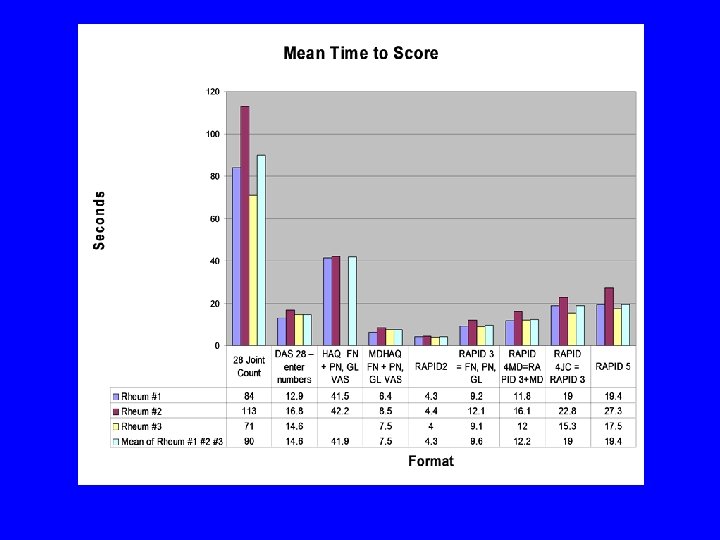
Median number of seconds to score various RA measures

Methods • A cross-sectional database of 100 consecutive patients with RA was established at 3 sites: New York –Yazici, Philadelphia – Bergman, Nashville –Pincus. • The rheumatologists completed a 28 joint count. • Patients completed an expanded health assessment questionnaire (HAQ), including a self-report RADAI joint count.

Indices to assess RA ACR DAS 28 SDAI CDAI # Tender joints √ √ # Swollen joints √ √ MD global √ - √ √ ESR or CRP √ √ √ -- Patient function √ -- -- -- Patient pain √ -- -- -- Patient global √ √

Indices to assess RA + RAPID= Routine Assessment of Patient Index Data # Tender joints √ √ PAS/ RAPID -- # Swollen joints √ √ -- MD global √ - √ √ -- ESR or CRP √ √ √ -- -- Patient function √ -- -- -- √ Patient pain √ -- -- -- √ Patient global √ √ √ ACR DAS 28 SDAI CDAI
 Measures Index: RAPID 3 RAPID 4 PT")
RAPID (Routine Assessment of Patient Index Data) Measures Index: RAPID 3 RAPID 4 PT JC RAPID 4 MD JC Physical Function √ √ √ Pain √ √ √ Patient Global Estimate √ √ √ Patient Joint Count (RADAI) MD/Assessor Joint Count MD/Assessor Global Estimate √ √

DAS 28 and proposed RAPID Categories DAS 28 Categories <2. 6 = Remission 2. 6 -3. 19 = Low DAS 3. 2 -5. 1 = Moderate DAS >5. 1 = High DAS Proposed RAPID Categories < 1. 0 = Near Remission 1. 01 -2 = Low Severity 2. 01 -4. 0 = Moderate Severity >4. 0 = High Severity

DAS 28 compared to RAPID 4 MDS&T scores in 274 patients at 3 sites RAPID 4 MDS&T Scores DAS 28 01. 0=Near remissio n 1. 1 -2. 0= 2. 1 -4. 0= 4. 1 Low Moderate 10=High Severity severity Total 02. 6=Remissio n 53 (52%) 28 (28%) 17 (17%) 3 (3%) 101 (37%) 2. 6 -3. 19=Low DAS 10 (27%) 13 (35%) 1 (3%) 37 (14%) 3. 25. 1=Moderate DAS 6 (7%) 18 (21%) 41 (47%) 22 (25%) 87 (32%) >5. 1=High DAS 0 (0%) 2 (4%) 11 (22%) 36 (73%) 49 (18%)

DAS 28 compared to RAPID 3 scores in 274 patients at 3 sites RAPID 3 Scores DAS 28 01. 0=Near remissio n 1. 1 -2. 0= 2. 1 -4. 0= 4. 1 Low Moderate 10=High Severity severity Total 02. 6=Remissio n 50 (50%) 23 (23%) 18 (18%) 10 (10%) 101 (37%) 2. 6 -3. 19=Low DAS 10 (27%) 8 (23%) 15 (41%) 4 (11%) 37 (14%) 3. 25. 1=Moderate DAS 7 (8%) 16 (18%) 26 (30%) 38 (44%) 87 (32%) >5. 1=High DAS 1 (2%) 11 (22%) 36 (73%) 49 (18%)

CDAI compared to RAPID 4 MDS&T scores in 274 patients at 3 sites RAPID 4 MDS&T Scores CDAI 01. 0=Near remissio n 1. 1 -2. 0= 2. 1 -4. 0= 4. 1 -10= Low Moderate High Severity severity 03. 3=Remissio n 43 (77%) 12 (21%) 1 (2%) 0 (0%) 56 (20%) 3. 4 -11. 0=Low activity 23 (25%) 36 (39%) 31 (33%) 3 (3%) 93 (34%) 11. 1 -26. 0= Moderate activity 3 (3%) 12 (13%) 45 (47%) 35 (37%) 95 (35%) >26=High activity 0 (0%) 1 (3%) 5 (17%) 24 (80%) 30 (11%) Total

CDAI compared to RAPID 3 scores in 274 patients at 3 sites RAPID 3 Scores CDAI 01. 0=Near remissio n 1. 1 -2. 0= 2. 1 -4. 0= 4. 1 -10= Low Moderate High Severity severity 03. 3=Remissio n 39 (70%) 13 (23%) 4 (7%) 0 (0%) 56 (20%) 3. 4 -11. 0=Low activity 23 (25%) 24 (26%) 31 (33%) 15 (16%) 93 (34%) 11. 1 -26. 0= Moderate activity 5 (5%) 11 (12%) 29 (31%) 50 (53%) 95 (35%) >26=High activity 1 (3%) 0 (0%) 6 (20%) 23 (77%) 30 (11%) Total

