OSTEOPOROSIS Prof Dr lk Akarrmak Metabolic Bone Diseases

OSTEOPOROSIS Prof. Dr. Ülkü Akarırmak

Metabolic Bone Diseases n Osteosclerosis n Osteolysis n Osteoporosis bone disease is the most common metabolic

Vertebral Body Normal Osteoporotic

Definition of Osteoporosis A systemic skeletal disease - characterized by low bone mass - microarchitectural deterioration of bone tissue - with a consequent increase in bone fragility and susceptibility to fracture

Osteoporosis 1. Low bone mass and 2. Reduced bone quality Result: Increased risk of fracture


Bone structure n Cortical and trabecular bone n Bone cells Bone function

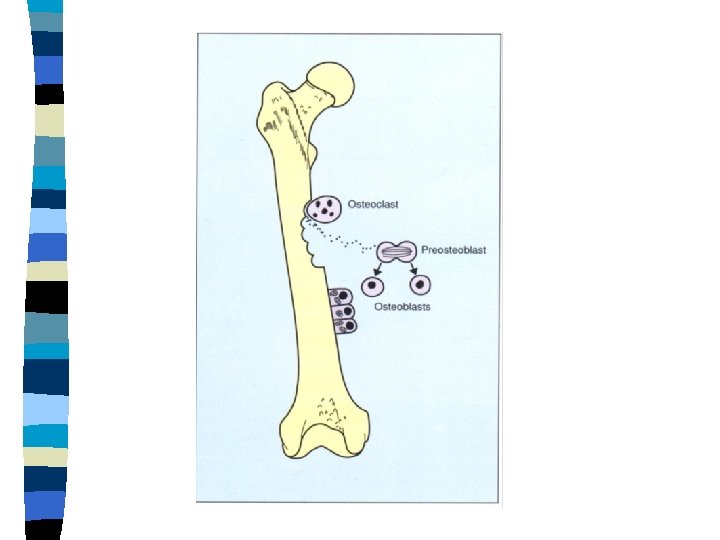
Bone Turnover - Osteoclasts - Bone resorption - Osteoblasts - Bone formation - Osteocytes Formation=Resorption

Bone Turnover Osteoclasts Osteoblasts Monocytes Osteocytes

Bone Metabolism

Bone Metabolism Local factors: Growth factors 3 Systemic hormones: - Parathormone - Vitamin D - Calcitonin 3 Involved systems: - Bone - Intestines - Renal

Peak Bone Mass Genetic factors 70% Nutrition PBM Exercises Hormones

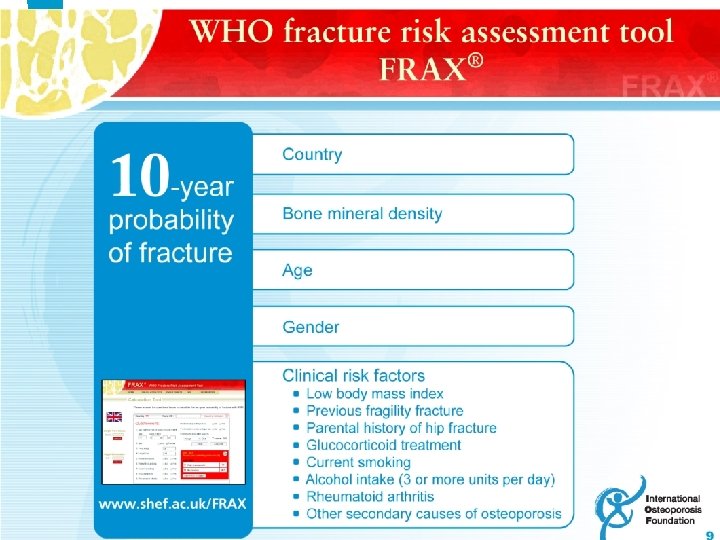
Risk Factors for Fracture n Age n Female sex n Family fx n Previous fx n Glucocorticoids

Risk Factors for Osteoporosis Modifiable n Inadequate exercise n Inadequate nutrition - calcium - vitamin D - balanced diet n Medications - glucocorticoids - excess thyroid - etc. n Smoking n Excessive alcohol intake

Risk Factors for Osteoporosis 2 Nonmodifiable Genetics n Gender n Race n Age n

Classification I. Primary OP 1 - Postmenopausal 2 - Senile II. Secondary OP

Sec. OP

Osteoporosis n Fractures: Mortality – Morbidity n Pain n Deformity n Loss of quality of life

Clinical Picture The traditional picture of an individual with osteoporosis: An elderly woman with a curved back and stooped posture, a woman who has lost height and who appears small and frail

Major Osteoporotic Fractures Type Colles Vertebral Hip Typical age 55 65 75 Female: male ratio 4: 1 3: 1 2: 1

Femur fx Peripheral fx Forearm fx

Spinal Osteoporotic Fractures n Acute – chronic pain n Kyphosis n Nontraumatic - low energy fx

Progressive loss of height; Development of kyphosis


Spinal Fx

Pathogenesis of Osteoporotic Fracture LOW PEAK BONE MASS POSTMENOPAUSAL BONE LOSS Low Bone Mass Nonskeletal factors AGE-RELATED BONE LOSS Other risk factors FRACTURE Increased risk of falls Poor bone quality

