OSTEOARTHRITIS DEGENERATIVE JOINT DISEASE DEFINITION Osteoarthritis OA is


 is the most common joint disease OA of the knee joint is")
 Most important")


")







 Osteophytes")









 Proteoglycan - Hyaluronic acid - Glycoseaminoglycan Water")

")





 Aerobic exercise programs Physical")


 NSAIDs • • Use generic NSAIDs first If no response")
 inhibitors • • • Pain relief equivalent to")







 Second-line approach • • • NSAIDs if acetaminophen fails Intra-articular")
- Slides: 48
OSTEOARTHRITIS DEGENERATIVE JOINT DISEASE
DEFINITION Osteoarthritis OA is a degenerative joints disease, characterized by Breakdown of articular cartilage and proliferative changes of surrounding bones. Synovial inflammation OA is a chronic disease of the musculoskeletal system, without systemic involvement
EPIDEMIOLOGY Osteoarthritis(OA) is the most common joint disease OA of the knee joint is found in 70% of the population over 60 years of age Radiological evidence of OA can be found in over 90 % of the population
LIMITED FUNCTION OA may cause functional loss Activites of daily living (ADL) Most important cause of disability in old age Major indication for joint replacement surgery
CLASSIFICATION OF OA Primary OA Etiology is unknown Secondary OA Etiology is known
AGE Primary OA > 40 years Direct correlation Aging process
RISK FACTORS FOR PRIMARY OA Age Sex Obesity Genetics Trauma (daily)
SECONDARY OSTOARTHRITIS Trauma Previous joint disorders; Congenital hip dislocation Infection: Septic arthritis, Brucella, Tb Inflammatory: RA Metabolic: Gout Hematologic: Hemophilia Endocrine: DM
ETIOLOGY OF OA Cartilage properties Biomechanical problem
OA: Symptoms and Signs Pain is related to use Pain gets worse during the day Minimal morning stiffness (<20 min) and after inactivity (gelling) Range of motion decreases Joint instability Bony enlargement Deformity – restricition of ADL Restricted movement Crepitus Variable swelling and/or instability
Morphology of Primary OA
Primary Generalized OA
LABORATORY FINDINGS OF OA There are no pathognomonic laboratory findings for OA Laboratory analysis is performed for differential diagnosis
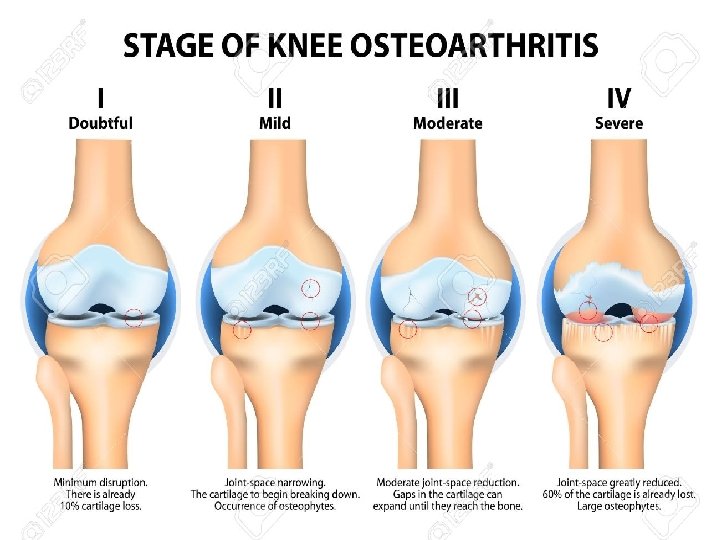
RADIOLOGIC FINDINGS OF OA Narrowing of joint space (due to loss of cartilage) Osteophytes Subchondral (paraarticular) sclerosis Bone cysts
RADIOLOGIC GRADE OF OA G 1 G 2 G 3 G 4 Normal Mild Moderate Severe Kellgren Lawrence Classification
DIAGNOSIS OF OA CLINICAL FINDINGS Joint pain + RADIOLOGIC FINDINGS Osteophytes
