Ospedale Papa Giovanni XXIII di Bergamo Dipartimento di

Ospedale Papa Giovanni XXIII di Bergamo Dipartimento di Anestesia e Rianimazione : Direttore F. L. Lorini Management of lung problems during Cardiac Surgery

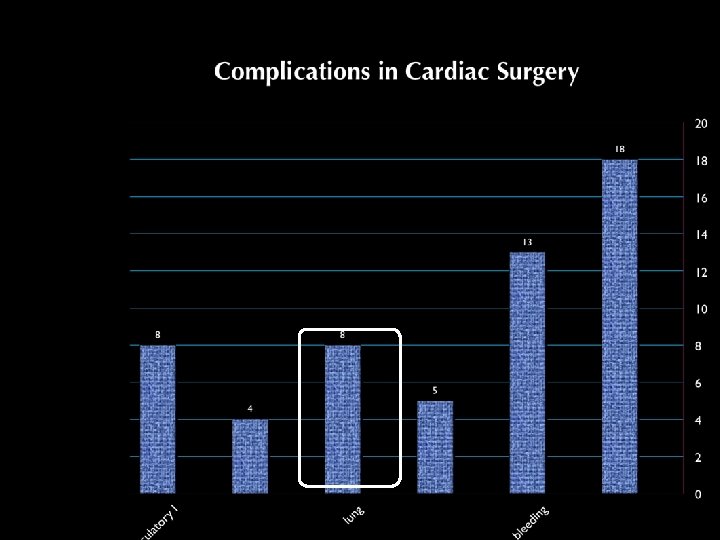
Objectives • Size of the problem and Factors causing pulmonary dysfunction • Definition of diseases • Therapeutic implications
 November 1999 pp 1831 -1839 Early onset of acute pulmonary dysfunction after")
Volume 25(11) November 1999 pp 1831 -1839 Early onset of acute pulmonary dysfunction after cardiovascular surgery: Risk factors and clinical outcome Rady, Mohamed Y. MD, Ph. D, FRCS, MRCP; Ryan, Thomas MB, MRCPI, FFARCSI; Starr, Norman J. MD A total of 3, 122 patients were evaluated and 1, 461 patients satisfied the entry criteria of the study. Early postoperative pulmonary dysfunction was present in 180 (12%) Conclusions: The incidence of early postoperative pulmonary dysfunction is uncommon; however, once developed, it is associated with increased morbidity and mortality after cardiovascular surgery. 4
 November 1999 pp 1831 -1839 Early")
Is There a Pulmonary Problem? • Volume 25(11) November 1999 pp 1831 -1839 Early onset of acute pulmonary dysfunction after cardiovascular surgery: Risk factors and clinical outcome • Rady, Mohamed Y. MD, Ph. D, FRCS, MRCP; Ryan, Thomas MB, MRCPI, FFARCSI; Starr, Norman J. MD • risk factors for early onset of severe pulmonary dysfunction after surgery. v Advanced age v large body mass index v preoperative increased pulmonary arterial pressure v low stroke volume index, hypoalbuminemia v history of cerebral vascular disease v emergency surgery, and prolonged CPB time Postoperative systemic hemodynamics suggest that early postoperative pulmonary dysfunction can be a component of a generalized inflammatory reaction to cardiovascular surgery.

Inflammatory response to CPB 1. Ischemia/Reperfusion 2. Complement activation Endotoxin Proinflammatory cytokines Cellular activation Oxygen free radicals PAF No Arachidonic acid metabolites Endothelins Proteases Tissue injury
 and alveolar")
Ischemia/Reperfusion Representative light microscopic images of lung tissue Alveolar septal thickness (A) and alveolar surface area (B) before CPB and at the end of reperfusion after CPB with or without controlled PA perfusion. 7

Is There a Pulmonary Problem? Do we think about lung protection? Ventilation – stop Perfusion – stop 3% Total lung Bl. Flow (Bronchial Artery) LEAST PROTECTED ORGAN DURING CPB

ALI-ARDS § PCWP < 18 mm. Hg § Pa. O 2/Fi. O 2 < 300 (ALI) § Pa. O 2/Fi. O 2 < 200 (ARDS) § Bilateral infiltrates on chest radiographs