RAPID 4 RADAI compared to RAPID 4 MDS&T scores in 274 patients at 3 sites RAPID 4 MDS&T Scores RAPID 4 RADAI 0 -1. 0=Near remission 01. 0=Near remissio n 1. 1 -2. 0= 2. 1 -4. 0= 4. 1 -10= Low Moderate High Severity severity Total 64 (96%) 3 (5%) 0 (0%) 67 (24%) 1. 1 -2. 0=Low severity 5 (9%) 46 (84%) 4 (7%) 0 (0%) 55 (20%) 2. 1 -4. 0= Moderate severity 0 (0%) 12 (16%) 61 (84%) 0 (0%) 73 (27%) 4. 1 -10=High severity 0 (0%) 17 (22%) 62 (78%) 79 (29%) 69 (25%) 61 (22%) 82 (30%) 62 (23%) 274 Total

RAPID 3 compared to RAPID 4 RADAI scores in 274 patients at 3 sites RAPID 4 RADAI Scores RAPID 3 01. 0=Near remissio n 0 -1. 0=Near remission 65 (96%) 3 (4%) 0 (0%) 68 (25%) 1. 1 -2. 0=Low severity 2 (4%) 43 (90%) 3 (6%) 0 (0%) 48 (18%) 2. 1 -4. 0= Moderate severity 0 (0%) 9 (13%) 57 (81%) 4 (6%) 70 (26%) 4. 1 -10=High severity 0 (0%) 13 (15%) 75 (85%) 88 (32%) 67 (24%) 55 (20%) 73 (27%) 79 (29%) 274 Total 1. 1 -2. 0= 2. 1 -4. 0= 4. 1 -10= Low Moderate High Severity severity Total

RAPID 3 compared to RAPID 4 MDS&T scores in 274 patients at 3 sites RAPID 4 MDS&T Scores RAPID 3 01. 0=Near remissio n 0 -1. 0=Near remission 65 (96%) 3 (4%) 0 (0%) 68 (25%) 1. 1 -2. 0=Low severity 4 (8%) 43 (90%) 1 (2%) 0 (0%) 48 (18%) 2. 1 -4. 0= Moderate severity 0 (0%) 15 (21%) 54 (77%) 1 (1%) 70 (26%) 4. 1 -10=High severity 0 (0%) 27 (31%) 61 (69%) 88 (32%) 69 (25%) 61 (22%) 82 (30%) 62 (23%) 274 Total 1. 1 -2. 0= 2. 1 -4. 0= 4. 1 -10= Low Moderate High Severity severity Total

Criteria for clinical measure • Clinical trials - – Validity – does it measure what is supposed to be measured? – Reliability – is it reproducible? • Clinical care – also consider – Feasibility – can it be performed? – Acceptability – will clinicians assess it?

Patient questionnaires for clinical research and improved standard patient care: is it better to have 80% of the information in 100% of patients or 100% of the information in 5% of patients? T Pincus, F Wolfe J Rheumatol 32: 575 -577, 2005.

Conclusions • A self-report RADAI joint count is confirmed to give information similar to a tender joint count performed by an assessor. • Self-report joint counts might be considered as a routine procedure for standard care of patients with rheumatic diseases. • A self-report RADAI joint count might be included in clinical trial protocols to assess longitudinal performance to distinguish between active and control treatements.

Conclusions • We hope to collaborate with 30 rheumatologists to perform comparisons of self-report joint counts and MD/assessor joint counts in 100 RA patients in their clinical care. • If interested, please contact: t. pincus@vanderbilt. edu

Continuous quality improvement based on MDHAQ indices 1. MDHAQ for feasibility 2. Easy scoring 3. Flowsheets–lab and drugs 4. Index or indices 5. Categories of severity 6. Continuous quality improvement for treatment decisions


Patients seen for standard rheumatoid arthritis care have significantly better articular, radiographic, laboratory, and functional status in 2000 than in 1985 T Pincus, T Sokka, H Kautiainen Arthritis Rheum 52: 1009 -1019, 2005

Cross-Sectional Data in Patients With RA: Cohort #2 in 1985 and Cohort #4 in 2000: Swollen Joint Count Scores 1985 2000 20 Swollen Joint Count 28 20 16 12 8 4 0 0 5 10 15 Disease Duration (Years) 20 0 5 10 15 Disease Duration (Years) Pincus, Sokka, Kautiainen, Arth Rheum 52: 1009, 2005 20

Cross-Sectional Data in RA Patients: Cohort #2 - 1985 and Cohort #4 -2000: Larsen X-Ray score, % of maximum 1985 2000 RFRF+ RF 5 positive 0 0 Pincus, Sokka, Kautiainen, Arth Rheum 52: 1009, 2005 RF-

Cross-Sectional Data in Patients With RA: Cohort #2 in 1985 and Cohort #4 in 2000: Multidimensional Health Assessment Questionnaire (MDHAQ) scores 2000 2. 0 1. 5 MHAQ 1985 1. 0 0. 5 0. 0 0 5 10 15 Disease Duration (Years) 20 0 5 10 15 20 Disease Duration (Years) Pincus, Sokka, Kautiainen, Arth Rheum 52: 1009, 2005

The treatment of rheumatoid arthritis: getting better all the time? RF van Vollenhoven, L Klareskog Arthritis Rheumatism 52: 991 -994, 2005

Six-year report of the STURE registry for biologicals in rheumatology: satisfactory overall results, but plenty of room of improvement RF van Vollenhoven, C Cullinane, J Bratt, L Klareskog Arthritis Rheumatism 52: S 135, 2005

Are patient questionnaires more “scientific” than lab test and x-rays in RA? Physical function scores on the HAQ or MDHAQ, not a joint count, lab test or X-ray, is far and away the most significant predictor in RA of functional status, work disability, costs, joint replacement surgery, and death l A physician may treat fever without a temperature, tachycardia without a pulse, diabetic coma without a glucose, but why l Treating RA with primary attention to laboratory tests and radiographs without a physical function score may be analogous to treating hypertension according to heart sounds or renal failure according to a urinalysis – it’s relevant but a not the most effective prognostic marker l

Focus on function – a modern patient centered approach in rheumatology - - Rheumatology measures for clinical research versus standard care Why focus on patient-reported outcome (PRO) measures? Routine Assessment of Patient Index Data (RAPID) scores on an MDHAQ to quantify RA severity without formal joint counts Remodeling the biomedical model to include a biopsychosocial model

Is it better to have 80% of the information in 100% of patients or 100% of the information in 5% of patients? T Pincus, F Wolfe J Rheumatol 32: 575 -577, 2005.

