OSTEOMYELITIS DR SHAILESH DEFINITION Osteomyelitis is an inflammation



Endogenous (Haematogenous) b)Exogenous • Based on host")





 • I. V.")

 E. coli, Proteus, Klebsiella, Haemophilus influenza-infants Salmonella, brucella,")














 1. An appropriate antibiotic will be effective before pus formation.")























 • This is seen when newly formed reactive bone")




 Gentamycin PMMA Beads")


")


 • This was described by Garre")
")











 B. Suis and B. melitensis.")












or • 2 -hydroxystilbamidine(8 -12 gm), IV is effective. b)Actinomycosis/Madura")














. - CT, MRI and")
. •")







- Slides: 114
OSTEOMYELITIS . DR SHAILESH
DEFINITION • Osteomyelitis is an inflammation of the bone caused by an infecting organism Osteon-bone Myelo-marrow • The infection mainly involves marrow spaces, haversian canals, and subperiosteal space. • Bone is involved secondarily.
CLASSIFICATION • Based on duration of symptoms: Acute Sub acute Chronic Active Dormant
CLASSIFICATION • Based on mode of spread: a)Endogenous (Haematogenous) b)Exogenous • Based on host response: a)Specific b)Non-specific
ACUTE OSTEOMYELITIS
• It is a rapidly destructive pyogenic infection, usually haematogenous in origin, starting in metaphysis of an actively growing long bone • Seen in infants and children
• It may occur in adults also due to spread of infection directly from another site or through compound fractures. • Haematogenous spread is rare
ETIOLOGY • Disease is common during the period of active bone growth (below 2 years and 8 -12 years). • Sex - Male : Female - 4: 1 • Site -Metaphysis, mainly in children (60 -70% around knee).
RISK FACTORS • Poor nutrition and unhygienic surrounding. • Trauma (more in men and boys). • Skin, dental, respiratory, GI, UT infections. • Bacterial endocarditis. • Burns
RISK FACTORS • Leukopoenia and leukocyte dysfunction. • Iatrogenic intervention (catheters) • I. V. drug abuse • Sickle cell anaemia • Haemodialysis/immune suppressive therapy
BACTERIOLOGY Gram positive Staph. aureus 60 -90% Streptococcus –multiple lesions Streptococcus epidermis, Enterococci, Clostridium, Bacillus, Diphteroids, Listeria.
BACTERIOLOGY Gram negative Pseudomonas (greenish discharge) E. coli, Proteus, Klebsiella, Haemophilus influenza-infants Salmonella, brucella, niesseria, bacterioids.
BACTERIOLOGY Specific type • • Tuberculosis M. leprae, Spirochetes-T. pallidum Actinomycosis, Candida, Cryptococcosis, Coccidiodo mycosis • Viral-small pox • Parasitic
BACTERIOLOGY Infant <1 yr 1 -16 yrs >16 yrs Group B Streptococci Staph. aureus E. coli S. aureus S. pyogenes H. influenza S. aureus S. epidermidis Gram –ve bacilli
BACTERIOLOGY eu s C N Ps S eu M R do SA ae St rug re in o p vi sa r St ida re ns p G St p B ap h ep i Eco li 50 45 40 35 30 25 20 15 10 5 0 St ap h au r Percent IDLinks Speakers Club 15
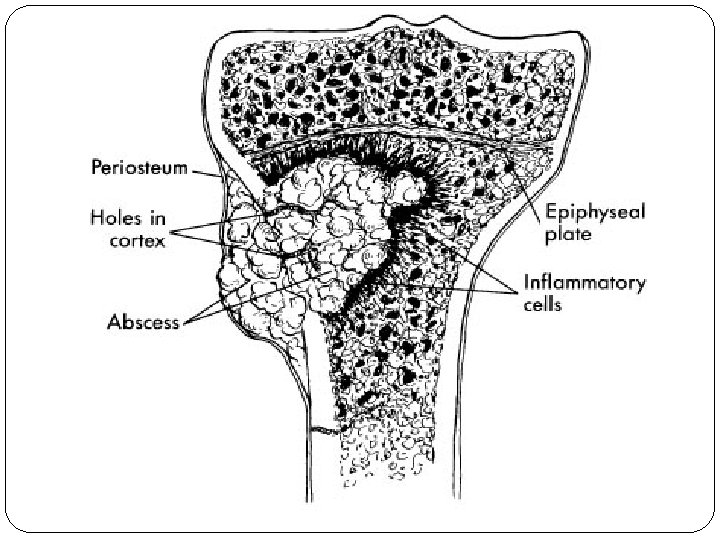
PATHOGENESIS Infective Emboli Blocks Nutrient Artery Necrosis of small part of bone
PATHOGENESIS Hyperemia Serum & Polymorphs Exudate & Debris
PATHOGENESIS ↑Pressure in compartment Follows least path of resistance Accumulate in subperiosteal spaces Ruptures & Forms abscess & along fascial planes
WHY METAPHYSEAL OM COMMON ?
• Hair pin bend vessels in metaphysis • As there is increased vascularity to metaphysis causing pooling of blood, it has been aptly called ‘a lake of blood’. • Immature cells of metaphysis due to high cell turnover.
• Relative lack of phagocytosis. • Presence of degenerating cartilage cells which acts as a good culture media. • Presence of end arteries in metaphysis. • More prone for trauma. • Presence of a single endothelial lining in metaphyseal arteries.