OA OF KNEE JOINT More common in obese females over 50 years of age Joint stiffness (<30 minutes) Mechanical pain Physical examination findings: Crepitus Pain on pressure Painful ROM and functional limitation Limitation of ROM in later stages of OA (first extension) Laboratory analysis within normal limits
OA OF HIP JOINT More common in males over 40 years of age Joint stiffness Pain of hip, gluteal and groin areas radiating to the knee Mechanical pain Limited walking function
Hip Osteoarthritis Physical examination: Antalgic limping Limitation of ROM Painful ROM Leg length discrepancy Laboratory analysis within normal limits
X-RAY OF HIP OA
Peripheral Joints Hands Feet
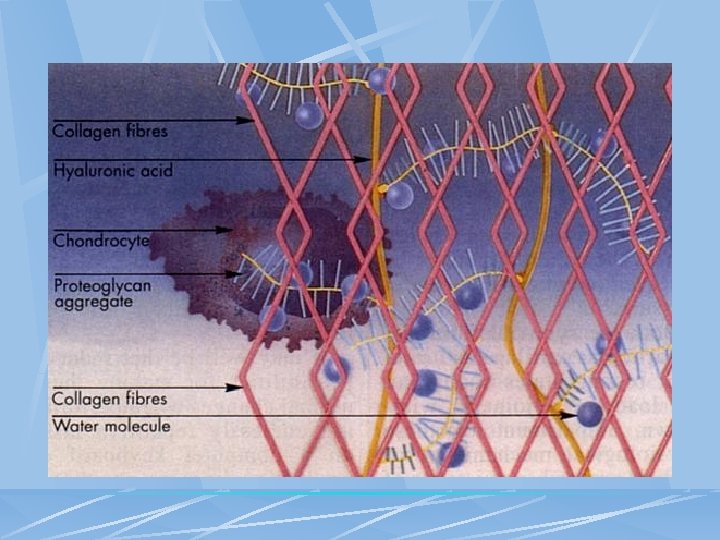
STRUCTURE OF JOINT CARTILAGE Collagen (Type 2) Proteoglycan - Hyaluronic acid - Glycoseaminoglycan Water Condrocyte Regeneration and Degeneration
ETIOPATHOGENESIS OF OA Age, gender Local Genetic biochemical Other factors OA effects
ETIOPATHOGENESIS OF OA Dysfunction of joint cartilage Condrocyte function: 1 - Degredative enzymes (metalloproteases) 2 - Inhibitors Degeneration and regeneration functions are balanced IL-1 , degredative enzymes + synovial inflammation results: Breakdown of cartilage
PATHOGENESIS OF OA Cytokines IL-1, IL-6, TNF- Cell destruction Membrane phospholipids Arachidonic acid Cox-1, Cox-2
IL-1 and metalloproteases have been found to play an important role in cartilage destruction. Local growth factors, especially transforming growth factor (TGF) are involved in the formation of osteophytes
TREATMENT OF OA Symptomatic treatment Structure modifying treatment Surgical treatment
PRIMARY PREVENTION OF OA ? ? Regular exercises Weight control Prevention of trauma
AIMS OF OA TREATMENT Pain relief Preservation and restoration of joint function Education
Non-Pharmacologic Treatment of OA Patient education Weight loss (if overweight) Aerobic exercise programs Physical therapy Range-of-motion exercises Muscle-strengthening exercises Assistive devices for ambulation Appropriate footwear Lateral-wedged insoles Bracing Occupational therapy Joint protection and energy conservation
Pharmacologic Management of OA Non-opioid analgesics Topical agents Intra-articular agents Opioid analgesics NSAIDs Unconventional therapies
Non-opioid Analgesic Therapy First-line—Acetaminophen • • • Pain relief comparable to NSAIDs, less toxicity Beware of toxicity from use of multiple acetaminophen-containing products Maximum safe dose = 4 grams/day
Non-opioid Analgesic Therapy (cont’d) NSAIDs • • Use generic NSAIDs first If no response to one may respond to another Lower doses may be effective Do not retard disease progression Gastroprotection increases expense Side effects: GI, renal, worsening CHF, edema Antiplatelet effects may be hazardous