Some limitations of patient self-report questionnaires 1. Need for translation –language issues 2. Cultural and linguistic issues 3. Possibility of “gaming” by patient, health professional to provide desired responses 4. Not specific to any disease

Focus on function – a modern patient centered approach in rheumatology - - Rheumatology measures for clinical research versus standard care Why focus on patient-reported outcome (PRO) measures? Routine Assessment of Patient Index Data (RAPID) scores on an MDHAQ to quantify RA severity without formal joint counts Remodeling the biomedical model to include a biopsychosocial model

The need for a new medical model: a challenge for biomedicine “Medicine’s unrest derives from a growing awareness among many physicians of the contradiction between the excellence of their biomedical background on the one hand the weakness of their qualifications in certain attributes essential for good patient care on the other. ” - George L. Engel Science 196: 134, 1977

Some Assumptions of a Biomedical Model · Reductionism – single cause, single cure for each disease · Mind-body dualism – “mental” vs “somatic" as separate entities · Diagnosis based mostly on “tests” · High tech lab, X-ray data superior to patient data to assess & predict · Outcomes depend more on MDs, drugs, than on patients

Editorial: Challenges to the biomedical model: are actions of patients almost always as important as actions of health professionals in long-term outcomes of chronic diseases? T Pincus Advances in Mind-Body Medicine 16: 276 -294, 2000
")
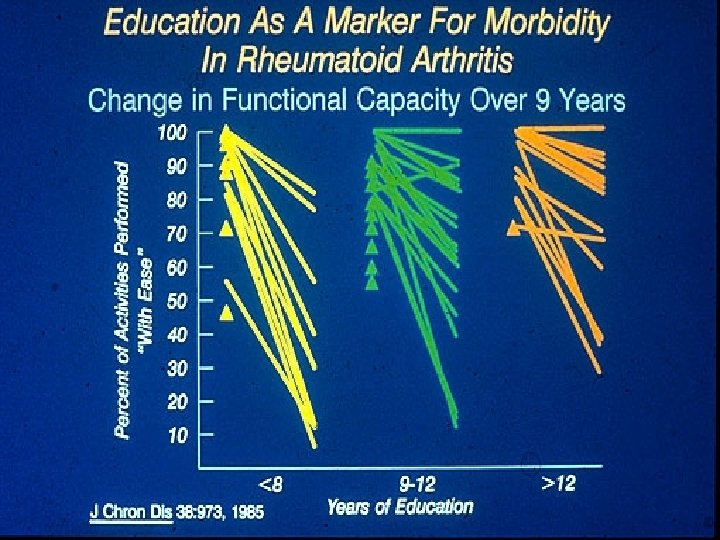
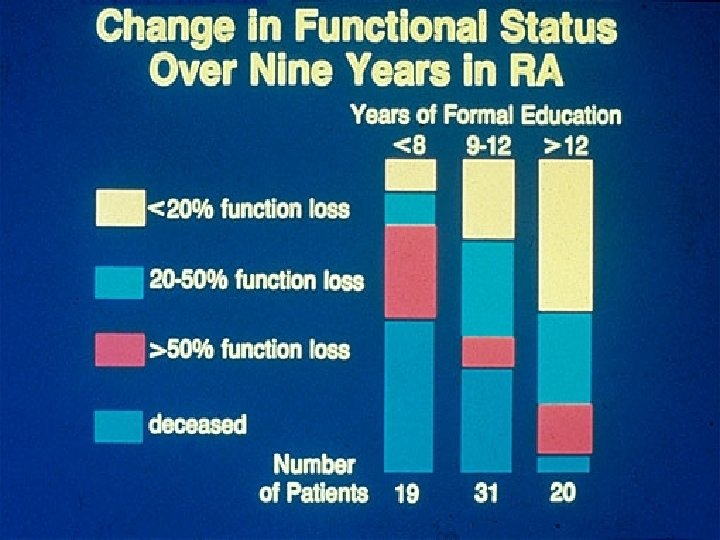
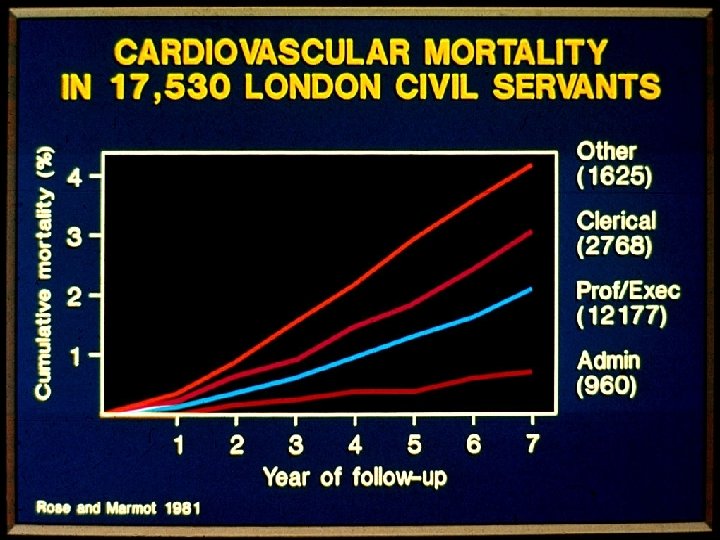
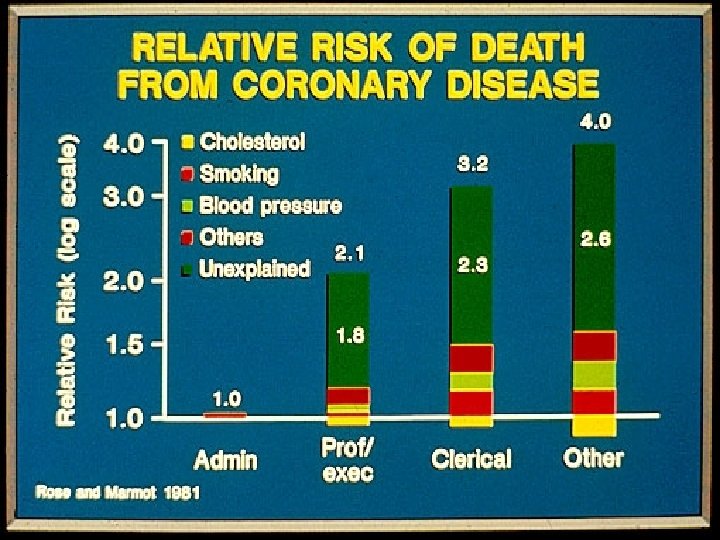
9 -10 Year Survival According to Quantitative Markers in Three Chronic Diseases Survival (%) 100 >90% 81– 90% 80 % Active “With Ease” 60 40 71– 80% 20 (Data from Pincus et al, 1987) Survival (%) C 0 20 40 60 80 100 Stage III All Stages, All Causes Stage IV 60 40 20 2 4 6 8 10 Years >12 Years 9– 12 Years 60 £ 8 Years 40 20 (Data from Pincus et al, 1987) 0 D 20 40 60 80 100 Months Coronary Artery Disease # of Involved Vessels 100 80 60 40 20 (Data from Kaplan, 1972) 0 80 Months Stage I 80 Formal Education Level 100 £ 70% Hodgkin’s Disease Anatomic Stage 100 B Survival (%) A Rheumatoid Arthritis - Survival (%) Rheumatoid Arthritis Activities of Daily Living 1 Artery 2 Arteries 3 Arteries LCA (Data from Proudfit et al, 1978) 0 2 4 6 8 10 Years