CLINICAL FEATURES • Antecedent infection is usually present /history of trauma. • Symptoms of Acute illness appears like irritability, restlessness, headache, vomiting, convulsions, chills, febrile with increase PR.
CLINICAL FEATURES • Pain • Initially no swelling is present but within few days, "the soft tissues becomes oedematous • Limb will be in a position of ease with restricted movements and surrounding muscle spasms.
CLINICAL FEATURES • Sympathetic synovitis of adjacent joints may be present. • If patient is not treated, he becomes apathetic and unconscious and continues fatal termination.
INVESTIGATION ØBlood investigation ØAspiration of pus & blood culture ØX-ray ØBone scan ØMRI
DIFFERENTIAL DIAGNOSIS • Rheumatic fever • Ewing’s tumor • Acute suppurative arthritis
PRINCIPLES OF TREATMENT NADE(1983) 1. An appropriate antibiotic will be effective before pus formation. 2. Antibiotics will not sterilize avascular tissues and purulent material that must be removed surgically.
3. If such removal is effective, then antibiotics should prevent their reformation and therefore primary wound closure should be safe. 4. Surgery should not further damage already ischaemic bone and soft tissues. 5. Antibiotics should be continued after surgery.
CONSERVATIVE TREATMENT Ø The affected part should be positioned comfortably at rest. Ø General supportive measures. Ø If subperiosteal and bone aspiration do not show any abscess, IV antibiotics are started.
SURGICAL TREATMENT Indications for Surgery • Presence of an abscess requiring drainage. • Failure of patient to improve despite appropriate IV antibiotic treatment. Objective of surgery is to drain any abscess cavity and remove all dead and necrotic materials.
AFTER TREATMENT • Part should be protected for several weeks to prevent pathological fracture. • IV antibiotics should be continued post operatively for a short course followed by oral antibiotics.
COMPLICATIONS Early ü Septic arthritis ü Tenosynovitis ü Thrombophlebitis ü Death from associated septicaemia
COMPLICATIONS Late ü Pathological fracture ü Local growth disturbances : Over growth - due to prolonged hyperaemia. ü Premature cessation - Due to epiphyseal plate destruction. ü Deformity due to epiphyseal plate destruction.
PROGNOSIS • About 90% of cases diagnosed early and treated energetically may be expected to resolve completely. Ø The organism Ø The bone infected ØThe age of the patient
SUBACUTE HEMATOGENOUS OM
• Differs from acute OM in the severity of symptoms and signs. This may be due to • Increased host resistance • Low bacterial virulence • Antibiotic therapy before symptoms occur.
CLASSIFICATION • Type-I : Metaphyseal lesion • Type-II : Eccentric metaphyseal lesion with cortical erosion • Type-III : Diaphyseal cortical lesion
CLASSIFICATION Type-IV : Lesion is a medullary abscess in diaphysis with periosteal reaction Type-V : Primary sub acute epiphyseal OM. Type-VI : Subacute OM crossing epiphyseal plate to involve both metaphysis and epiphysis.
CLASSIFICATION
CLINICAL FEATURES • • Pain without constitutional symptoms. ESR elevated in 50% of cases. Blood culture negative. Pus C/S positive in 60% patients.
DIAGNOSIS • On clinical suspicion and radiographic imaging. • Bacteriology : Staph, aureus and epidermidis common
TREATMENT • Typical lesions - Antibiotics for 6 weeks. • Diagnosis in doubt – Biopsy and curettage of lesion and antibiotics.
CHRONIC OSTEOMYELITIS
When acute OM was untreated/ inadequately treated or due to haematogenous spread of low virulence or infection through external wound.
CLASSIFICATION Cierny and Mader classification - based on anatomic and physiologic criteria. Anatomic Criteria: Intramedullary Superficial Local Diffuse with segmental bone loss.