TRALI = Transfusion Related Acute Lung Injury § Acute onset § Within 6 hours after transfusion § ALI characteristics

TRALI Causes: § Packed RBC, FFP, Platelets, granulocytes, cryoprecipitate, IV immunoglobulin , bone marrow stem cells § No Association with washed red cells, albumin, clotting factor concentrates Pathogenesis is not clear : § Ab- mediated TRALI § Non Ab mediated TRALI § Two hits

TRALI Journal of Intensive Care Medicine Volume 23 Number 2 March/April 2008 109121

TRALI § Resolution usually in 96 h after transfusion § Mortality between 5 -10% § Therapy is supportive

TRALI RBC are the major cause of transfusion related side effects Ann Thorac Surg 2009; 88: 1410– 8

TRALI Crit Care Med 2010 Vol. 38, No. 3

Monitoring Vital Parametrs Swan -Ganz RS function Echography Radiology Chemistry
 • Pulmonary hypertension • Valve function")
Echography Heart: • Biventricular funtion ( RV failure) • Pulmonary hypertension • Valve function • Septal defects Lung: • Effusion • Consolidation • PNX

raphy Right Ventricular Function Baseline Recruitment Open lung PEEP Critical Care 2009, 13: R 59

Variation of RV function after CABG in 250 elective patients

Lung-Heart interaction Afterload of RV increase for : § Compression of intralveolar vessel by positive pressure ventilation § Increasing of vasomotor tone § Reduction of vessel tree by reduction of lung parenchyma § Fluid overload ( prexisting and caused by fluid resuscitation) Acidemia Hypercania Hypoxia

Ventilation Recruitment Lung protective ventilation Permissive hypercapnia

Ventilation § TV ≤ 6 ml/Kg IBW (men weight in kg= 50+ 0. 91 *(height in cm-152) (women weight in kg= 45. 5+ 0. 91 *(height in cm-152) § Plateu pressure ≤ 30 cm. H 20 § RF ≤ 35 b/min § PEEP
 there is an evidence of using high PEEP")
PEEP § ALVEOLI, LOVs, EXPRESS ) there is an evidence of using high PEEP in patients with ARDS. May be harmful in patient with ALI § Titration of PEEP is not univocal § Less time to unassisted breath in ARDS patients Current Opinion in Critical Care 2010, 16: 39– 44 JAMA, March 3, 2010—Vol 303, No. 9

PEEP JAMA, March 3, 2010—Vol 303, No. 9

PEEP JAMA, March 3, 2010—Vol 303, No. 9

PEEP ALVEOLI –LOVS high PEEP Fio 2 0. 3 0. 4 0. 5 0. 6 0. 7 0. 8 0. 9 1 PEEP 8 -12 12 -18 18 -20 20 -22 22 22 -24 • Sp 02 between 88%-95%. • Po 2 between 55 mm. Hg-80 mm. Hg. • Ventilation strategies included a protocol for reducing PEEP levels when plateau pressure exceeded 30 -35 cm. H 2 O or when mean arterial pressure decreased to less than 60 mm. Hg. EXPRESS • In the higher PEEP group levels were set to maintain the plateau airway pressure between 28 cm. H 2 O and 30 cm H 2 O. • When the plateau pressure was less than 28 cm H 2 O despite a PEEP level producing a total PEEP of 20 cm H 2 O, PEEP was not increased further • When oxygenation targets were not met despite an Fi. O 2 of 1 and a PEEP level producing a plateau of 30 cm H 2 O, PEEP was increased, provided the plateau pressure remained no greater than 32 cm H 2 O
: CD 006667")
Recruitment Cochrane Database Syst Rev. 2009 Apr 15; (2): CD 006667

Recruitment Am J Respir Crit Care Med Vol 178. pp 1156– 1163, 2008

Recruitment § Sure effect on oxygenation § Outstanding improving of oxygenation may indicate that PEEP is too low § Hypotension and desaturation are self-limited and without serious risk § Few side effect ( barotrauma 1%) § At the moment there is no evidence to use recruitment maneuvers as a routine, reserve it to patients with severe refractory hypoxemia

Recruitment 28 days mortality ICU mortality Cochrane Database of Systematic Reviews 2009, Issue 2. Art. No. :