Survival in rheumatoid arthritis 1973 -1982 Pincus et al. Arthritis Rheum. 1984; 27: 864. J Rheumatol 1987; 14: 240

Severe functional declines, work disability, and increased mortality in seventy-five rheumatoid arthritis patients studied over nine years T Pincus, LF Callahan, WG Sale, AL Brooks, LE Payne, WK Vaughn Arthritis Rheum 27: 864 -872, 1984

Rheumatoid Arthritis over 9 years – changes in functional status in activities of daily living and morning stiffness 1973 -1982 Activities of daily living 1973 100 1982 Morning Stiffness 1973 0 90 30 80 60 70 90 60 120 50 150 40 180 30 210 20 240 10 270 0 300 % No Difficulty 1982 Minutes Pincus et al. Arthritis Rheum. 1984; 27: 864; J Rheumatol. 1992; 19: 1051

Taking mortality in rheumatoid arthritis seriously – predictive markers, socioeconomic status and comorbidity T Pincus , LF Callahan J Rheumatology 13: 841 -845 1986
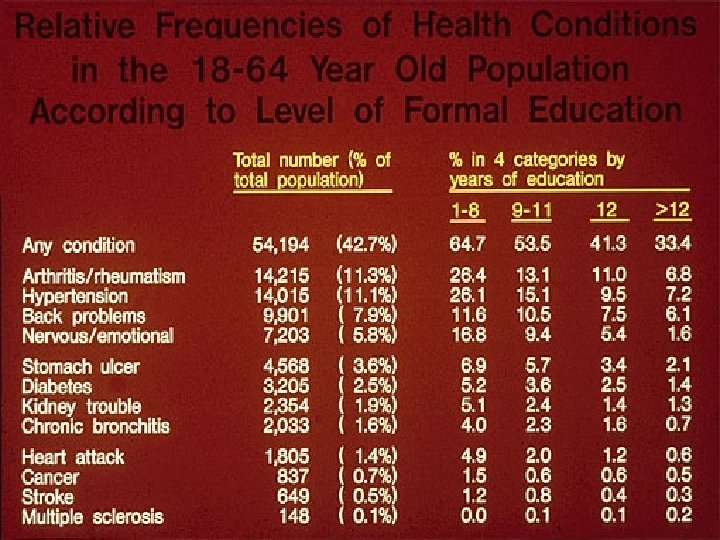
 and health – Possible explanations Limited education Possible solutions More")
Formal education (socioeconomic status) and health – Possible explanations Limited education Possible solutions More education Limited Resources Money, Medicaid Limited access to “health care” Psychosocioeconomic problems Increase access to medical services Change how “system” works

U. S. Expenditures as a Percentage of GDP, 1962 -1998

“A Biopsychosocial Model” GL Engel, Science 196: 129, 1977 • “Non -reductionism” or “wholism” - multiple causes, approaches to “control” vs “cure”treat whole patient - not just “broken part” • Mind-body connections in all aspects of care • Patient data more “scientific” than lab, X-ray • Outcomes depend as much on patients as on professionals • Medical care system limited to improve health Does this model provide an extraordinary opportunity for leadership by rheumatologists, rather than trying to fit a “biomedical model” ?

Do We Need Two Complementary Models? • Bio-medical model in acute diseases, and in acute events within chronic diseases for short term care • Bio-psychosocial model in chronic diseases, to address long term patient care needs and outcomes

Rudolph Virchow • “Omnis cellula ex cellula • Founder of cellular pathology • Named: • leukocyte, • leukemia, • pulmonary embolism, • amyloid, • trichinosis

“The improvement of medicine would eventually prolong human life, but improvement of social conditions could achieve this result now more rapidly and more successfully. ” Rudolf Virchow 1848

“Medicine is a social science, and politics nothing else but medicine on a large scale. ” “The physicians are the natural attorneys of the poor, and the social problems should largely be solved by them. ” Rudolf Virchow, 1848

The Sickness Unto Death A Christian Psychological Exposition for Upbuilding and Awakening Soren Kierkegaard, 1849 This concept, the sickness unto death, must, however, be understood in a particular way… we use the expression “fatal sickness” as synonymous with the sickness unto death.