CLASSIFICATION Physiologic Criteria: Ø Normal immune system and adequate soft tissue envelope. Ø Local /systemic /both compromised patients. Ø When the results of treatment are potentially more damaging than the presenting condition
PATHOLOGY SEQUESTRUM INVOLUCRUM CLOACA
SEQUESTRUM It is a microscopic or macroscopic fragment of necrotic, usually, cortical bone found at the nidus of the infection within the bone. MERCER
TYPES • Tubular sequestrum-Pyogenic infection<2 years • Feathery-Pyogenic infection. • Coarse Sandy Sequestrum-In tuberculosis. • Dense ivory- In syphilis • Coloured sequestrum (Black)-In ulna and tibia OM. • Ring Sequestrum- Pin tract infection and amputation stump infection. • Bombay Sequestrum -Calcaneal OM. • Corolliform-Pyogenic infections.
INVOLUCRUM • Derived from-volvere(to wrap) • This is seen when newly formed reactive bone occurs at the interface between diseased bone and healthy tissue • Multiple openings in the involucrum -CLOACA
CLINICAL FEATURES • During acute exacerbation • Aching pain, • Overlyingsoft tissues become oedematous, warm, reddened and tender. • Patient will be febrile. • As infection progresses, a sinus may open and drain, extruding small sequestra at intervals.
ROENTGENOGRAPHIC FINDINGS Ø Early stages - Moth-eaten appearance. Ø Elevation of periosteum with subperiosteal laminations of new bones. Ø Sharply delineated areas of dense bone with surrounding decalcification. Ø Gradually, necrotic dense area is surrounded by white ring of involucrum. Ø Shaft becomes enlarged and mishapen.
TREATMENT • The goal of surgery is eradication of infection by achieving a viable and vascular environment which may require radical debridement. • Inadequate debridement may be the cause for high recurrence rate.
• • • Sequestrectomy and Curettage Open bone grafting(Papineau technique) Gentamycin PMMA Beads Closed Suction Drains Soft Tissue Transfer
• • • Ilizarov Technique Hyberbaric Oxygen Therapy Belfast Technique Silver Iontophoresis Amputation-infrequently performed
Sequestrectomy and Curettage
(Papineau technique)
COMPLICATIONS Ø Growth disturbances Ø Pathological fracture Ø Muscle contracture Ø Secondary septicaemia Ø Epithelioma Ø Joint stiffness Ø Amyloidosis.
MISCELLANEOUS CONDITION
1. Scelrosing OM of Garre (Idiopathic cortical sclerosis) • This was described by Garre in 1891. • Infants and children are more frequently affected. • The long bones particularly tibia and femur are usually affected. • It is subacute or chronic. • Cause is unknown but it is thought to be an infection caused by low grade anaerobic bacteria
CLINICAL FEATURES • Pain, dull aching in nature, worse at night. • Swelling (Fusiform) and deep tenderness present on the affected bone. • Overlying soft tissues are normal
Investigation: ESR increased, culture negative. Radiology: shows symmetrical thicknening of cortex with some narrowing of medulla and also shows sclerosis.
Biopsy: shows chronic low grade non specific OM. Treatment: Fenestration of sclerotic bone and antibiotics
2. Brodies Abscess • It is a localized form of subacute OM caused by organsims of low virulence. • Occurs in young adults, more often in the long bones of lower extremities
• Most commonly in metaphysis before epiphyseal closure. • In the adults metaphyseal epiphyseal area is involved.
Clinical Features: • Intermittent pain of long duration • O/E local tenderness on the affected area X-ray: shows an osteolytic area with a ring of dense sclerosis.
• Staphylococcus aureus is cultured in 50% of the patient and 20% are negative cultures. • Diagnosis often requires biopsy. • Treatment curettage of lesion with administration of antibiotics. Wound is closed over drains.
SPECIFIC TYPES