Non-opioid Analgesics in OA Cyclooxygenase-2 (COX-2) inhibitors • • • Pain relief equivalent to older NSAIDs Probably less GI toxicity Side effects: Renal, edema Older populations with multiple CV medical problems should be tested Cost similar to generic NSAIDs plus proton pump inhibitor or misoprostol
Opioid Analgesics in OA Tramadol • • Affects opioid and serotonin pathways Nonulcerogenic May be added to NSAIDs, acetaminophen Side effects: Nausea, vomiting, lowered seizure threshold, rash, constipation, drowsiness, dizziness
Opioid Analgesics for OA Codeine, oxycodone • Long-acting oxycodone may have fewer CNS side effects Propoxyphene Morphine and fentanyl patches for severe pain interfering with daily activity and sleep
Topical Agents for Analgesia in OA Local cold or heat: Hot packs, hydrotherapy Capsaicin-containing topicals • • Use well supported by evidence Use daily for up to 2 weeks before benefit Compliance poor without full instruction Avoid contact with eyes Liniments = methyl salicylates • Temporary benefit
OA: Intra-articular Therapy Intra-articular steroids • Good pain relief • Most often used in knees, up to q 3 months • With frequent injections; risk infection, worsening diabetes, or CHF Joint lavage • Significant symptomatic benefit demonstrated Hyaluronate injections • Symptomatic relief • Improved function • Require series of injections • No evidence of longterm benefit • Limited to knees • Expensive
OA: Unconventional Therapies Polysulfated glycosaminoglycans— nutriceuticals • Glucosamine +/- chondroitin sulfate: Symptomatic benefit, no known side effects, long-term controlled trials pending Tetracyclines as protease/cytokine inhibitors • • Under study Have disease-modifying potential
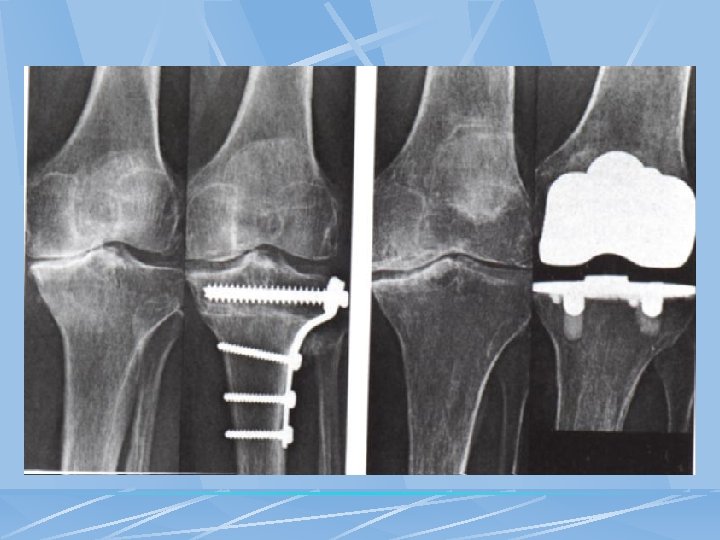
Surgical Therapy for OA Arthroscopy • • • May reveal unsuspected focal abnormalities Results in tidal lavage Expensive, complications possible Osteotomy: May delay need for TKR for 2 to 3 years Total joint replacement: When pain severe and function significantly limited
OA: Management Summary First: Be sure the pain is joint related (not a tendonitis or bursitis adjacent to joint) Initial treatment • • Muscle strengthening exercises and reconditioning walking program Weight loss Acetaminophen first Local heat/cold and topical agents
OA: Management Summary (cont’d) Second-line approach • • • NSAIDs if acetaminophen fails Intra-articular agents or lavage Opioids Third-line • • • Arthroscopy Osteotomy Total joint replacement