The Varieties of Religious Experience William James, 1902, “The Sick Soul” “antagonism may naturally arise between the healthy-minded way of viewing life and the way that takes all this experience of evil as something essential. . . Evil is a disease; and worry over disease is itself an additional form of disease…to the healthy-minded way, on the other hand, the way of the sick soul seems diseased. ”
 The indigent sick of this city and its environs, without")
Johns Hopkins (1795 -1873) The indigent sick of this city and its environs, without regard to sex, age or color, who may require surgical or medical treatment, and the poor of this city and State, of all races, who are stricken down by any casualty, shall be received into the Hospital, without charge, for such periods of time and under such regulations as you may prescribe. Letter to the first Trustees of the Johns Hopkins Hospital, March

Focus on function – a modern patient centered approach in rheumatology - - Measures in clinical rheumatology Why focus on patient-reported outcome (PRO) measures? A continuous quality improvement strategy using patient questionnaires in the infrastructure of patient care Remodeling the biomedical model to include a biopsychosocial model

“The proper study of mankind is man…. ” Alexander Pope, 1733

“The proper study of mankind is man…. ” Alexander Pope, 1733 …. and woman Theodore Pincus, 2006 t. pincus@vanderbilt. edu

Thank you for your attention and interest! Tack so mycket


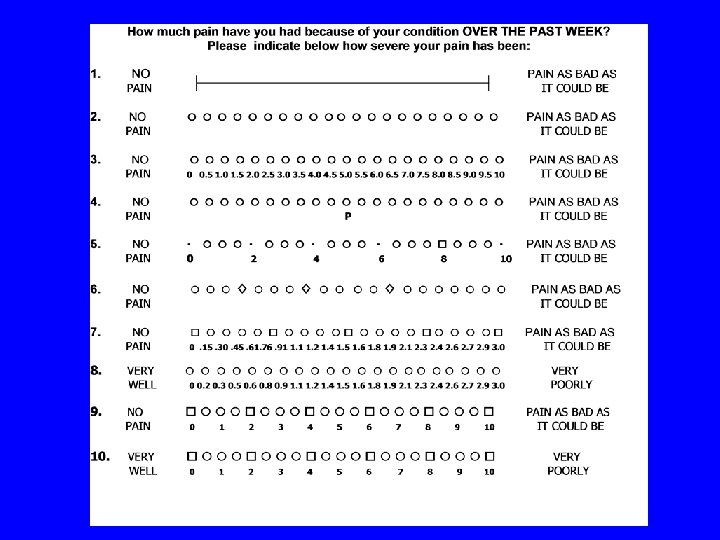
Multidimensional Health Assessment Questionnaire AT THIS MOMENT, are you able to: Dress yourself, including tying shoelaces and doing buttons? Get in and out of bed? Lift a full cup or glass to your mouth? Walk outdoors on flat ground? Wash and dry your entire body? Bend down to pick up clothing from the floor? Turn regular faucets on and off? Get in and out of a car, bus, train or airplane? Walk 2 miles or 3 kilometers? Participate in sports and games as you would like? Get a good night’s sleep? Deal with feelings of anxiety or being nervous? Deal with feelings of depression or feeling blue? Without ANY Difficulty -------------------- With SOME Difficulty With MUCH Difficult UNABLE To Do ---------------------------------------- How much pain have you had because of your condition IN THE PAST WEEK? Place a mark on the line below to indicate how severe your pain has been: NO PAIN 0 0. 5 1. 0 1. 5 2. 0 2. 5 3. 0 3. 5 4. 0 4. 5 5. 0 5. 5 6. 0 6. 5 7. 0 7. 5 8. 0 8. 5 9. 0 9. 5 10 Considering all the ways in which your illness and health conditions may affect you at this time, place a mark to show you are doing: VERY WELL 0 0. 5 1. 0 1. 5 2. 0 2. 5 3. 0 3. 5 4. 0 4. 5 5. 0 5. 5 6. 0 6. 5 7. 0 7. 5 8. 0 8. 5 9. 0 9. 5 10 PAIN AS BAD AS IT COULD BE VERY POORLY
")
A Multinational Cross-Sectional Database To Assess Clinical Status Of Patients With Rheumatoid Arthritis (QUESTRA) Sokka, Mäkinen, Hetland, Verstappen, Toloza, Herborn, Naranjo, Gossoc, Bresnihan, Cazzato, Baecklund, Sierakowski, Tunc, Skakic, Pincus for the Quest-RA Group

An international effort: • To enroll 100 consecutive patients with RA • >10 countries • >3 sites/country • to establish a collaborative cross sectional study of RA

Primary Objective • To provide experience with measurement tools that can be used in routine clinical care, to improve patient care

Methods of data collection • 100 consecutive patients with RA in each clinic to complete 4 -page a patient questionnaire • The patients to be assessed according to a standard protocol to evaluate RA: – a review of clinical features – comorbidities – all disease-modifying antirheumatic drugs (DMARDs) used – joint count
 with •")
• The patients completed an expanded self-report health assessment questionnaire (HAQ) with • visual analog scales (VAS) for pain, global status, and fatigue • a self-report joint count on RADAI • life-style choices such as smoking and physical exercise • work status

• Data collection started in January 2005

Study status 14 -August-2006 # sites # patients in the database Denmark 3 301 Finland 3 304 France 4 389 Germany 3 226 Ireland 3 225 Italy 4 336 Netherlands 3 317 Poland 7 638 Spain 3 301 Sweden 3 244 UK 3 114 Turkey 3 300 Serbia 1 100 USA 3 295 Argentina 2 246 Total = 15 48 4336 Country

New Quest-RA Countries collecting data: Estonia Greece Hungary Latvia Lithuania Macedonia

New countries interested; ACR 2006 • Russia • Australia • Canada • Latin America
 or percentage Age, current, years 57. 0")
Patients; Demographic variables Demographic Variables Mean (SD) or percentage Age, current, years 57. 0 (13. 8) Age at 1 st symptoms, years 45. 4 (15. 0) Female Education, years 78. 0% 10. 6 (3. 9) Caucasian 88. 0% Currently working full time 20. 7%
 or per ce nta ge")
Patients; Disease characteristics Disease Mean Characteris (S tics D) or per ce nta ge Disease 11. 5 duration, (10. years 0) from 1 st symptoms fibrosis/pericarditis/Felty/vasculitis/scleritis *nodules/pulm