Tuberculosis • Is chronic specific granulomatous inflammation by acid fast bacilli-Mycobacterium tuberculosis of bovine or human type. • Usually secondary to primary elsewhere • Affects any age with metaphysis in children and diaphysis in adults.
PATHOLOGY Trauma with hematoma Tubercle bacilli from circulation Settles & proliferates Acute & chronic inflammatory response Tubercle follicle Casseated pus, debris extend peripherally Subperiosteal abscess-Fascial planes with least resistance Cold abscess Discharging sinus
CLINICAL FEATURES • Pain, swelling, local tenderness with muscle spasm. • Cold abscess with chronic discharging sinus, adhering to underlying bone. • Bony thickening and muscular wasting with constitutional symptoms.
X-ray: • Osteoporosis, outline of articular cortex is lost. • Osteolytic area are granular foci which are surrounded by diffuse osteoporosis. • Osteosclerosis in disease healing and chronic stage. Treatment: As in acute OM along with ATT
Brucellar osteomyelitis Caused by brucella abortis (most common) B. Suis and B. melitensis. It is transmitted through excretion and secretions (milk) of animals to humans.
• More common in the vertebra. • Brucellosis or undulant fever is an uncommon generalised infectious disease • Characterised by acute febrile stage lasting for few days to weeks followed by protracted convalescent or chronic stage over several months or years.
• Characterized by recurring episodes of fever and multiplicity of symptoms. It is during this chronic stage of undulant fever, spine is involved
Clinical Features • • Backpain Recurring fever Loss of weight Sweating at night
O/E: absces formation, palpable in the iliac fossa. • Spinal movements may be full but persisting local pain, local tenderness and muscle spasms may be evident
X-ray: Shows marginal erosion of the body of vertebra with narrowing of_disc space with psoas shadow Lab: ESR raised, brucella aglutination tests positive. Blood culture positive after 2 -3 weeks.
Treatmen: • Streptomycin 2 gram IM daily • Tetracycline 500 mg q. i. d x 2 weeks • Drainage and sequestrectomy can be done
Typhoid osteomyelitis • This is subacute OM of hematogenous origin. • Usually occurring in ulna, ribs, lumbar spine and of diaphyseal region. • Patient with sickle cell anaemia are more prone. • It occurs some months after the attack of typhoid fever
Clinical features: • Pain, On examination tenderness over the affected bone with signs of inflammation X-ray: • Shows central or cortical area of rarefaction with periosteal new bone formation
Lab: Blood culture, culture from the lesion, stool culture, widal test may be positive Treatment: Chloramphenicol(3 -4 gm/day)
Fungal infection of bone • Mycotic OM is a group of rare disease caused by variety of fungus • a)Blastomycosis /Coccidiodomycosis • Usual fungal infections that destroy bone. • Fungi resides in soil and disease is acquired by inhalation of spores. • Onset is insidious and causes mild respiratory infection.
• Most of these patients remain cured but some develop allergic reactions. • Characterised by fever, arthritis, muscle pains. Joints are tender and slightly swollen. • Granulomatous lesion can occur in bones, joints and skin
• Bone lesions are similar with lesions arising in cancellous bone are destructive with little periostitis, bone production/marginal reaction. • Awell defined area of osteolytic destruction is seen.
Treatment: • Amphotericin-B(2 -3 gm)or • 2 -hydroxystilbamidine(8 -12 gm), IV is effective. b)Actinomycosis/Madura mycosis/Sporotrichosis: • May also secondarily affect the bone
OM in HIV disease • Causative organism-S. Aureus, or salmonella or other gram negative organism. • Bones affected are: upper tibia, lower femur, usually bilateral and septic arthritis is common.