Hip Fx

Femoral Fractures n Mortality in 20% of patients over 60 years of age n Morbidity in 50%

Clinical Results of Osteoporotic Fractures n Pain n Reduction in physical activity n Deformity n Muscle weakness n Social isolation n Loss of independence n Increased mortality

Evaluation of Osteoporosis n Identify risk factors for OP n Identify contributing factors Medical history: Secondary OP n Physical examination n DXA n X-ray n Laboratory Evaluation

Radiographic Evaluation n n n 0 Normal 1 End plate deformity 2 Fish vertebrae 3 End plate fracture 4 Wedge vertebrae 5 Compression fracture

X-Ray of Thoracic Spine

Diagnosis of Osteoporosis n Osteodensitometry DXA = Dual X- ray Absorptiometry Bone Mineral Density BMD

Indications for Bone Densitometry n n n Female patients > 65 years Patients with osteoporosis risk factors Vertebral abnormalities and/or osteopenia on x-rays Long – term glucocorticoid therapy Primary hyperparathyroidism or other diseases with high risk of OP Patients being treated for OP, to monitor changes in bone mass
 BMD T-score Normal 0 - (-1)SD Osteopenia (-1) -")
Diagnosis Based on BMD (WHO) BMD T-score Normal 0 - (-1)SD Osteopenia (-1) - (-2. 5)SD Osteoporosis <(-2. 5)SD Established OP ‘’ + fracture

Recommendations Based on BMD Normal Osteopenia OP Establ OP Risk of Fx Very low Low High<(-2. 5)SD Very high Action Prevention Treatment

Osteodensitometry is the most important method for diagnosis Fracture risk may be assessed n Low BMD is associated with increased fracture risk n

ROI

Laboratory Tests - Routine Biochemistry Serum calcium Phosphorus Alkaline phosphatase Creatinine Total protein, albumin, and globulin 25(OH)Vitamin D - Complete blood count - Sedimantation rate - Biochemical markers of bone turnover

Differential Diagnosis Metastasis Multiple Myeloma Osteoporotic Fx

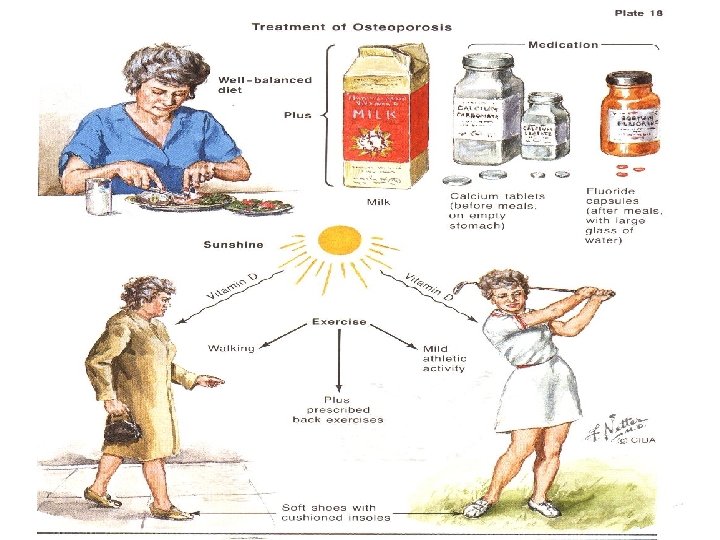
Osteoporosis is a…. n Preventable n Treatable disease Recommendations n 1. Nutrition 2. Activity 3. Vitamin D n

Approaches for Management of Osteoporosis: Pharmac&Nonpharmacologic n Prevent fractures - Medical therapy - Prevention of falls n Improve physical function n Improve quality of life

Therapeutic Agents Used in Osteoporosis Osteoclast Inhibition of Resorption Osteoblast Stimulation of Formation

Inhibitors of Bone Resorption n n n n Calcium HT: Estrogens +/- progestogens SERMs Bisphonates Alendronate Zoledronate Risedronate Ibandronate Calcitonin

Stimulators of Bone Formation n Parathyroid hormone injections

Dual Action n Strontium n Vitamin ranelate D and active derivatives n Ipriflavon n Anabolic steroids

Calcium – Vitamin D Calcium - Adults : 1000 mg Increased: Over 65 years, after menopause, pregnancy, stilling Vitamin D : Adults : 400 -800 IU Over 70 years: >800 IU

HRT: Estrogen n Reduces the rate of bone loss n Reduces fracture risk in postmenopausal women Adverse effects; WHI Limited time

Calcitonin n Reduces bone loss in postmenopausal women- bone quality n Effective on spinal fractures n Opt. dose: 200 IU/daily nasal spray n High tolerability

Bisphonates: Gold Standard Indication: PMO Male OP GIO Decrease fracture incidence ALN: 70 mg/w ZOL: 5 mg. IV/yearly infusion RIS: 35 mg/w-75/mo IBN: 150 mg/mo - 3 mg 3 mo inf Contraindication: Oesaphageal irritation

Strategies for Reducing Falls and Fractures - Maintain physical activity - Provide a safe home environment - Balance training - Ambulatory support when appropriate - Avoid sedative medications - Minimize other contributing medical problems - Hip pads in the frail elderly

Hip Pads n Prevention of hip fractures in patients with high fracture risk - shock absorbing effect

Decrease Risk of Falls

Questions n Comments
- Slides: 57