Patients; Clinical measures Swollen Joint count 28 Tender Joint count 28 DAS 28 0 -10 MD global VAS 0 -10 Questionnaire measures HAQ 0 -3 Pain VAS 0 -10 Morning stiffness, minutes Laboratory ESR Mean (SD) 4. 2 (5. 4) 6. 0 (7. 2) 4. 1 (1. 7) 2. 8 (2. 4) 1. 0 (0. 8) 4. 1 (2. 7) 51. 3 (69. 2) 27. 7 (23. 4)

Comparison of clinical measures in Western Europe vs. Other Countries N SJC 28 TJC 28 MDGlobal VAS ESR DAS 28 HAQ PAIN VAS Fatigue VAS Morning stiffness W. Europe and USA 2964 3. 3 4. 4 Other Countries 1194 6. 5 9. 9 2. 3 24. 2 3. 7 0. 9 3. 7 4. 0 45. 4 4. 0 36. 0 5. 1 1. 3 5. 0 5. 1 64. 9 Mean values shown; Student’s t-test p<0. 001 for all comparisons

The first DMARD in 1970’s to 2000’s in Europe; The raise of methotrexate IM Gold MTX SSZ Traditional DMARDs HCQ

Next slide will show • Selected DMARDs ever used by >4000 RA patients from the 15 countires • In each column • yellow indicates the highest • blue the lowest percentage among the countries

DMARD ever: Pred MTX HCQ SSZ LEF Any Biol Denmark 43% 86% 39% 64% 11% 23% Finland 74% 85% 74% 84% 21% 17% France 83% 87% 55% 49% 42% 53% Germany 54% 80% 36% 25% 29% Ireland 71% 92% 15% 33% 24% 41% Italy 69% 78% 42% 14% 31% 26% Netherlands 26% 81% 28% 35% 6% 19% Poland 69% 79% 34% 60% 18% 8% Spain 67% 85% 43% 29% 34% 27% Sweden 66% 81% 34% 62% 9% 31% UK 51% 75% 39% 46% 4% 16% Turkey 69% 81% 27% 61% 22% 7% Serbia 88% 69% 55% 17% 7% 2% USA 77% 85% 49% 12% 19% 33% Argentina 83% 68% 49% 6% 16% 3% Total; n=4157 66% 81% 43% 21% 23%

DMARDs: Discussion • Large differences are seen in the use of biologics and other DMARDs among countries. • Reasons for this observation may include: – patients who participated in RCTs were not excluded – local and national traditions to use DMARDs – differences in national guidelines to use/limit biologics – genetic/behavioral factors of patient populations – marketing

DOES POOR FUNCTIONAL CAPACITY PREVENT PATIENTS WITH RHEUMATOD ARTHRITIS FROM PHYSICAL EXERCISES?
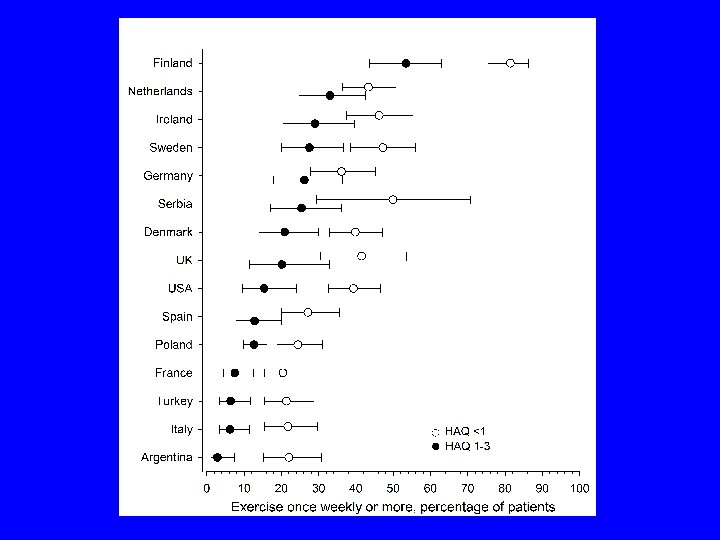

Physical Exercises: Discussion • A low proportion of RA patients exercise in many countries. • However, poor functional status does not necessarily prevent RA patients from physical exercises. • Importance of regular physical exercises should be emphasized in RA patients – rather than neglected or even forbidden - its effects on fitness, metabolic status, and longevity need more attention in patients with RA. • These data may serve as a basis for health educators to improve patterns of exercise habits in patients with RA in different countries.

Clinical status of RA in relation to macro economic variables in 15 countries Next slide: Relationship between Gross Domestic Product (GDP), expressed as parity purchasing power, and the overall clinical status on the Mean Outcome Index for Rheumatoid Arthritis (MOIRA) in 15 QUEST-RA countries. The area of the disc reflects the amount of the total national health expenditure (TNEH) per capita in each country.
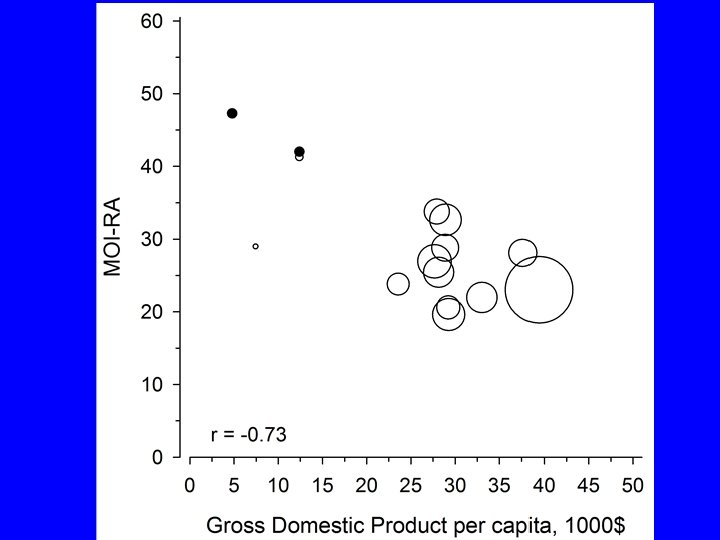

Discussion; macro economic variables and RA disease activity • Macro-economic variables that characterize a nation are important predictors of health outcomes. • Gross domestic product (GDP) is a predictor of overall mortality, infant mortality, and life expectancy. • Concerning outcomes of specific diseases, a 5 -years survival of cancer was associated with GDP in an analysis of data from 22 European countries. • Macro-economic variables appear important also concerning RA clinical disease activity.