Radiology: there is comperative lack of new periosteal bone formation with much necrosis. Treatment: Antibiotic, drainage and immobilization but with a poor prognosis because of decreased immunity.
OM with Implants in-situ • The microorganisms probably grew in biofilm or glycocalyx that adhered to surfaces of biomaterials present. • It is suggested that OM in presence of implants is more resistant to host defence mechanisms and antibiotic treatment.
• If OM develops in healed fracture, implant can be removed. • If the implant is not providing stability, the implant can be removed and fixed with external fixator or stabilized with splint/cast.
It depends on factors • Stage of fracture healing • The amount of stability provided • The amount of time since surgery • Fracture location.
OM IN SPECIFIC SITES
OM of spine - 2 -4% of all cases of OM. - Commonly lumbar spine then thoracic and cervical spine. - Vertebral bodies are usual site. - Simultaneous involvement of 2 adjacent vertebral end plates with intervening disc is usual presentation.
Etiology • Venous return from pelvis- venous plexus of vertebral column. Explains presence of vertebral metastasis in the absence of lung metastasis. • Richly vascular metaphyseal bone near anterior longitudinal ligament correlates with most common site of infection.
• Interroseous artery in children are anastomotic, so because of collateral flow, occlusion of single nutrient artery by septic emboli leads to destruction of only a small portion of bones • In adults these arteries are end arteries so large portion of bone is destroyed.
• Disc is avascular and attacked equally in all ages. • Common spread is from haematogenous spread. • Spinal epidural abscess is monomicrobial (S. aureus common). • Least common sites are occiput, atlas and axis.
Risk Factors • DM, RA. • Urinary, respiratory, dental, vertebral/abdominal sepsis. • Antecedent anterior cervical surgery. • Increasing age.
Diagnosis History and physical examination Significant delay of weeks to months Dramatic localized and regional pain exacerbated by motion/compression is most common Symptom it is excruciatingly persistent despite bed rest. Night pain, fever, anorexia, weight loss.
Physical Examination • Severe PSMS, tenderness, decreased vertebral motion, guarding Lab: • ESR and TC raised. • Blood cultures (during febrile episode)-S. aureus -P. aeruginosa -S. Epidermidis
X-ray: - Earliest finding is disc space narrowing with end plate erosion followed by vertebral body destruction. - Vertebral end plate sclerosis with density in subchondral bone.
- Can ultimately lead to spinal fusion (6 -24 months). - CT, MRI and T 99 scan may be diagnostic. D/D: • Primary neoplasm, TB spine, and metastasis.
Treatment • IV antibiotic treatment (6 wks IV followed by 6 wks oral). • Rest, Spinal immobilisation. • Surgery.
OM in calcaneum • Calcaneum is a spongy bone with a thin periosteum firmly adherent to the bone. • Periosteum is usually perforated rather than elevated by purulent material. • Sequestrum is very rarely formed.
Treatment • Medial and lateral approaches to the calcaneum are satisfactory for incision and drainage of localized abscess • Gaenslen’s approach through the planter surface of the heel is indicated for resecting diseased bone in chronic OM.
Gaenslen’s Approach
CONCLUSION • • • Prevention best High suspicion Early intervention Obtain deep cultures Aggressive debridement
CONCLUSION • • Appropriate antibiotics Early coverage Stabilize appropriate sites Strive for function and cure
THANK YOU
REFERENCES 1. Orthopaedics, Principles and Their Application- Turek 4 th edn. 2. Mercer’s Orthopaedic Surgery`9 th edn. 3. Campbell’s Operative Orthopaedics 10 th edn. 4. Orthopaedic Pathology, Vincent J. Vigorita. 5. Chapman- Operative Orthopaedics.