Recruitment In Hospital Mortality There is no available evidence to determine whether recruitment manoeuvres alter mortality, duration of mechanical ventilation, or hospital stay. Further research is required to determine if recruitment in isolation increase oxygen partial pressure for a longer period of time and whether this has any impact on longerterm outcome. Cochrane Database of Systematic Reviews 2009, Issue 2. Art. No. : CD 006667

Prone Position § Better recruitment of dorsal region § Heart on sternum § Better distribution of ventilation and ventilation /perfusion ratio § Improving on arterial saturation § Advantage in severe hypoxiemic ARDS ( P/F<100) Minerva Anestesiol. 2010 Jun; 76(6): 448 -54 CHEST 2010; 137( 5 ): 1203 – 1216

Prone Position In Gattinoni’s review were take in account 4 studies (Prono-Supine I e II, Mancebo 2006, Guerin 2003 ) Minerva Anestesiol. 2010 Jun; 76(6): 448 -

Prone Position Alsaghir’s review take in account 5 studies with different timing and duration of supination Crit Care Med 2008 Vol. 36, No. 2
")
ECMO V-V 1. In hypoxic respiratory failure due to any cause (primary or secondary) ECLS should be considered when the risk of mortality is 50% or greater, and is indicated when the risk of 80% or greater. a. 50% mortality risk can be identified by a Pa. O 2/Fi. O 2 < 150 on Fi. O 2 > 90% and/or Murray score 2 -3 b. 80% mortality risk can be identified by a Pa. O 2/Fi. O 2 < 80 on Fi. O 2> 90% and Murray score 3 -4 2. CO 2 retention due to asthma or permissive hypercapnia with a Pa. CO 2 > 80 or inability to achieve safe inflation pressures (Pplat ≤ 30 cm HO) is an indication for ECLS. 3. Severe air leak syndromes
 1. Pa. O 2/FIO 2")
The Murray score grading system for ARDS (0 -4) 1. Pa. O 2/FIO 2 at 1 for at least 20 minutes. 2. PEEP in CMH 2 O 3. Lung Compliance in ml/CMH 2 O 4. Number of quadrants with infiltration seen on chest X- ray Score values • Pa. O 2/FIO 2: ≥ 300 = 0, 225– 299 = 1, 175– 224 = 2, 100– 174 = 3, <100 = 4 • CXR: normal = 0, 1 point per quadrant infiltrated. • PEEP: ≤ 5 = 0, 6– 8 = 1, 9– 11 = 2, 12– 14 = 3, ≥ 15 = 4. 36 • Compliance : ≥ 80 = 0, 60– 79 = 1, 40– 59 = 2, 20– 39 = 3, and ≤ 19 = 4

ECMO V-V Considered relative contraindication because of expected poor outcome: 1. Mechanical ventilation at high settings (Fi. O 2 >. 9, P-plat > 30) for 7 days or more 2. Major pharmacologic immunosuppression (absolute neutrophil count <400/ml 3 3. CNS hemorrhage that is recent or expanding

ECMO V-V Criteri per ECMO VV: • Pa. O 2/Fi. O 2<100 con Fi. O 2 100% • P (A-a)>600 mm. Hg • Murray Score > 3 CESAR • Not buffered hypercania p. H < 7, 2 • Respiratory condition with a reversible possibilty • Age < 65 y • No controindication to herapin Lancet Vol 374 Oct 17, 2009

CESAR Trial Lancet Vol 374 Oct 17, 2009

CESAR Trial Lancet Vol 374 Oct 17, 2009

Murray score Lancet Vol 374 Oct 17, 2009 Pa. O 2/FIO 2: ≥ 300 = 0, 225– 299 = 1, 175– 224 = 2, 100– 174 = 3, <100 = 4 CXR: normal = 0, 1 point per quadrant infiltrated. PEEP: ≤ 5 = 0, 6– 8 = 1, 9– 11 = 2, 12– 14 = 3, ≥ 15 = 4. Compliance (ml/cm. H 2 O): ≥ 80 = 0, 60– 79 = 1, 40– 59 = 2, 20– 39 = 3, and ≤ 19 = 4 Sum of the components divided for the number of the components used

Steroids Ventilator free days at day 28 Mortality patients with steroids before 14 days Crit Care Med 2008 Vol. 36, No.
- Slides: 42