Conclusions • This international multi-center cross sectional database will provide a general overview of clinical status and treatments of patients with RA in standard clinical care in 2005 -06 although data may not be representative for all included countries due to few sites. • The QUEST-RA program should further enhance introduction of quantitative assessment into standard care of patients with rheumatic diseases, including those who are not treated with biological agents and not included in databases that involve patient selection.

Thanks to the Quest-RA Group: • • • • • Denmark : K Hørslev-Petersen, M Hetland, TM Hansen; Finland: H Makinen, K Immonen, S Forsberg, J Lähteenmäki, R Luukkainen; France: M Dougados, L Gossec, JF Maillefert, B Combe, J Sibilia; Germany: R Rau, G Herborn, R Alten, C Pohl, G Burmester; Ireland: B Bresnihan, P Minnock, E Murphy, C Sheehy, J Devlin, S Alraqi; Italy: M Cutolo, M Cazzato, GF Ferraccioli, F Salaffi, A Stancati; The Netherlands: S Verstappen, M Huisman, M Hoekstra; Poland: S Sierakowski, S Sadkiewicz, M Majdan, D Zarowny-Wierzbinska, W Romanowski, D Kapolka, W Tlustochowicz; Spain: M Belmonte, J Calvo-Alen, A Naranjo; Sweden: E Baecklund, AC Holmqvist, R Oding; UK: P Taylor, C Mc. Clinton, K Dolan, E Choy, S Kelly, A Woolf, G Chorghade; Turkey: F Gogus, S Celik, R Tunc; Serbia: V Skakic, A Dimic, J Nedovic, A Stankovic; USA: T Pincus, M Bergman, Y Yazici; Argentina: S Toloza Abbott DATABASE SPECIALIST: Christopher Swearingen DATA ENTRY: Melissa Gibson, Gina Sung, Kalevi Koskinen, Joni Saalamo Ted Pincus

An index of the three core data set patient questionnaire measures distinguishes efficacy of active treatment from the of placebo as effectively as the American College of Rheumatology 20% response criteria (ACR 20) or the disease activity score (DAS) in a rheumatoid arthritis clinical trial. T Pincus, V Strand, G Koch, I Amara, B Crawford, F Wolfe, S Cohen, D Felson Arthritis Rheum 48: 625 -630, 2003

A proposed continuous quality improvement program to improve care of patients with RA without formal joint counts based on MDHAQ indices 1. MDHAQ for feasibility 2. Easy scoring 3. Flow sheets–lab and drugs 4. Index or indices 5. Categories of severity 6. Continuous quality improvement for treatment decisions

Focus on function – a modern patient centered approach in rheumatology - Rheumatology measures for clinical research versus standard care Why focus on patient-reported outcome (PRO) measures? A RAPID index for RA severity based on MDHAQ, without joint counts Remodeling the biomedical model to include a biopsychosocial model

Median number of seconds to score various RA measures

Continuous quality improvement based on MDHAQ indices 1. MDHAQ for feasibility 2. Easy scoring 3. Flowsheets–lab and drugs 4. Index or indices 5. Categories of severity 6. Continuous quality improvement for treatment decisions

Types of measures to assess rheumatoid arthritis: Joint count a. Swelling, tenderness or pain on motion b. Limited motion or deformity 2. Radiographs scores 1. a. Erosion b. Joint space narrowing 3. Laboratory tests 1. a. Erythrocyte Sedimentation Rate (ESR) 2. b. C-Reactive Protein (CRP) 1. 4. Patient questionnaire a. Physical function b. Pain c. Psychological distress d. Fatigue 5. Global measures
 score based on the MDHAQ indices 1.")
A Routine Assessment of Patient Data (RAPID) score based on the MDHAQ indices 1. MDHAQ for feasibility 2. Easy scoring 3. Flowsheets–lab and drugs 4. Index or indices 5. Categories of severity 6. Continuous quality improvement for treatment decisions

MDHAQ Page 1

Continuous quality improvement based on MDHAQ indices 1. MDHAQ for feasibility 2. Easy scoring 3. Flowsheets–lab and drugs 4. Index or indices 5. Categories of severity 6. Continuous quality improvement for treatment decisions

Median number of seconds to… Perform 28 joint count 90 Enter DAS at web site 14. 6 Score standard HAQ Score MDHAQ Score RAPID 2 Score RAPID 3 Score RAPID 4 MDGL Score RAPID 4 PTJC Score RAPID 5 41. 9 7. 5 4. 3 9. 6 12. 2 19. 0 19. 4

Continuous quality improvement based on MDHAQ indices 1. MDHAQ for feasibility 2. Easy scoring 3. Flowsheets–lab and drugs 4. Index or indices 5. Categories of severity 6. Continuous quality improvement for treatment decisions

Patient Self-Report Questionnaire Scores in the Assessment of RA 1. Significant correlation with joint counts, ESR, X-ray scores, physical measures 2. More reproducible than traditional joint counts, ESR, X-ray scores 3. As informative as the ACR-20, -50, -70, or DAS in clinical trials 4. Predicts work disability, costs, joint replacement, and premature death better than traditional joint counts, radiographs, and DAS = Disease Activity Score. tests laboratory

m. HAQ: Correlation With Various Measures of Clinical Status in 259 Patients With RA Variable* Correlation Coefficient Joint count score 0. 60 Radiographic score 0. 31 ESR 0. 24 Grip strength – 0. 53 Walk time 0. 44 ARA class 0. 60 Patient global 0. 74 Age 0. 23 Duration of disease 0. 28 Formal education level – 0. 24 *P < 0. 001 for all variables versus mean scores for 8 activities of daily living on the m. HAQ. ARA = American Rheumatism Association; m. HAQ = Modified Health Assessment Questionnaire. Pincus T, et al. Ann Intern Med. 1989; 110: 259– 266.

Patient Self-Report Questionnaire Scores in the Assessment of RA 1. Significant correlation with joint counts, ESR, X-ray scores, physical measures 2. More reproducible than traditional joint counts, X-ray scores, ESR 3. As informative as the ACR-20, -50, -70, or DAS in clinical trials 4. Predicts work disability, costs, joint replacement and premature death better than traditional joint counts, radiographs, and laboratory tests

Patient Self-Report Questionnaire Scores in the Assessment of RA 1. Significant correlation with joint counts, ESR, X-ray scores, physical measures 2. More reproducible than traditional joint counts, ESR, X-ray scores 3. As informative as the ACR-20, -50, -70, or DAS in clinical trials 4. Predicts work disability, costs, joint replacement and premature death better than traditional joint counts, radiographs, and laboratory tests

Patient Self-Report Questionnaire Scores in the Assessment of RA 1. Significant correlation with joint counts, ESR, X-ray scores, physical measures 2. More reproducible and less likely to improve with placebo than traditional joint counts, ESR, X-ray scores, physical measures 3. As informative as the ACR-20, -50, -70, or DAS in clinical trials 4. Predicts work disability, costs, joint replacement and premature death better than traditional joint counts, radiographs, and

Attributed Causes of Death in 2, 262 RA Patients in 13 Series from Diverse Locales Compared to General Population Attributed Cause of Death % of RA Deaths Cardiovascular disease 42. 1 41. 0 Cancer 14. 1 20. 4 Infection 9. 4 1. 0 Renal disease 7. 8 1. 1 Pulmonary disease 7. 2 3. 9 RA 5. 3 --GI disease 4. 2 2. 4 CNS disease 4. 2 9. 6 Accidents 1. 0 5. 4 Miscellaneous 6. 4 15. 2 Unknown 0. 6 --- % of 1977 US Pincus T, Callahan LF. J Rheumatol. 1986; 13: 841.
: 115 -26.")
Atherosclerosis--an inflammatory disease R Ross N Engl J Med 1999; 340(2): 115 -26.

Quantitative Monitoring of RA Over 720 Days: MHAQ, Pain 10 Visual Analog 5 Pain Scale 0 2 MHAQ 1 Difficulty Score 0 Salsalate Zero Order Aspirin Fenoprofen Piroxicam Methotrexate Auranofin Injectable Gold Prednisone 9/87 1/88 5/88 Pincus T. Arthritis Care Res. 1996; 9: 339. 9/88 1/89 5/89 8/89

Quantitative Monitoring of a Patient With SLE over 180 days: ESR, anti-DNA, CH 50 Creat Clear (m. L/min) LE Prep CH 50 100 140 50 90 0 40 - + + - - 200 100 % DNA 50 Bound 100 0 Prednison e (mg/day) ESR (mm/hr ) 0 50 0 20 40 60 80 100 120 140 160 180 Days Pincus, Schur, Rose, Talal, Decker. New Engl J Med. 1969; 281: 701.
 0 -5")
RADAI self-report Jt Count vs MD TJt. C RADAI score (0 -48) 0 -5 5 -9 10 -19 20 -48 Total MD tender joint count (0 -28) 0 -2 91 (88%) 39 (63%) 31 (48%) 12 (27%) 173 (63%) 3 -5 6 -11 12+ 8 (8%) 3 (3%) 2 (2%) 6 (10%) 3 (5%) 14 (23%) 16 (25%) 1 (2%) 39 (14%) 14 (22%) 16 (36%) 39 (14%) 3 (5%) 15 (34%) 23 (8%) Total 104 (38%) 62 (23%) 64 (23%) 44 (16%) 274

Criteria for clinical measure • Clinical trials - – Validity – does it measure what is supposed to be measured? – Reliability – is it reproducible? • Clinical care – also consider – Feasibility – can it be performed? – Acceptability – will clinicians assess it?

5 -Year Survival in 206 Patients With RA: Cohort #2 – 19851990 Rheumatoid Factor MHAQ Score 80 80 Survival (%) 100 60 Absent (29) Present (175) 40 20 0 0 12 24 36 48 Months After Baseline Arthritis Care Res 10: 381, 1997 60 60 0. 00 (12) 0. 01– 0. 99 (91) 1. 00– 1. 99 (86) >2. 00 (21) 40 20 0 0 12 24 36 48 Months After Baseline 60

A HAQ or MDHAQ Patient Questionnaire not a Lab test or X-ray – is Best Predictor in RA of… n Functional status (Pincus et al. Arthritis Rheum. 1984, Wolfe et al. J Rheumatol. 1991) n Work disability (Borg et al. J Rheumatol 1991, Callahan et al. J Clin Epidemiol. 1992, Wolfe and Hawley. J Rheumatol. 1998, Fex et al. J Rheumatol 1998, Sokka et al. J Rheumatol 1999, Barrett et al. Rheumatology 2000, ) n Costs (Lubeck et al. Arthritis Rheum. 1986) n Joint replacement surgery (Wolfe and Zwillich. Arthritis Rheum. 1998) n Death (Pincus et al. Arthritis Rheum. 1984, Ann Intern Med. 1994, Wolfe et al. J Rheumatol 1988, Leigh&Fries J Rheumatol 1991, Wolfe et al. Arthritis Rheum. 1994, Callahan et al. Arthrits Care Res 1996, 1997, Soderlin et al. J Rheumatol 1998, Maiden et al. Ann Rheum Dis 1999, Sokka et al. Ann Rheum Dis 2004)

Fax Server § Accepts faxed forms electronically § 8 Fax lines capability § Converts faxes to electronic Teleform data § Verified, validated and converted to SQL by same method as paper forms
 Fax")
Rheumatic Disease Data Banking § Data Collection Methods § § § Scanning (Teleform) Fax Server Web entry Interactive PDF Telephone interview with patient Telephone contact with physicians (rare)
- Slides: 150